Definition of diabetic foot ulcer
Diabetic Foot Ulcer (DFU) - Definition

Key Pathophysiological Components
1. Peripheral Neuropathy
- Sensory neuropathy - loss of light touch and temperature sensation in a glove-and-stocking distribution; patients cannot detect minor cuts, pressure, or injury
- Autonomic neuropathy - reduced skin blood flow, diminished sweating, dry and cracked skin prone to fissuring
- Motor neuropathy - intrinsic foot muscle wasting, leading to deformities (claw toe, hammer toe, fat pad migration) and abnormal plantar pressure distribution
2. Peripheral Vascular Disease
3. Impaired Wound Healing
Clinical Presentation
- Diabetic ulcers most commonly occur at the metatarsal head of the first or fifth toe due to abnormal pressurization from gait changes
- Ischemic ulcers from PAD typically present on the tips of the toes
- Appearance: pink center with granulation tissue and raised edges
- Often painless due to sensory neuropathy - patients frequently do not recall the inciting injury
- Surrounding erythema, purulent drainage, or deep penetration suggests active infection
Epidemiology
- Diabetic patients have a lifetime risk of 15% for developing a DFU, with an annual incidence of 2%
- Medicare patients with a DFU are seen by a healthcare provider an average of 14 times per year and have 1.5 hospitalizations per year
- DFUs are distressingly common and frequently lead to amputation if not managed promptly
In Summary
Peripheral neuropathy and its role in DFU. PPT SLIDE
ls /home/daytona/workspace/ 2>/dev/null || echo "workspace empty or missing"
~/dfu-presentation/peripheral_neuropathy_dfu.js
const pptxgen = require("pptxgenjs");
const pres = new pptxgen();
pres.layout = "LAYOUT_16x9";
pres.title = "Peripheral Neuropathy and Its Role in Diabetic Foot Ulcer";
// ─── COLOR PALETTE ───────────────────────────────────────────────
const DARK_BG = "0D1B2A"; // deep navy (dominant)
const MID_NAVY = "1B2F4E"; // mid navy
const ACCENT = "E87A25"; // amber/orange accent
const ACCENT2 = "4FC3C3"; // teal accent
const WHITE = "FFFFFF";
const LIGHT_GRAY= "C8D6E5";
const RED_WARN = "E84040";
// ═══════════════════════════════════════════════════════════════════
// SLIDE 1 — TITLE SLIDE
// ═══════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
// full dark background
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: DARK_BG } });
// amber accent bar left
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 0.18, h: 5.625, fill: { color: ACCENT } });
// decorative teal circle (abstract neuron)
s.addShape(pres.ShapeType.ellipse, {
x: 7.2, y: 0.4, w: 3.2, h: 3.2,
fill: { type: "solid", color: "1B3F5E" },
line: { color: ACCENT2, width: 2 }
});
s.addShape(pres.ShapeType.ellipse, {
x: 7.8, y: 0.9, w: 2.0, h: 2.0,
fill: { type: "solid", color: "112840" },
line: { color: ACCENT2, width: 1.5 }
});
// nerve "axon" lines inside circle
for (let i = 0; i < 5; i++) {
s.addShape(pres.ShapeType.line, {
x: 8.8, y: 1.9,
w: 0.8 * Math.cos((i * 72 * Math.PI) / 180),
h: 0.8 * Math.sin((i * 72 * Math.PI) / 180),
line: { color: ACCENT, width: 1.5 }
});
}
// title
s.addText("Peripheral Neuropathy", {
x: 0.45, y: 1.0, w: 6.5, h: 0.9,
fontSize: 36, bold: true, color: WHITE, fontFace: "Calibri",
charSpacing: 1
});
s.addText("& Its Role in Diabetic Foot Ulcer", {
x: 0.45, y: 1.9, w: 6.5, h: 0.7,
fontSize: 26, bold: false, color: ACCENT2, fontFace: "Calibri"
});
// subtitle divider
s.addShape(pres.ShapeType.rect, { x: 0.45, y: 2.75, w: 5.5, h: 0.05, fill: { color: ACCENT } });
s.addText("Pathophysiology | Clinical Impact | Management", {
x: 0.45, y: 2.95, w: 6.5, h: 0.5,
fontSize: 14, color: LIGHT_GRAY, fontFace: "Calibri", italic: true
});
s.addText("Source: Fischer's Mastery of Surgery, 8th ed. | Campbell's Operative Orthopaedics, 15th ed.", {
x: 0.45, y: 5.1, w: 9.0, h: 0.4,
fontSize: 9, color: "6A8CAF", fontFace: "Calibri"
});
}
// ═══════════════════════════════════════════════════════════════════
// SLIDE 2 — OVERVIEW: Three Types of Neuropathy
// ═══════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: DARK_BG } });
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 0.9, fill: { color: MID_NAVY } });
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 0.18, h: 5.625, fill: { color: ACCENT } });
s.addText("THREE TYPES OF DIABETIC PERIPHERAL NEUROPATHY", {
x: 0.35, y: 0.1, w: 9.5, h: 0.7,
fontSize: 17, bold: true, color: WHITE, fontFace: "Calibri", charSpacing: 1.5
});
const cards = [
{
x: 0.35, y: 1.05, w: 2.9, h: 3.9,
icon: "S", iconColor: ACCENT,
title: "SENSORY",
bullets: [
"Loss of light touch & temperature",
"Glove-and-stocking distribution",
"Numbness → paresthesias → pain",
"Cannot detect minor cuts or pressure",
"Unnoticed wounds progress to ulcers"
]
},
{
x: 3.55, y: 1.05, w: 2.9, h: 3.9,
icon: "A", iconColor: ACCENT2,
title: "AUTONOMIC",
bullets: [
"Reduced skin blood distribution",
"Decreased sweating & skin oils",
"Dry, cracked, fissured skin",
"Increased susceptibility to breakdown",
"Impaired microvascular regulation"
]
},
{
x: 6.75, y: 1.05, w: 2.9, h: 3.9,
icon: "M", iconColor: RED_WARN,
title: "MOTOR",
bullets: [
"Intrinsic foot muscle wasting",
"Claw toe & hammer toe deformities",
"Fat pad distal migration",
"Abnormal plantar pressure zones",
"Altered gait → ulcer formation"
]
}
];
cards.forEach(c => {
// card background
s.addShape(pres.ShapeType.roundRect, {
x: c.x, y: c.y, w: c.w, h: c.h,
fill: { color: MID_NAVY },
line: { color: c.iconColor, width: 1.5 },
rectRadius: 0.12
});
// icon circle
s.addShape(pres.ShapeType.ellipse, {
x: c.x + 1.05, y: c.y + 0.12, w: 0.75, h: 0.75,
fill: { color: c.iconColor }
});
s.addText(c.icon, {
x: c.x + 1.05, y: c.y + 0.12, w: 0.75, h: 0.75,
fontSize: 20, bold: true, color: WHITE, align: "center", valign: "middle", fontFace: "Calibri"
});
// card title
s.addText(c.title, {
x: c.x + 0.12, y: c.y + 1.0, w: c.w - 0.24, h: 0.42,
fontSize: 13, bold: true, color: c.iconColor, align: "center", fontFace: "Calibri", charSpacing: 2
});
// divider
s.addShape(pres.ShapeType.rect, {
x: c.x + 0.2, y: c.y + 1.45, w: c.w - 0.4, h: 0.04,
fill: { color: c.iconColor }
});
// bullets
s.addText(c.bullets.map((b, i) => ({
text: b,
options: { bullet: { type: "bullet" }, color: LIGHT_GRAY, breakLine: i < c.bullets.length - 1 }
})), {
x: c.x + 0.18, y: c.y + 1.55, w: c.w - 0.36, h: 2.2,
fontSize: 10.5, fontFace: "Calibri", color: LIGHT_GRAY, lineSpacingMultiple: 1.3
});
});
s.addText("Hyperglycemia → Sorbitol accumulation → Vasa nervorum glycosylation → Chronic ischemia → Nerve fiber damage", {
x: 0.35, y: 5.15, w: 9.3, h: 0.35,
fontSize: 9, color: ACCENT, fontFace: "Calibri", italic: true, align: "center"
});
}
// ═══════════════════════════════════════════════════════════════════
// SLIDE 3 — MOLECULAR MECHANISM
// ═══════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: DARK_BG } });
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 0.9, fill: { color: MID_NAVY } });
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 0.18, h: 5.625, fill: { color: ACCENT2 } });
s.addText("MOLECULAR MECHANISMS OF NERVE DAMAGE", {
x: 0.35, y: 0.1, w: 9.5, h: 0.7,
fontSize: 17, bold: true, color: WHITE, fontFace: "Calibri", charSpacing: 1.5
});
// cascade flow: 5 boxes in a horizontal chain
const steps = [
{ label: "Chronic\nHyperglycemia", color: ACCENT },
{ label: "Sorbitol &\nFructose\nAccumulation", color: "E8A025" },
{ label: "Glycosylation of\nVasa Nervorum\nBasement Membrane", color: ACCENT2 },
{ label: "Oxidative\nStress &\nFree Radicals", color: "E84040" },
{ label: "Axonal\nDegeneration &\nNerve Ischemia", color: "B040E8" },
];
const bw = 1.55, bh = 1.25, by = 1.1, gap = 0.28;
steps.forEach((st, i) => {
const bx = 0.35 + i * (bw + gap);
s.addShape(pres.ShapeType.roundRect, {
x: bx, y: by, w: bw, h: bh,
fill: { color: MID_NAVY },
line: { color: st.color, width: 2 },
rectRadius: 0.1
});
s.addText(st.label, {
x: bx, y: by, w: bw, h: bh,
fontSize: 10, bold: true, color: st.color, align: "center", valign: "middle", fontFace: "Calibri"
});
// arrow between boxes
if (i < steps.length - 1) {
s.addShape(pres.ShapeType.rect, {
x: bx + bw, y: by + bh / 2 - 0.04, w: gap, h: 0.08,
fill: { color: "6A8CAF" }
});
}
});
// consequence boxes below
s.addText("DOWNSTREAM CONSEQUENCES", {
x: 0.35, y: 2.6, w: 9.3, h: 0.38,
fontSize: 12, bold: true, color: ACCENT, fontFace: "Calibri", charSpacing: 2
});
const cons = [
{ title: "ATPase Pump\nFailure", detail: "Structural nerve breakdown\n& impaired axonal transport", col: ACCENT },
{ title: "Loss of\nProtective Sensation", detail: "Smallest unmyelinated fibers\naffected first → then larger", col: ACCENT2 },
{ title: "Impaired\nAutonomic Control", detail: "Dry skin, poor circulation,\nincreased fissuring risk", col: RED_WARN },
{ title: "Motor Nerve\nDysfunction", detail: "Intrinsic muscle wasting,\ndeformities, gait change", col: "E8A025" },
];
cons.forEach((c, i) => {
const cx = 0.35 + i * 2.42, cy = 3.1;
s.addShape(pres.ShapeType.rect, {
x: cx, y: cy, w: 2.2, h: 2.1,
fill: { color: "0A1420" },
line: { color: c.col, width: 1 }
});
s.addShape(pres.ShapeType.rect, {
x: cx, y: cy, w: 2.2, h: 0.08,
fill: { color: c.col }
});
s.addText(c.title, {
x: cx, y: cy + 0.12, w: 2.2, h: 0.7,
fontSize: 10, bold: true, color: c.col, align: "center", fontFace: "Calibri"
});
s.addText(c.detail, {
x: cx + 0.1, y: cy + 0.88, w: 2.0, h: 1.1,
fontSize: 9, color: LIGHT_GRAY, fontFace: "Calibri", align: "center", lineSpacingMultiple: 1.3
});
});
}
// ═══════════════════════════════════════════════════════════════════
// SLIDE 4 — HOW NEUROPATHY LEADS TO ULCER
// ═══════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: DARK_BG } });
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 0.9, fill: { color: MID_NAVY } });
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 0.18, h: 5.625, fill: { color: RED_WARN } });
s.addText("HOW NEUROPATHY LEADS TO FOOT ULCERATION", {
x: 0.35, y: 0.1, w: 9.5, h: 0.7,
fontSize: 17, bold: true, color: WHITE, fontFace: "Calibri", charSpacing: 1.5
});
// Vertical pathway in center
const pathway = [
{ step: "1", text: "Chronic hyperglycemia → nerve fiber damage", color: ACCENT },
{ step: "2", text: "Loss of protective sensation (sensory neuropathy)", color: ACCENT },
{ step: "3", text: "Unnoticed repetitive trauma / pressure on foot", color: "E8A025" },
{ step: "4", text: "Muscle wasting → toe deformities → abnormal plantar pressure (motor neuropathy)", color: "E8A025" },
{ step: "5", text: "Dry, cracked, fissured skin (autonomic neuropathy)", color: ACCENT2 },
{ step: "6", text: "Skin breakdown → full-thickness wound = DIABETIC FOOT ULCER", color: RED_WARN },
];
pathway.forEach((p, i) => {
const py = 1.0 + i * 0.7;
// step number circle
s.addShape(pres.ShapeType.ellipse, {
x: 0.35, y: py + 0.05, w: 0.5, h: 0.5, fill: { color: p.color }
});
s.addText(p.step, {
x: 0.35, y: py + 0.05, w: 0.5, h: 0.5,
fontSize: 13, bold: true, color: WHITE, align: "center", valign: "middle", fontFace: "Calibri"
});
// connecting line downward (except last)
if (i < pathway.length - 1) {
s.addShape(pres.ShapeType.rect, {
x: 0.575, y: py + 0.55, w: 0.05, h: 0.2, fill: { color: "6A8CAF" }
});
}
// text box
s.addText(p.text, {
x: 1.0, y: py, w: 8.6, h: 0.6,
fontSize: 12.5, color: i === 5 ? WHITE : LIGHT_GRAY,
bold: i === 5,
fontFace: "Calibri", valign: "middle",
fill: i === 5 ? { color: "2A0A0A" } : undefined,
line: i === 5 ? { color: RED_WARN, width: 1.5 } : undefined
});
});
s.addText("Most common sites: 1st & 5th metatarsal head | Tips of toes (ischemic) | Great toe (pressure)", {
x: 0.35, y: 5.18, w: 9.3, h: 0.33,
fontSize: 9, color: ACCENT2, fontFace: "Calibri", italic: true, align: "center"
});
}
// ═══════════════════════════════════════════════════════════════════
// SLIDE 5 — CLINICAL FEATURES & ASSESSMENT
// ═══════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: DARK_BG } });
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 0.9, fill: { color: MID_NAVY } });
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 0.18, h: 5.625, fill: { color: "4FC3C3" } });
s.addText("CLINICAL FEATURES & ASSESSMENT", {
x: 0.35, y: 0.1, w: 9.5, h: 0.7,
fontSize: 17, bold: true, color: WHITE, fontFace: "Calibri", charSpacing: 1.5
});
// Left column – clinical features
s.addShape(pres.ShapeType.roundRect, {
x: 0.35, y: 1.0, w: 4.4, h: 4.3,
fill: { color: MID_NAVY }, line: { color: ACCENT2, width: 1.5 }, rectRadius: 0.12
});
s.addShape(pres.ShapeType.rect, { x: 0.35, y: 1.0, w: 4.4, h: 0.06, fill: { color: ACCENT2 } });
s.addText("CLINICAL FEATURES", {
x: 0.45, y: 1.08, w: 4.2, h: 0.45,
fontSize: 12, bold: true, color: ACCENT2, fontFace: "Calibri", charSpacing: 2
});
s.addText([
{ text: "Often painless", options: { bullet: true, breakLine: true, bold: true, color: WHITE } },
{ text: " — sensory loss masks injury\n", options: { color: LIGHT_GRAY, breakLine: true } },
{ text: "Pink center with granulation tissue", options: { bullet: true, breakLine: true, color: LIGHT_GRAY } },
{ text: "Raised callused edges", options: { bullet: true, breakLine: true, color: LIGHT_GRAY } },
{ text: "Dry, fissured surrounding skin", options: { bullet: true, breakLine: true, color: LIGHT_GRAY } },
{ text: "Foot deformities (claw toe, hammer toe)", options: { bullet: true, breakLine: true, color: LIGHT_GRAY } },
{ text: "Absent reflexes, reduced vibration sense", options: { bullet: true, breakLine: true, color: LIGHT_GRAY } },
{ text: "Glove-and-stocking sensory loss", options: { bullet: true, color: LIGHT_GRAY } },
], { x: 0.5, y: 1.6, w: 4.1, h: 2.9, fontSize: 11, fontFace: "Calibri", lineSpacingMultiple: 1.4 });
// Right column – assessment tools
s.addShape(pres.ShapeType.roundRect, {
x: 5.0, y: 1.0, w: 4.65, h: 4.3,
fill: { color: MID_NAVY }, line: { color: ACCENT, width: 1.5 }, rectRadius: 0.12
});
s.addShape(pres.ShapeType.rect, { x: 5.0, y: 1.0, w: 4.65, h: 0.06, fill: { color: ACCENT } });
s.addText("ASSESSMENT TOOLS", {
x: 5.1, y: 1.08, w: 4.4, h: 0.45,
fontSize: 12, bold: true, color: ACCENT, fontFace: "Calibri", charSpacing: 2
});
const tools = [
{ name: "Semmes-Weinstein Monofilament", detail: "Screens for peripheral neuropathy; 10-g filament", col: ACCENT },
{ name: "Ankle-Brachial Index (ABI)", detail: "Assesses perfusion; invalid if arteries calcified", col: ACCENT2 },
{ name: "Toe-Brachial Index (TBI)", detail: ">0.4 or toe pressure >40 mmHg = adequate healing", col: ACCENT2 },
{ name: "Probe-to-Bone Test", detail: "Metal probe strikes bone = osteomyelitis likely", col: RED_WARN },
{ name: "MRI Foot", detail: "Most sensitive for osteomyelitis", col: RED_WARN },
];
tools.forEach((t, i) => {
const ty = 1.62 + i * 0.72;
s.addShape(pres.ShapeType.rect, { x: 5.1, y: ty, w: 0.08, h: 0.52, fill: { color: t.col } });
s.addText(t.name, {
x: 5.28, y: ty, w: 4.2, h: 0.3,
fontSize: 10.5, bold: true, color: t.col, fontFace: "Calibri"
});
s.addText(t.detail, {
x: 5.28, y: ty + 0.28, w: 4.2, h: 0.28,
fontSize: 9.5, color: LIGHT_GRAY, fontFace: "Calibri", italic: true
});
});
}
// ═══════════════════════════════════════════════════════════════════
// SLIDE 6 — KEY TAKEAWAYS
// ═══════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: DARK_BG } });
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 0.18, h: 5.625, fill: { color: ACCENT } });
s.addText("KEY TAKEAWAYS", {
x: 0.45, y: 0.3, w: 9.1, h: 0.7,
fontSize: 22, bold: true, color: WHITE, fontFace: "Calibri", charSpacing: 3
});
s.addShape(pres.ShapeType.rect, { x: 0.45, y: 1.0, w: 9.1, h: 0.05, fill: { color: ACCENT } });
const takeaways = [
{ num: "01", text: "Peripheral neuropathy is the single most important risk factor for DFU — present in up to 60% of patients at time of ulceration.", color: ACCENT },
{ num: "02", text: "Three neuropathy types work together: sensory (unnoticed injury), autonomic (skin breakdown), motor (deformity & abnormal pressure).", color: ACCENT2 },
{ num: "03", text: "The molecular root is hyperglycemia → sorbitol accumulation → vasa nervorum glycosylation → chronic nerve ischemia.", color: "E8A025" },
{ num: "04", text: "Painless presentation is a hallmark — patients often cannot identify when or how the wound began.", color: RED_WARN },
{ num: "05", text: "Screening with Semmes-Weinstein monofilament + regular foot inspection is the most effective prevention strategy.", color: "4FC3C3" },
];
takeaways.forEach((t, i) => {
const ty = 1.2 + i * 0.82;
s.addShape(pres.ShapeType.rect, { x: 0.45, y: ty, w: 0.7, h: 0.6, fill: { color: t.color } });
s.addText(t.num, {
x: 0.45, y: ty, w: 0.7, h: 0.6,
fontSize: 16, bold: true, color: DARK_BG, align: "center", valign: "middle", fontFace: "Calibri"
});
s.addText(t.text, {
x: 1.3, y: ty + 0.02, w: 8.3, h: 0.6,
fontSize: 11.5, color: LIGHT_GRAY, fontFace: "Calibri", valign: "middle", lineSpacingMultiple: 1.25
});
});
s.addText("Fischer's Mastery of Surgery, 8th ed. | Campbell's Operative Orthopaedics, 15th ed. 2026 | Mulholland & Greenfield's Surgery, 7th ed.", {
x: 0.45, y: 5.2, w: 9.1, h: 0.3,
fontSize: 8, color: "4A6A8A", fontFace: "Calibri", italic: true
});
}
// ─── WRITE FILE ──────────────────────────────────────────────────
pres.writeFile({ fileName: "/home/daytona/workspace/dfu-presentation/Peripheral_Neuropathy_DFU.pptx" })
.then(() => console.log("✅ PPTX saved successfully"))
.catch(e => console.error("❌ Error:", e));
cd /home/daytona/workspace/dfu-presentation && node peripheral_neuropathy_dfu.js
ls -lh /home/daytona/workspace/dfu-presentation/Peripheral_Neuropathy_DFU.pptx
Peripheral Neuropathy DFU
Presentation · PPTX
| Slide | Content |
|---|---|
| 1 - Title | "Peripheral Neuropathy & Its Role in Diabetic Foot Ulcer" with decorative neuron graphic |
| 2 - Three Types | Side-by-side cards for Sensory, Autonomic, and Motor neuropathy with bullet points for each |
| 3 - Molecular Mechanism | Cascade flow diagram: Hyperglycemia → Sorbitol accumulation → Vasa nervorum glycosylation → Oxidative stress → Axonal degeneration, with 4 downstream consequence boxes |
| 4 - Pathway to Ulcer | Numbered step-by-step flow (6 steps) from nerve damage to DFU formation, with common ulcer sites noted |
| 5 - Clinical Features & Assessment | Two-column layout: left = clinical signs (painless, granulation tissue, deformities), right = assessment tools (Semmes-Weinstein, ABI, TBI, Probe-to-Bone, MRI) |
| 6 - Key Takeaways | 5 numbered takeaways covering prevalence, mechanism, molecular basis, painless presentation, and prevention |
Dont give me in a ppt, i just need it for a slide in ppt. just put it out here
🧠 Peripheral Neuropathy & Its Role in Diabetic Foot Ulcer
What is Diabetic Peripheral Neuropathy?
- Glucose → sorbitol/fructose accumulation → ATPase pump failure
- Glycosylation of vasa nervorum (nerve blood supply) → chronic ischemia
- Mitochondrial oxidative stress → axonal degeneration
Three Types — Each Contributes to Ulcer Formation
| Type | What Happens | How It Causes Ulcers |
|---|---|---|
| Sensory | Loss of touch, temperature, pain sensation (glove-and-stocking pattern) | Patient cannot feel cuts, pressure, or minor injuries — wounds go unnoticed |
| Autonomic | Reduced sweating, decreased skin blood flow | Dry, cracked, fissured skin prone to breakdown |
| Motor | Intrinsic muscle wasting → claw toe, hammer toe, fat pad migration | Abnormal plantar pressure → repeated trauma → ulceration at metatarsal heads |
The Pathway to Ulceration
- Most common sites: 1st & 5th metatarsal head, tips of toes, great toe
- Ulcers are typically painless — patients often cannot recall how the wound started
Key Clinical Points
- Neuropathy is present in up to 60% of patients at time of ulceration
- Semmes-Weinstein 10-g monofilament test screens for loss of protective sensation
- Absent ankle reflexes and reduced vibration sense are early signs
- Foot deformities (claw/hammer toe) signal advanced motor involvement
Glucose → sorbitol/fructose accumulation → ATPase pump failure. how does this leads to neuropathy ?
The Polyol Pathway → ATPase Failure → Neuropathy
Step 1 — Why does glucose enter the polyol pathway?
Step 2 — The Polyol Pathway (Two Enzymatic Steps)
Glucose →(Aldose Reductase)→ Sorbitol →(Sorbitol Dehydrogenase)→ Fructose
uses NADPH uses NAD+
- Aldose reductase converts glucose to sorbitol, consuming NADPH in the process
- Sorbitol is then converted to fructose, consuming NAD+
- Both sorbitol and fructose accumulate inside nerve cells because they cannot easily cross cell membranes
Step 3 — How Sorbitol Accumulation Damages the Nerve
a) Myoinositol depletion (the critical link to ATPase)
- Sorbitol accumulation competitively blocks the uptake of myoinositol (a sugar alcohol essential for nerve cell membrane function) into nerve cells
- Myoinositol is required for the synthesis of phosphatidylinositol, a membrane phospholipid
- Phosphatidylinositol activates protein kinase C (PKC)
- PKC is necessary to drive Na⁺/K⁺-ATPase (the sodium-potassium pump)
b) NADPH depletion → oxidative stress
- NADPH consumed by aldose reductase is also needed to regenerate glutathione (the cell's main antioxidant)
- Less NADPH → less glutathione → oxidative stress builds up inside nerve cells
- Free radicals damage nerve cell membranes, mitochondria, and axonal structures
Step 4 — What Na⁺/K⁺-ATPase Failure Actually Does to Nerves
- Maintaining the resting membrane potential of neurons
- Driving axonal transport (moving proteins and nutrients along the axon)
- Regulating intracellular sodium and potassium balance
| Consequence | Effect |
|---|---|
| Membrane potential disrupted | Impaired nerve conduction velocity (NCV) |
| Axonal transport impaired | Axonal atrophy and "dying-back" degeneration |
| Intracellular Na⁺ builds up | Osmotic swelling, structural breakdown |
| Energy failure | Mitochondrial dysfunction, more free radicals |
Step 5 — Endoneurial Hypoxia Amplifies the Damage
- Further reduces Na⁺/K⁺-ATPase activity (the pump is highly energy-dependent - it consumes ~30% of neuronal ATP)
- Impairs axonal transport even more
- Creates a vicious cycle: hypoxia → more ATPase failure → more axonal degeneration → more hypoxia
The Full Cascade in One View
Chronic Hyperglycemia
↓
Polyol Pathway activated (aldose reductase)
↓
Sorbitol + Fructose accumulate in nerve cells
↓
┌────────────────────────────┐
↓ ↓
Myoinositol depleted NADPH depleted
↓ ↓
PKC activity falls Glutathione falls
↓ ↓
Na⁺/K⁺-ATPase fails Oxidative stress
↓ ↓
└──────────────┬─────────────┘
↓
Axonal atrophy + "dying-back" degeneration
Impaired nerve conduction velocity
Loss of sensation (sensory neuropathy)
Impaired autonomic & motor function
↓
DIABETIC PERIPHERAL NEUROPATHY
Give me an image about it
A detailed medical diagram showing the polyol pathway cascade leading to diabetic peripheral neuropathy. The diagram flows top to bottom with labeled boxes and arrows. Starting with "Chronic Hyperglycemia" at the top, arrow down to "Glucose shunted into Polyol Pathway", then showing the two enzymatic steps: "Glucose → (Aldose Reductase + NADPH) → Sorbitol → (Sorbitol Dehydrogenase + NAD+) → Fructose". Then two branching pathways side by side: Left branch: "Sorbitol accumulates → Blocks Myoinositol uptake → Low Phosphatidylinositol → PKC activity falls → Na+/K+ ATPase pump fails → Axonal transport impaired + Membrane potential disrupted". Right branch: "NADPH depleted → Glutathione falls → Oxidative stress → Free radical damage to nerve membranes and mitochondria". Both branches converge at the bottom to "Endoneurial Hypoxia (vasa nervorum glycosylation)" and finally "Axonal degeneration - dying-back neuropathy - Loss of sensation - Diabetic Peripheral Neuropathy". Include a small inset illustration of a nerve fiber showing demyelination and axonal atrophy. Use a clean clinical style with dark navy blue background, amber and teal accent colors for the two branches, white text labels, and clear directional arrows.
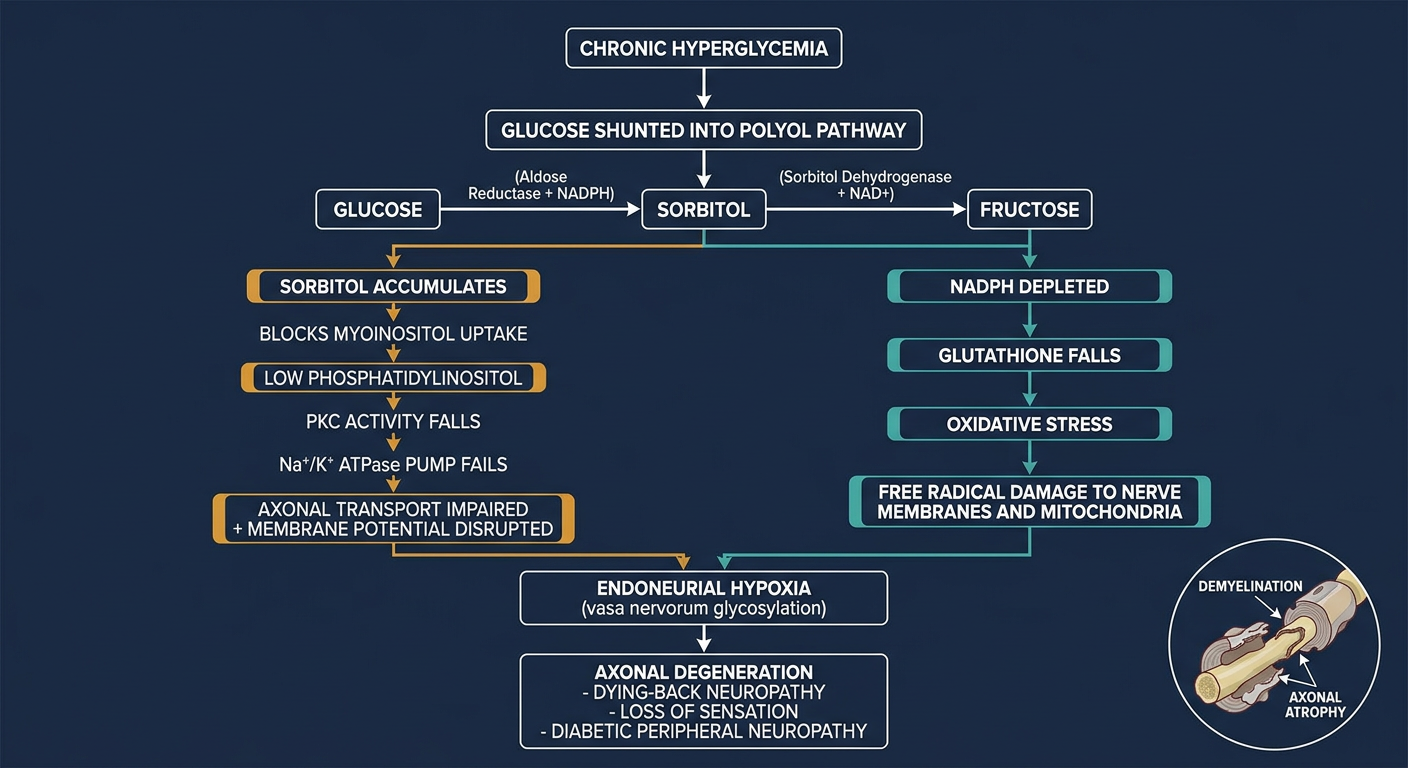
- Left branch (amber) - the Myoinositol → PKC → ATPase failure arm
- Right branch (teal) - the NADPH depletion → oxidative stress arm
- Both converge at endoneurial hypoxia and ultimately axonal degeneration - the structural basis of diabetic peripheral neuropathy
Yes, but put on an image that covers total diabetic neuropathy and its effect on dfu
A comprehensive medical infographic diagram titled "Diabetic Peripheral Neuropathy & Its Role in Diabetic Foot Ulcer". Dark navy blue background, clean clinical style. TOP SECTION - "MOLECULAR MECHANISM (Polyol Pathway)": Chronic Hyperglycemia → Aldose Reductase activates → Glucose converts to Sorbitol + Fructose. Two branches: Left: Sorbitol accumulates → Myoinositol depleted → PKC falls → Na+/K+ ATPase fails → Axonal transport breakdown. Right: NADPH depleted → Glutathione falls → Oxidative stress → Nerve membrane damage. Both arrows point down to: Vasa Nervorum glycosylation → Endoneurial Hypoxia → Axonal degeneration. MIDDLE SECTION - "THREE TYPES OF NEUROPATHY" shown as three columns with icons: Column 1 SENSORY (orange): Loss of pain/touch/temperature sensation, Glove-and-stocking distribution, Cannot feel cuts or pressure Column 2 AUTONOMIC (teal): Reduced sweating, Dry cracked fissured skin, Poor skin blood flow Column 3 MOTOR (red): Intrinsic muscle wasting, Claw toe / Hammer toe, Abnormal plantar pressure, Fat pad migration BOTTOM SECTION - "HOW IT LEADS TO DFU" as a horizontal flow: Unnoticed trauma + Foot deformity + Dry fissured skin → Repeated pressure on metatarsal heads → Skin breakdown → DIABETIC FOOT ULCER (highlighted in red box). Small foot diagram showing common ulcer sites at 1st and 5th metatarsal heads and toe tips. Use amber/orange for sensory, teal for autonomic, red for motor. White text throughout. Bold arrows connecting all sections.
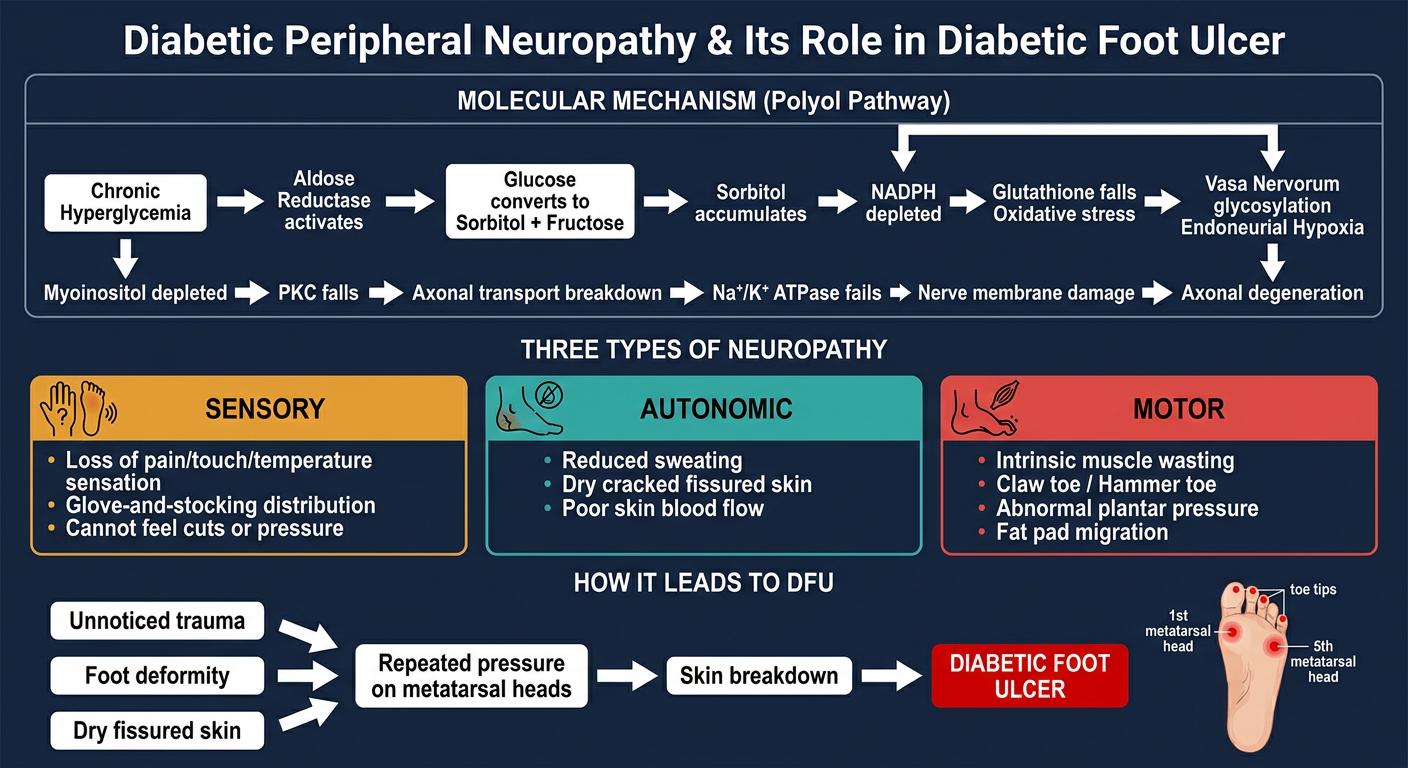
- Top - The molecular polyol pathway cascade (glucose → sorbitol → ATPase failure + oxidative stress → axonal degeneration)
- Middle - The three neuropathy types (Sensory / Autonomic / Motor) with their key effects
- Bottom - How all three converge to cause the diabetic foot ulcer, with common ulcer sites on the foot
lets go into deail about the types of neuropathy
Types of Diabetic Peripheral Neuropathy — In Detail
1. SENSORY NEUROPATHY
What fibers are affected?
| Fiber Type | When Lost | Symptoms |
|---|---|---|
| Small unmyelinated C-fibers | Early | Pain, temperature, light touch lost first |
| Large myelinated A-fibers | Later | Vibration sense, proprioception, deep tendon reflexes lost |
Symptoms — Two Categories
- Numbness and loss of sensation
- Cannot feel heat, cold, or sharp objects
- Loss of balance and proprioception (poor foot placement)
- Absent ankle reflexes
- Burning, tingling, paresthesias
- Shooting or electric pain (especially at night)
- Allodynia — even bedsheets touching the foot feel painful
Why it causes DFU
- Patient cannot detect minor cuts, pressure points, ill-fitting shoes, or foreign objects in footwear
- Repeated unnoticed mechanical trauma on a bony prominence goes uncorrected
- Painful bony pressure points are ignored - no pain signal = no protective withdrawal
- Without off-loading, pressure ulceration develops, most commonly over the 1st or 5th metatarsal head
2. AUTONOMIC NEUROPATHY
Which autonomic functions are damaged?
Sudomotor dysfunction (sweat glands)
- Autonomic signals normally maintain skin oils and moisture
- When autonomic fibers degenerate, sweating is diminished or absent in the feet
- Result: dry, inelastic, cracked skin that fissures easily at the heels and between toes
- Fissures become portals of entry for bacteria
Vasomotor dysfunction (blood vessel control)
- Autonomic nerves regulate the precapillary sphincters that distribute blood to skin
- Loss of vasomotor tone causes arteriovenous shunting - blood bypasses capillaries and goes directly through AV shunts
- The skin is actually warm and well-perfused at rest, but the microcirculation is dysregulated
- This is why a diabetic foot can have bounding pulses yet still ulcerate - the microvascular nutritive flow to skin is impaired
Other autonomic manifestations beyond the foot:
- Postural hypotension
- Gastroparesis, diarrhoea, constipation
- Bladder dysfunction (incomplete emptying → recurrent infections)
- Sexual dysfunction
- Cardiac arrhythmias
- Pupillary abnormalities
Why it causes DFU
- Dry, fissured skin has dramatically reduced barrier function
- Small cracks at pressure sites quickly become full-thickness wounds
- Impaired local blood flow regulation means wound healing is further impaired
3. MOTOR NEUROPATHY
What gets damaged?
The Biomechanical Cascade
Intrinsic muscle wasting (lumbricals, interossei)
↓
Extrinsic muscles (long flexors/extensors) now unopposed
↓
Toe deformities develop:
• Hammer toe (PIP joint flexion contracture)
• Claw toe (MTP hyperextension + IP flexion)
• Mallet toe
↓
Fat pad migrates distally (normally cushions metatarsal heads)
↓
Metatarsal heads become exposed and unpadded
↓
Gastrocnemius-soleus contracture → increased forefoot force load
↓
Abnormally high plantar pressure at metatarsal heads + toe tips
↓
Callus formation → if not managed → sub-callus ulceration
Gait Changes
- Decreased proprioception → wider step width for balance
- Slower walking speed
- Abnormal weight distribution → peak pressure shifts to vulnerable bony prominences
Why it causes DFU
- Structural deformity creates focal pressure points that exceed tissue tolerance
- The combination of deformity + insensate foot = pressure applied repetitively without any protective response
- Classic sites: 1st metatarsal head (most common), 5th metatarsal head, under hammer/claw toes
How All Three Types Work Together
SENSORY AUTONOMIC MOTOR
↓ ↓ ↓
Cannot feel Dry, fissured Deformity +
the damage skin abnormal pressure
└──────────────────┴────────────────┘
↓
Repetitive unnoticed trauma
on structurally vulnerable,
poorly lubricated skin
↓
DIABETIC FOOT ULCER
Histopathology (What the Nerve Actually Looks Like)
- Reduced number of myelinated axons (especially large fibers)
- Active axonal degeneration with degenerating myelin sheaths
- Regenerative axonal clusters (failed repair attempts)
- Endoneurial arterioles show: thickened walls, hyalinization, PAS-positive basement membrane reduplication
- Dropout of small unmyelinated C-fibers in skin biopsies - correlates directly with symptom severity
Generate a visual diagram showing all three neuropathy types and how they converge to cause DFU
A detailed medical convergence diagram titled "Three Types of Diabetic Peripheral Neuropathy Converging to Cause Diabetic Foot Ulcer". Dark navy blue background, clean clinical infographic style, white text. TOP: Large centered box labeled "DIABETIC PERIPHERAL NEUROPATHY" with subtitle "Chronic Hyperglycemia → Nerve Fiber Damage" in amber color. MIDDLE SECTION: Three tall vertical columns, each with a distinct color theme, separated by space: LEFT COLUMN - orange/amber theme - titled "SENSORY NEUROPATHY": - Icon: nerve with dotted lines (sensation loss symbol) - Bullet points: • Small C-fibers lost first (pain, temperature) • Large A-fibers lost later (vibration, proprioception) • Glove-and-stocking distribution • Positive symptoms: burning, tingling, shooting pain • Negative symptoms: numbness, absent ankle reflexes - Red warning box at bottom: "CANNOT FEEL cuts, pressure, trauma, foreign objects in shoe" MIDDLE COLUMN - teal theme - titled "AUTONOMIC NEUROPATHY": - Icon: sweat droplet with X - Bullet points: • Sudomotor failure → no sweating • Vasomotor dysfunction → AV shunting • Skin oils depleted • Dry, cracked, fissured skin • Impaired microcirculation • Reduced skin barrier function - Red warning box at bottom: "Skin FISSURES become entry points for bacteria" RIGHT COLUMN - red theme - titled "MOTOR NEUROPATHY": - Icon: foot bone diagram - Bullet points: • Intrinsic muscle wasting • Extrinsic muscles unopposed • Hammer toe, claw toe deformities • Fat pad migrates distally • Metatarsal heads exposed • Gastrocnemius contracture → forefoot overload • Abnormal gait, wider step width - Red warning box at bottom: "PEAK PRESSURE at metatarsal heads and toe tips" CONVERGENCE SECTION: Three large arrows from each column converging downward into a central funnel shape, with labels on the arrows: "Unnoticed trauma" (from sensory), "Skin breakdown" (from autonomic), "Structural deformity" (from motor). BOTTOM: Large highlighted box in deep red with white bold text: "DIABETIC FOOT ULCER" with sub-labels showing common sites: "1st & 5th metatarsal head | Toe tips | Great toe | Heel fissures". Small anatomical foot outline showing ulcer locations marked with red dots. Use clean sans-serif fonts, bold section headers, clear arrows, consistent icon style throughout.
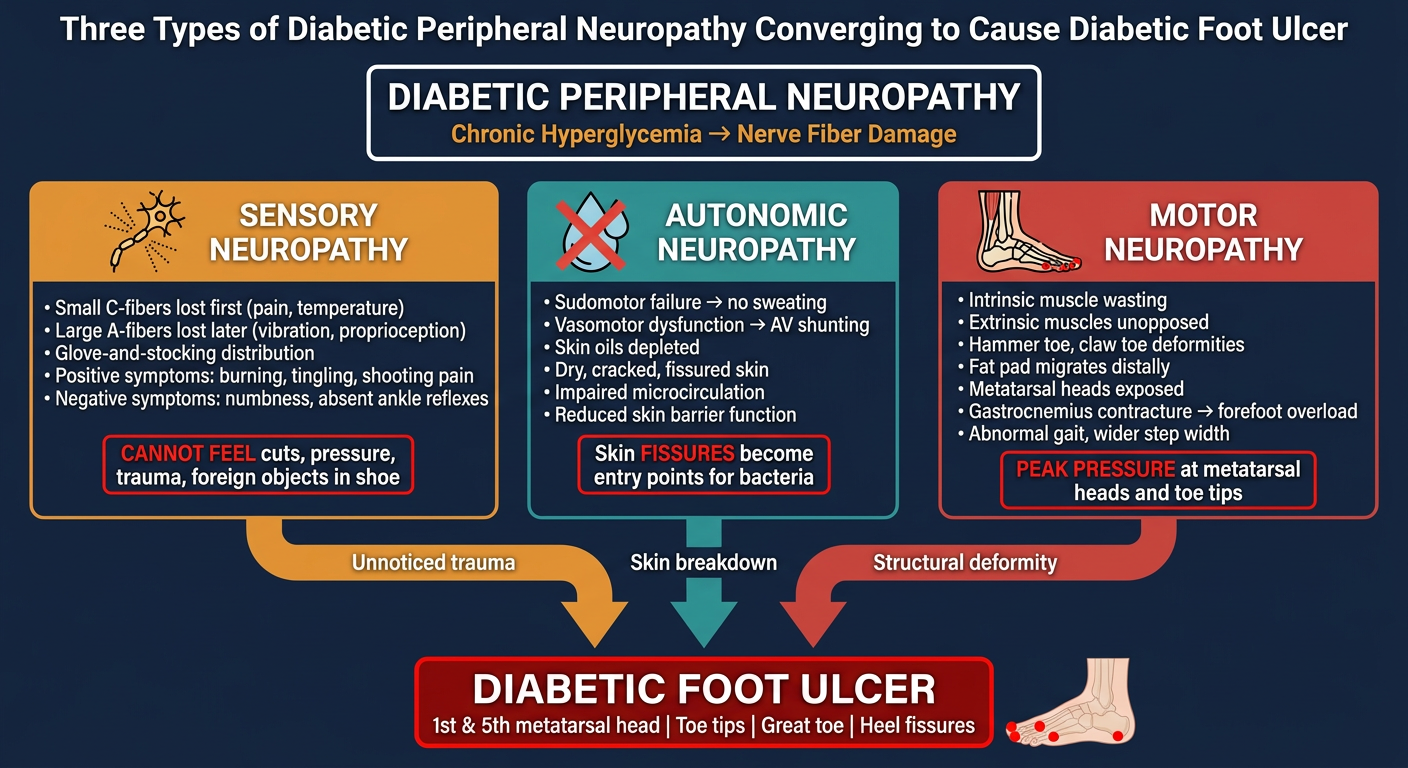
- Top - Diabetic Peripheral Neuropathy as the root cause
- Three columns - Sensory (amber), Autonomic (teal), Motor (red) - each with their specific mechanisms and consequences
- Convergence arrows - labeled with the specific contribution of each type (unnoticed trauma / skin breakdown / structural deformity)
- Bottom - Diabetic Foot Ulcer as the common endpoint, with an anatomical foot marking the classic ulcer sites
what is glove and stocking distribution ?
Glove-and-Stocking Distribution
The Core Concept
- The feet and lower legs - like a pair of stockings pulled up to the knees
- The hands and forearms - like a pair of gloves covering the hands
Why Does It Happen in This Pattern? — The Length-Dependent Principle
Spinal cord → Sciatic nerve → Tibial nerve → Plantar nerves → Toe tips
(longest axons in the body — up to 1 metre)
- The toes and feet are at the far end of the longest axons in the body → affected first and most severely
- As disease progresses, the boundary ascends up the leg toward the knee
- When leg involvement reaches roughly mid-calf level, the hands start to be affected (because the hand axons are now the same length as the affected leg axons)
- In severe disease, the boundary continues to ascend toward the thigh, and even the anterior trunk (abdomen, thorax) can be affected in extreme cases
The Shape of the Sensory Loss
Normal sensation
↓
Slightly reduced
↓
Moderately reduced ← mid-calf / mid-forearm (ascending border)
↓
Severely reduced
↓
Complete sensory loss ← toes, feet, fingertips
What Sensations Are Lost? — Depends on Which Fibers Are Hit
| Fiber Type | Sensation Carried | Lost in DPN? | When? |
|---|---|---|---|
| Small unmyelinated C-fibers | Pain, temperature | Yes | Early |
| Small myelinated Aδ-fibers | Sharp pain, cold | Yes | Early |
| Large myelinated Aβ-fibers | Light touch, vibration, proprioception | Yes | Later |
- They cannot feel a hot water bottle burning their foot
- They cannot feel a nail inside their shoe
- But early on, they may still feel vibration with a tuning fork
Visual Summary
NORMAL AFFECTED
Head: ✅ ✅ (spared in most cases)
Trunk: ✅ ✅ (spared except severe cases)
Upper thighs: ✅ ✅
─────────────────────────────────── ← ascending border (late disease)
Mid-thigh: ✅ ⚠️ (very severe only)
─────────────────────────────────── ← ascending border (mid disease)
Knee: ✅ ⚠️
─────────────────────────────────── ← ascending border (early disease)
Lower leg: ✅ ❌ "STOCKING"
Foot: ✅ ❌ "STOCKING" (worst here)
Toes: ✅ ❌ (first affected)
Forearm: ✅ ❌ "GLOVE" (when leg disease is mid-shin)
Hand: ✅ ❌ "GLOVE"
Fingers: ✅ ❌ (first in upper limbs)
Other Causes of Glove-and-Stocking Distribution
- Chronic alcohol use
- Vitamin B12 deficiency
- Chemotherapy toxicity (paclitaxel, vincristine)
- Chronic kidney disease (uraemic neuropathy)
- HIV-associated neuropathy
- Arsenic/heavy metal poisoning
- Guillain-Barré syndrome (though this is ascending and acute)
Relevance to DFU
Do a image like that for PAD and infection too ?
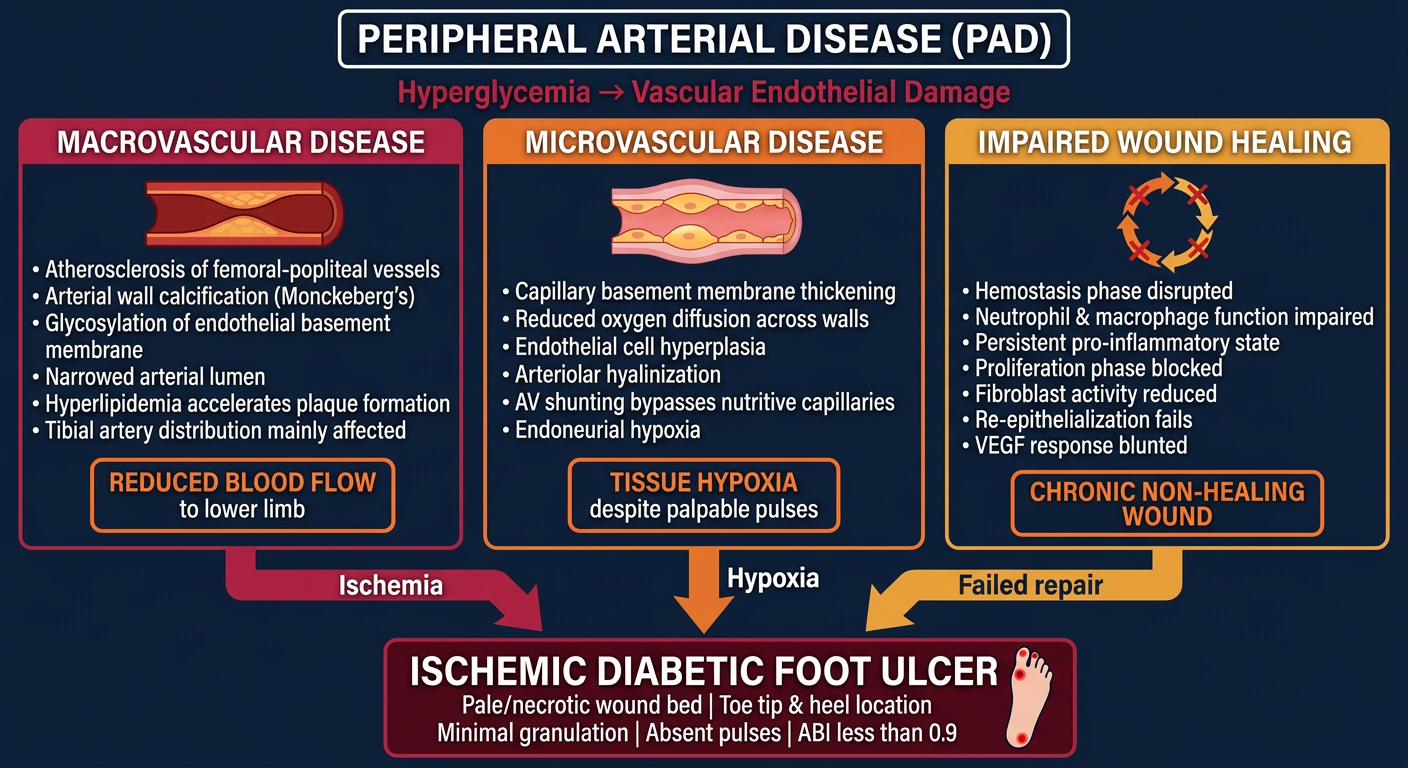
A detailed medical convergence diagram titled "Peripheral Arterial Disease (PAD) in Diabetic Foot Ulcer". Dark navy blue background, clean clinical infographic style, white text. TOP: Large centered box labeled "PERIPHERAL ARTERIAL DISEASE (PAD)" with subtitle "Hyperglycemia → Vascular Endothelial Damage" in deep red/crimson color. MIDDLE SECTION: Three tall vertical columns with distinct color themes: LEFT COLUMN - crimson/red theme - titled "MACROVASCULAR DISEASE": - Icon: narrowed artery cross-section - Bullet points: • Atherosclerosis of femoral-popliteal vessels • Arterial wall calcification (Monckeberg's) • Glycosylation of endothelial basement membrane • Narrowed arterial lumen • Hyperlipidemia accelerates plaque formation • Tibial artery distribution mainly affected - Orange warning box at bottom: "REDUCED BLOOD FLOW to lower limb" MIDDLE COLUMN - orange theme - titled "MICROVASCULAR DISEASE": - Icon: capillary with thickened wall - Bullet points: • Capillary basement membrane thickening • Reduced oxygen diffusion across walls • Endothelial cell hyperplasia • Arteriolar hyalinization • AV shunting bypasses nutritive capillaries • Endoneurial hypoxia - Orange warning box at bottom: "TISSUE HYPOXIA despite palpable pulses" RIGHT COLUMN - amber/yellow theme - titled "IMPAIRED WOUND HEALING": - Icon: broken wound healing cycle - Bullet points: • Hemostasis phase disrupted • Neutrophil & macrophage function impaired • Persistent pro-inflammatory state • Proliferation phase blocked • Fibroblast activity reduced • Re-epithelialization fails • VEGF response blunted - Orange warning box at bottom: "CHRONIC NON-HEALING WOUND" CONVERGENCE SECTION: Three bold arrows from each column converging downward with labels: "Ischemia" (from macro), "Hypoxia" (from micro), "Failed repair" (from healing). BOTTOM: Large highlighted box in dark crimson with white bold text: "ISCHEMIC DIABETIC FOOT ULCER" with features listed: "Pale/necrotic wound bed | Toe tip & heel location | Minimal granulation | Absent pulses | ABI less than 0.9". Small foot outline showing ulcer locations at toe tips and heel marked with red dots. Clean sans-serif fonts, bold headers, consistent icon style, clear arrows.
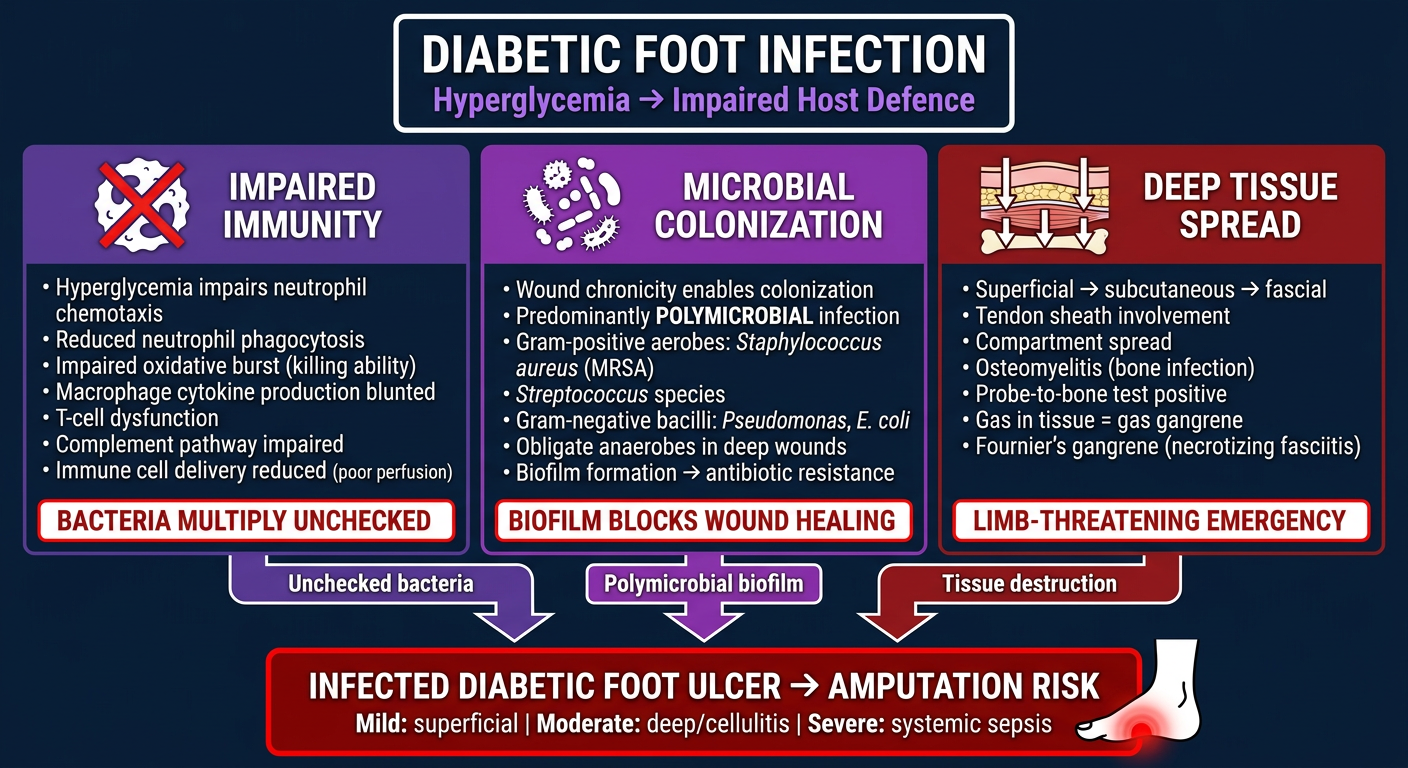
A detailed medical convergence diagram titled "Infection in Diabetic Foot Ulcer". Dark navy blue background, clean clinical infographic style, white text. TOP: Large centered box labeled "DIABETIC FOOT INFECTION" with subtitle "Hyperglycemia → Impaired Host Defence" in purple/violet color. MIDDLE SECTION: Three tall vertical columns with distinct color themes: LEFT COLUMN - purple theme - titled "IMPAIRED IMMUNITY": - Icon: white blood cell with X - Bullet points: • Hyperglycemia impairs neutrophil chemotaxis • Reduced neutrophil phagocytosis • Impaired oxidative burst (killing ability) • Macrophage cytokine production blunted • T-cell dysfunction • Complement pathway impaired • Immune cell delivery reduced (poor perfusion) - Red warning box at bottom: "BACTERIA MULTIPLY UNCHECKED" MIDDLE COLUMN - violet/magenta theme - titled "MICROBIAL COLONIZATION": - Icon: bacteria cluster - Bullet points: • Wound chronicity enables colonization • Predominantly POLYMICROBIAL infection • Gram-positive aerobes: Staphylococcus aureus (MRSA) • Streptococcus species • Gram-negative bacilli: Pseudomonas, E. coli • Obligate anaerobes in deep wounds • Biofilm formation → antibiotic resistance - Red warning box at bottom: "BIOFILM BLOCKS WOUND HEALING" RIGHT COLUMN - dark red theme - titled "DEEP TISSUE SPREAD": - Icon: layers of tissue with arrows going deeper - Bullet points: • Superficial → subcutaneous → fascial • Tendon sheath involvement • Compartment spread • Osteomyelitis (bone infection) • Probe-to-bone test positive • Gas in tissue = gas gangrene • Fournier's gangrene (necrotizing fasciitis) - Red warning box at bottom: "LIMB-THREATENING EMERGENCY" CONVERGENCE SECTION: Three bold arrows converging downward labeled: "Unchecked bacteria" (from immunity), "Polymicrobial biofilm" (from colonization), "Tissue destruction" (from spread). BOTTOM: Large highlighted box in deep red with white bold text: "INFECTED DIABETIC FOOT ULCER → AMPUTATION RISK" with IDSA severity listed: "Mild: superficial | Moderate: deep/cellulitis | Severe: systemic sepsis". Small foot outline with spreading red zone indicating infection spread. Clean sans-serif fonts, bold headers, consistent icon style, urgent warning visual feel.
PAD in Diabetic Foot Ulcer
Infection in Diabetic Foot Ulcer
- Neuropathy - the silent enabler
- PAD - the ischemic driver
- Infection - the limb-threatening complication
EXPLAIN ME ABOUT PAD AND INFECTION
PART 1 — PERIPHERAL ARTERIAL DISEASE (PAD) IN DFU
What is PAD in Diabetes?
Macrovascular Disease — The Large Vessel Problem
How Hyperglycemia Damages Large Arteries
- Glycosylation of endothelial basement membrane - glucose attaches to proteins in the arterial wall, forming Advanced Glycation End Products (AGEs), which stiffen and thicken vessel walls, reducing oxygen diffusion
- Atherosclerosis - hyperlipidemia (common in diabetes) accelerates plaque formation in artery walls, progressively narrowing the lumen
- Arteriosclerosis and Monckeberg's calcification - calcium deposits harden the arterial wall, making vessels stiff and noncompressible — this is why ABI readings are often falsely elevated or invalid in diabetic patients
- Endothelial AGE receptor ligation - triggers release of pro-inflammatory cytokines and activates the coagulation cascade, promoting thrombosis
Which Vessels Are Affected?
- Tibial arteries (anterior and posterior tibial, peroneal) - the vessels supplying the foot directly
- Femoral-popliteal distribution - the thigh and knee-level vessels
Microvascular Disease — The Small Vessel Problem
- Capillary basement membrane thickens and duplicates → oxygen cannot diffuse freely across the wall to tissues
- Endothelial cell hyperplasia narrows capillary lumens
- Arteriolar hyalinization - walls become glassy and lose elasticity
- AV shunting - blood bypasses nutritive capillaries entirely, going through arteriovenous shunts directly to veins
- Result: tissue receives inadequate oxygen despite apparently warm, well-perfused skin
How PAD Kills Wound Healing
| Stage | What Needs Oxygen | What Happens in PAD |
|---|---|---|
| Hemostasis | Platelet aggregation | Relatively preserved |
| Inflammation | Neutrophil/macrophage activity | Impaired — cells cannot reach wound |
| Proliferation | Fibroblast activity, VEGF, angiogenesis | Severely impaired - hypoxia blocks VEGF response |
| Remodeling | Collagen synthesis | Fails - insufficient oxygen for fibroblasts |
Clinical Features of Ischemic DFU
| Feature | Ischemic Ulcer | Neuropathic Ulcer |
|---|---|---|
| Location | Toe tips, heel, lateral foot | Metatarsal heads, plantar surface |
| Pain | Painful (rest pain, claudication) | Painless |
| Wound bed | Pale, necrotic, sloughy | Pink with granulation tissue |
| Surrounding skin | Cool, hairless, shiny atrophic skin | Dry, callused, warm |
| Pulses | Absent/diminished | Present |
| Edges | Punched-out | Callused raised edges |
Assessment of PAD in DFU
- Ankle-Brachial Index (ABI) - compares ankle to arm blood pressure; ABI <0.9 = PAD; but in diabetes, arterial calcification makes vessels noncompressible → falsely normal or elevated ABI
- Toe-Brachial Index (TBI) - more reliable in diabetics; TBI >0.4 or toe pressure >40 mmHg = adequate perfusion for healing
- Transcutaneous oxygen tension (TcPO2) - direct measure of skin oxygenation
- Patients without adequate perfusion → referred to vascular surgeon for revascularization before aggressive debridement
⚠️ Critical rule: Aggressive wound debridement must NOT be performed until adequate perfusion is confirmed — without blood supply, debridement creates a larger wound that cannot heal.
PART 2 — INFECTION IN DFU
Why Diabetic Patients Are Uniquely Susceptible to Infection
1. Impaired Immune Defence
| Immune Cell | Normal Function | In Diabetes |
|---|---|---|
| Neutrophils | Chemotaxis → site of infection | Impaired migration to wound |
| Neutrophils | Phagocytosis of bacteria | Reduced phagocytic killing |
| Neutrophils | Oxidative burst (ROS killing) | Blunted due to hyperglycemia |
| Macrophages | Cytokine production | Impaired in hyperglycemic state |
| T-cells | Adaptive immunity | Dysfunction with prolonged hyperglycemia |
- Vascular compromise additionally reduces delivery of immune cells and antibiotics to the infection site
- The complement system is also impaired in diabetes
2. The Wound as a Perfect Bacterial Habitat
- Moist, warm, protein-rich environment
- Necrotic tissue - acts as culture medium
- Poor perfusion - immune cells and antibiotics cannot penetrate
- Continuous bacterial re-inoculation from skin flora and environment
- Result: biofilm formation - bacteria surround themselves in a protective polysaccharide matrix, dramatically increasing resistance to antibiotics and phagocytosis
Microbiology — What Is Growing in the Wound?
| Organism Type | Common Species | Prevalence |
|---|---|---|
| Gram-positive aerobes | S. aureus (including MRSA), Streptococcus spp. | Most prevalent overall |
| Gram-negative bacilli | Pseudomonas aeruginosa, E. coli, Proteus | Moderate |
| Obligate anaerobes | Bacteroides, Peptostreptococcus | Deep/necrotic wounds, especially chronic |
Key point: Superficial wound swabs are unreliable and should NOT be performed - they grow skin colonizers, not the true pathogens. Only deep tissue culture or bone biopsy culture gives clinically meaningful results.
Depth of Infection — The Progression
Skin surface (colonization — all chronic wounds)
↓
Superficial infection (cellulitis — erythema, warmth, swelling)
↓
Deep soft tissue infection (fascia, tendon sheath involvement)
↓
Abscess formation (pus collection — needs surgical drainage)
↓
Osteomyelitis (bone infection — present in 67% of ulcers that reach bone)
↓
Gas gangrene / Necrotizing fasciitis (surgical emergency)
↓
Pedal sepsis → systemic sepsis → multi-organ failure
Osteomyelitis — The Most Feared Complication
Diagnosis
| Test | Sensitivity | Specificity | Notes |
|---|---|---|---|
| Probe-to-bone test | 60% | 91% | PPV ~90% in high pretest probability; sterile metal probe clicks on bone |
| Plain X-ray | 30-50% | 50-90% | Low sensitivity; useful for follow-up |
| MRI | 80-100% | 80-90% | Most sensitive; first-line imaging for osteomyelitis |
| WBC scan (Tc/In) | High | High | Used when MRI unavailable; better than Tc alone |
| Bone biopsy | Gold standard | Gold standard | Invasive; gives organism + sensitivities |
Lab markers (non-specific but supportive):
- ESR >70 mm/hr = 11-fold greater risk of osteomyelitis
- Elevated CRP supports diagnosis
IDSA Classification of DFU Infection Severity
| Grade | Description | Management |
|---|---|---|
| Mild | Superficial, cellulitis <2cm, no systemic features | Oral antibiotics, outpatient |
| Moderate | Deep infection (fascia, tendon, bone) OR cellulitis >2cm, no systemic features | IV antibiotics, possible hospitalisation |
| Severe | Any infection + systemic features (fever, tachycardia, hypotension, leukocytosis, metabolic acidosis) | Hospitalise immediately, IV broad-spectrum antibiotics, urgent surgical consultation |
Pedal Sepsis — The Surgical Emergency
- Fever, tachycardia, hypotension
- Altered mental status, metabolic acidosis
- End-organ failure
Antibiotic Principles
- Mild infection - oral agent active against gram-positive cocci (S. aureus, Streptococcus); include MRSA coverage if risk factors present (vancomycin)
- Moderate-severe - broad spectrum IV coverage; if prior antibiotics → include gram-negatives (clindamycin + fluoroquinolone); Pseudomonas risk → piperacillin-tazobactam or cefepime
- Osteomyelitis - antibiotic duration: 4-6 weeks if infected bone not fully removed; 3 weeks post-surgical debridement; guided by bone biopsy culture
The Full DFU Triad — How PAD and Infection Connect
NEUROPATHY PAD INFECTION
↓ ↓ ↓
Unnoticed Ischemia → failed Impaired immunity
trauma wound healing + chronic wound
↓ ↓ ↓
──────── DIABETIC FOOT ULCER ────────
↓
Bacteria colonize
↓
Biofilm → deep spread
↓
Osteomyelitis / Sepsis
↓
AMPUTATION
What is probe to bone test ?
The Probe-to-Bone Test
What It Is
How to Perform It
- Take a sterile blunt metal probe (a stainless-steel instrument, similar to a dental probe)
- Insert it gently into the depth of the wound
- Advance it carefully through the wound tissue
- Assess what you feel at the base:
| Finding | Interpretation |
|---|---|
| Hard, gritty, rock-solid surface with no intervening soft tissue | POSITIVE - bone reached = osteomyelitis highly likely |
| Soft tissue throughout - no hard surface | NEGATIVE - bone not reached |
Diagnostic Performance
| Statistic | Value | Source |
|---|---|---|
| Sensitivity | 60-87% | Varies by study |
| Specificity | 83-91% | |
| Positive Predictive Value (PPV) | ~90% in high pretest probability | Harrison's, 22nd ed. |
| Likelihood Ratio (negative test) | 0.2 | Osteomyelitis becomes unlikely if negative |
- Positive PTB in a hospitalized diabetic with a chronic deep foot ulcer = ~90% chance of osteomyelitis - essentially diagnostic without imaging
- Negative PTB significantly reduces the probability of osteomyelitis (LR 0.2) but does not exclude it - MRI is still needed if clinical suspicion remains
When to Use It — Context Matters
- Hospitalized diabetic patient
- Chronic, deep, non-healing foot ulcer
- Ulcer larger than 2 cm
- ESR >70 mm/hr
- Recurrent or deepening ulcer
Why It Works — The Pathological Basis
- Infection tracks contiguously from skin → soft tissue → periosteum → cortical bone
- 67% of DFU that probe to bone have confirmed osteomyelitis on imaging or biopsy
- The direct continuity between ulcer and infected bone means a metal probe can physically reach the bone surface through the wound tract
How It Fits Into the Diagnostic Workup
Diabetic patient with foot ulcer
↓
Perform Probe-to-Bone test
↓
┌───────┴───────┐
POSITIVE NEGATIVE
↓ ↓
High pretest? Clinical suspicion still high?
↓ ↓
YES YES
↓ ↓
Diagnose MRI foot
osteomyelitis (sensitivity 80-100%)
+ confirm with ↓
MRI if needed Still unclear?
↓
Bone biopsy (GOLD STANDARD)
+ culture for antibiotic guidance
PTB vs. Other Diagnostic Tests for DFU Osteomyelitis
| Test | Sensitivity | Specificity | Practical Use |
|---|---|---|---|
| Probe-to-bone | 60-87% | 83-91% | First-line bedside test |
| Plain X-ray | 30-50% | 50-90% | Cheap, easy; misses early disease |
| MRI | 80-100% | 80-90% | Best imaging; first-line if PTB equivocal |
| WBC scan (Tc/In) | High | High | When MRI unavailable or contraindicated |
| Bone biopsy | Gold standard | Gold standard | Definitive - gives organism + sensitivities |
Combined Diagnostic Approach
- Positive probe-to-bone test
- Elevated inflammatory markers (ESR >70, raised CRP)
- Abnormal plain radiograph (bone erosion, periosteal reaction)
Clinical Pearl
Because diabetic patients often have sensory neuropathy, the probe-to-bone test is well tolerated even without anaesthesia - they frequently feel nothing as the probe is advanced into the wound. This also reinforces why these wounds are so dangerous - the patient's absence of pain gives no indication of how deep the infection has actually tracked.
wagner classification with images in a single slide like image
A single comprehensive medical reference slide titled "WAGNER CLASSIFICATION OF DIABETIC FOOT ULCERS" on a dark navy blue background. White text throughout. Clean clinical infographic style suitable for a medical presentation. Layout: title at top, then 6 boxes arranged in 2 rows of 3, each box representing one Wagner grade. Each box has: a large grade number badge, grade name, description, key features, and management note at bottom. GRADE 0 box (green border): - Badge: "0" in green circle - Title: "PRE-ULCER / AT-RISK FOOT" - Description: "No open ulcer — intact skin" - Features: Callus, bony prominence, deformity, neuropathy, dry fissured skin - Image placeholder: foot with callus/pressure marks - Management: "Education, offloading, accommodative footwear, regular inspection" GRADE I box (yellow/amber border): - Badge: "I" in amber circle - Title: "SUPERFICIAL ULCER" - Description: "Full-thickness skin ulcer, not penetrating deeper" - Features: Pink granulation base, raised callused edges, typically plantar/metatarsal head - Image area: shows superficial oval ulcer on foot - Management: "Clinic debridement, total contact cast, off-loading" GRADE II box (orange border): - Badge: "II" in orange circle - Title: "DEEP ULCER" - Description: "Penetrates to tendon, capsule, or bone surface" - Features: Exposed tendon or joint capsule visible, no abscess, no osteomyelitis yet - Image area: large open wound exposing deep structures - Management: "Surgical debridement, culture-specific antibiotics, TCC" GRADE III box (red border): - Badge: "III" in red circle - Title: "DEEP ULCER + OSTEOMYELITIS / ABSCESS" - Description: "Deep ulcer with bone infection or abscess formation" - Features: Probe-to-bone positive, ESR elevated, MRI confirms bone involvement - Image area: deep penetrating wound - Management: "Surgical debridement or partial amputation + antibiotics" GRADE IV box (dark red border): - Badge: "IV" in dark red circle - Title: "PARTIAL GANGRENE" - Description: "Gangrene limited to forefoot or toes" - Features: Black necrotic tissue, demarcation line, foul odor, ischemic/infected - Image area: gangrenous great toe with demarcation - Management: "Local or ray amputation based on extent" GRADE V box (black/charcoal border): - Badge: "V" in near-black circle - Title: "EXTENSIVE GANGRENE" - Description: "Gangrene of entire foot or major portion" - Features: Extensive tissue necrosis, sepsis, non-salvageable foot - Image area: whole foot gangrene schematic - Management: "Major amputation (below-knee or above-knee)" Bottom: Thin banner showing: "Severity increases with grade — Grades 0-II: conservative/minor surgical | Grades III-V: surgical/amputation" Caption: "Source: Wagner FW, 1979 | Campbell's Operative Orthopaedics 15th ed." Use color-coded severity progression: green → yellow → orange → red → dark red → black, matching the border and badge of each grade box. Each box should have equal size. Image placeholders should be represented as labeled gray boxes with a small schematic cross-section of skin layers showing depth of involvement.
429 Too Many Requests. {'message': '{\n "error": {\n "code": 429,\n "message": "Resource exhausted. Please try again later. Please refer to https://cloud.google.com/vertex-ai/generative-ai/docs/error-code-429 for more details.",\n "status": "RESOURCE_EXHAUSTED"\n }\n}\n', 'status': 'Too Many Requests'}
We encountered an error while processing your request. Please try again or reach out to us for help.