Define cholesteatoma , etiology ( table) , pathology (chart form) , clinical features, investigation and management ( non pharmacology, pharmacology and surgical treatment ( name of surgery ( anaesthesia used, indications, preop , operative steps, post op of cholesteatoma
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
cholesteatoma ear middle ear mastoid
Reading File
Here is the complete, structured clinical review of cholesteatoma:
CHOLESTEATOMA — Comprehensive Clinical Review
Sources: Cummings Otolaryngology Head and Neck Surgery; K.J. Lee's Essential Otolaryngology
1. DEFINITION
A cholesteatoma is an epidermal inclusion of the middle ear or mastoid — a cystic or sheet-like accumulation of keratinizing squamous epithelium within the middle ear cleft, filled with desquamated keratin debris. The term was coined by Johannes Müller (1838) because the white-yellow keratin flakes grossly resemble cholesterol crystals. Cruveilhier first described it as the "pearly tumor of the temporal bone" (1829).
It is not a true neoplasm — it is a destructive, expansile epidermal cyst capable of eroding bone through osteoclast activation.
2. ETIOLOGY — TABLE
| Category | Type | Mechanism |
|---|---|---|
| Congenital | Primary congenital cholesteatoma | Embryonic epidermal cell rests trapped behind an intact tympanic membrane; no prior otitis media, no TM perforation |
| Acquired — Primary | Pars flaccida retraction pocket | ET dysfunction → chronic negative middle ear pressure → retraction + invagination of pars flaccida → keratin accumulates |
| Acquired — Secondary | Epithelial migration via TM perforation | Squamous epithelium migrates through a pre-existing perforation (from CSOM) into the middle ear |
| Acquired — Secondary | Traumatic implantation | Squamous epithelium implanted during trauma, surgery, temporal bone fracture, or foreign body |
| Acquired — Secondary | Metaplasia theory | Chronic inflammation → metaplastic transformation of middle ear mucosa into keratinizing squamous epithelium |
| Acquired — Secondary | Basal cell proliferation | Hyperproliferative basal keratinocytes invade through basement membrane (invasion/proliferation theory) |
| EAC type | External auditory canal cholesteatoma | Ulceration of EAC skin + necrosis of posteroinferior EAC bone; distinct from middle ear cholesteatoma |
Key predisposing factors: Eustachian tube dysfunction, cleft palate, underdeveloped mastoid pneumatization, chronic OME, Down syndrome, craniofacial anomalies (Treacher Collins), low socioeconomic status.
3. PATHOLOGY — CHART FORM
3A. Structural Components
CHOLESTEATOMA
├── MATRIX (inner lining)
│ └── Hyperproliferative keratinizing squamous epithelium
│ (basal layer shows increased mitotic activity)
│
├── PERIMATRIX (surrounding connective tissue)
│ └── Fibrous stroma with:
│ • Macrophages, lymphocytes, plasma cells
│ • Osteoclast precursor cells
│ • Fibroblasts, histiocytes
│ • RANKL-expressing stromal & T-cells
│
└── CONTENTS
└── Laminated keratin debris (desquamated squames)
+ Small amounts of cholesterol crystals
+ Occasional anaerobic bacteria (if infected)
3B. Bone Erosion Mechanism — Pathophysiology Flowchart
Keratinizing squamous epithelium in confined middle ear space
↓
Keratin accumulation → expansion → infection
↓
Keratin extrudes into perimatrix subepithelium
↓
Inflammatory cascade activated
↓
RANKL ↑ on stromal cells & activated T-lymphocytes
+ M-CSF upregulation
↓
Osteoclastogenesis via RANK–RANKL–OPG axis
↓
Multinucleated osteoclasts recruited to bone surface
↓
Enzymatic bone resorption:
• Acid phosphatase
• Collagenase
• Cathepsin-like proteases (pH ~4.0 microenvironment)
↓
PROGRESSIVE BONE DESTRUCTION (intermittent)
→ Ossicular erosion (most common: long process of incus)
→ Scutum erosion (attic wall)
→ Tegmen erosion → intracranial extension
→ Labyrinthine fistula (horizontal SCC — 7–10% of cases)
→ Facial canal dehiscence
→ Petrous apex involvement
Old theory (abandoned): Pressure necrosis — disproven because measured cholesteatoma pressure (1.3–11.9 mmHg) never exceeds capillary perfusion pressure (~25 mmHg). Osteoclastic resorption is the established mechanism.
3C. Histopathology
- Stratified squamous epithelium with surface keratinization
- Subepithelial chronic inflammatory infiltrate
- Osteoclasts at bone interface with resorption lacunae (Howship's lacunae)
- Endochondral otic capsule bone is relatively resistant to erosion compared to intramembranous bone of middle ear and mastoid
4. CLINICAL FEATURES
Symptoms
| Feature | Details |
|---|---|
| Otorrhea | Chronic, recurrent, malodorous (foul-smelling — anaerobic organisms); scanty but persistent; unresponsive to standard topical treatment |
| Hearing loss | Progressive conductive hearing loss (ossicular erosion); mixed hearing loss if labyrinthine fistula develops |
| Otalgia | Mild, dull; acute pain if superinfected |
| Vertigo | Suggests labyrinthine (semicircular canal) fistula |
| Facial palsy | Suggests facial nerve canal erosion |
| Asymptomatic | Common in early congenital cholesteatoma — found incidentally |
Signs on Otoscopy / Microscopy
| Sign | Description |
|---|---|
| Attic retraction pocket | Pars flaccida retraction with keratin debris — most common otoscopic presentation |
| White pearly mass | Behind intact TM (congenital); or visible in attic |
| Keratin flakes | White/cream cheesy material in external canal |
| Scutal erosion | Erosion of the lateral attic wall — pathognomonic sign |
| Marginal/attic perforation | Posterosuperior or attic perforation with cholesteatoma sac visible |
| Granulation tissue | Around retraction pocket or perforation edges |
Complications
| Intratemporal | Intracranial |
|---|---|
| Conductive / mixed hearing loss | Meningitis |
| Labyrinthine fistula | Extradural abscess |
| Labyrinthitis / sensorineural HL | Subdural abscess |
| Facial nerve palsy | Brain abscess |
| Petrositis / Gradenigo syndrome | Lateral sinus thrombosis |
| Tympanosclerosis | Otitic hydrocephalus |
Gradenigo's triad (petrous apicitis): Deep facial/retro-orbital pain (V) + ipsilateral abducens palsy (VI) + otorrhea
5. INVESTIGATIONS
Audiological
| Test | Expected Finding |
|---|---|
| Pure Tone Audiogram (PTA) | Conductive hearing loss (25–60 dB depending on ossicular involvement); mixed if labyrinthine fistula |
| Tympanometry | Type B (flat) or Type C (negative pressure); flat trace with ossicular fixation |
| Tuning fork tests | Rinne negative (BC > AC), Weber lateralized to affected ear |
| Fistula test (Hennebert's test) | Positive = nystagmus with tragal pressure → suggests labyrinthine fistula |
| Speech audiometry | Assess communication impact |
Imaging
| Modality | Indication / Finding |
|---|---|
| HRCT Temporal Bone (1 mm slices, axial + coronal) | First-line imaging; soft tissue opacity in middle ear/epitympanum/mastoid; scutum erosion; ossicular destruction; tegmen/SCC involvement; facial canal dehiscence; degree of mastoid pneumatization |
| Non-EPI DWI-MRI (non-echo-planar diffusion-weighted) | Gold standard for detecting residual/recurrent cholesteatoma post-operatively; cholesteatoma shows restricted diffusion (high signal); meta-analysis confirms high sensitivity and specificity |
| Gadolinium-enhanced MRI | Differentiates cholesteatoma (non-enhancing) from granulation tissue (enhances) |
| Endoscopy / Otoendoscopy | Direct visualization of retraction pockets, hidden recesses |
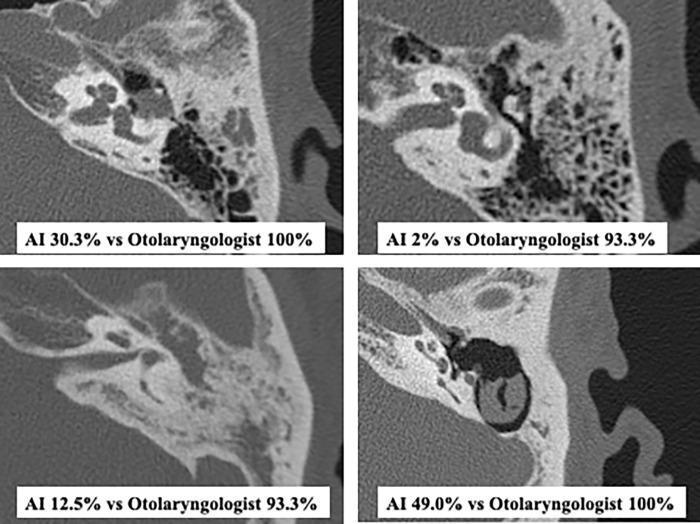
HRCT temporal bone: top row = cholesteatoma without mastoid extension; bottom row = with mastoid extension showing soft tissue opacification of mastoid air cells and ossicular destruction
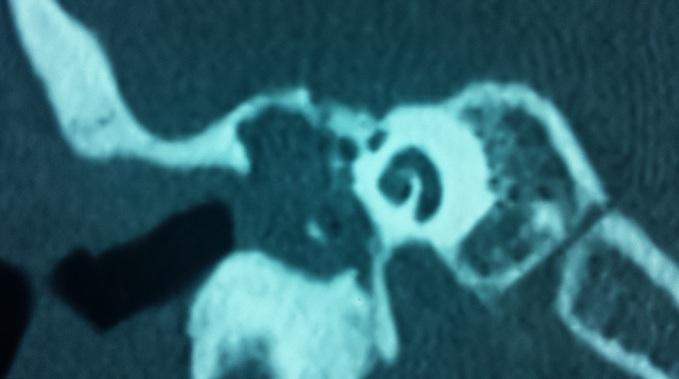
Coronal CT temporal bone: large soft tissue opacity in middle ear/epitympanum, scutum erosion, ossicular chain disruption — classic radiological signs of acquired cholesteatoma
6. MANAGEMENT
A. Non-Pharmacological (Conservative)
| Measure | Description |
|---|---|
| Microsuction / Aural toilet | Removal of keratin debris in clinic under microscope; delays surgery, prevents infection |
| Saline irrigation | Irrigation to clear accessible retraction pockets |
| Water precautions | Ear plugs, avoid swimming; prevents water-triggered infections |
| Hearing aid | If significant hearing loss and patient is not surgical candidate |
| Regular surveillance | 6–12-monthly otoscopy + audiometry; essential even between treatments |
Conservative management is temporizing only — cholesteatoma can only be cured by surgery.
B. Pharmacological
| Drug | Indication |
|---|---|
| Topical ciprofloxacin / ofloxacin drops | Treat superimposed infection; reduce otorrhea pre-operatively |
| Topical acetic acid (2%) | Anti-Pseudomonal; acidification reduces anaerobic colonisation |
| Topical steroid-antibiotic combinations | Reduce granulation tissue around retraction pocket |
| 1:3 dilute alcohol irrigation | Antiseptic; conservative topical management |
| Systemic antibiotics (amoxicillin-clavulanate, fluoroquinolones) | Active infection, pre-op preparation, post-op prophylaxis |
| IV ceftriaxone ± metronidazole | Intracranial complications (meningitis, brain abscess) |
| Antivertiginous agents | Symptomatic vertigo (labyrinthine fistula) |
C. Surgical Treatment
Surgery is the only definitive treatment. Goals:
- Complete eradication of cholesteatoma (primary)
- Management of complications
- Hearing reconstruction (secondary)
SURGERY 1: CANAL WALL-UP (CWU) TYMPANOMASTOIDECTOMY (Intact Canal Wall / Closed Technique)
| Parameter | Details |
|---|---|
| Anaesthesia | General anaesthesia, endotracheal intubation; hypotensive technique (MAP 60–70 mmHg); facial nerve monitoring (NIM) mandatory; muscle relaxant to be reversed before FN monitoring |
| Indications | Limited cholesteatoma (attic/mesotympanum); good ET function; reliable patient for follow-up; pediatric patients; desire to preserve normal EAC anatomy |
| Pre-operative | HRCT temporal bone; PTA + speech audiometry; informed consent (facial nerve injury, deafness, recurrence, second-look surgery); treat active infection with topical ± systemic antibiotics; NPO 6–8 hrs; shave hair behind pinna; anaesthetic assessment; mark operative side |
Operative Steps:
- Patient supine, head turned contralateral, arm abducted; post-aural skin incision 1 cm behind auriculocephalic sulcus
- Elevation of periosteum; identify spine of Henle (landmark for antrum) and linea temporalis
- Cortical mastoidectomy: systematic exenteration of mastoid air cells with continuous irrigation; identify mastoid antrum, horizontal (lateral) semicircular canal, fossa incudis, short process of incus, sigmoid sinus, tegmen
- Antrotomy: open antrum widely
- Atticotomy: remove lateral attic wall (scutum) bone to expose cholesteatoma in epitympanum
- Careful matrix dissection: methodical removal of cholesteatoma preserving ossicular chain if possible; trace posteriorly through antrum into mastoid
- Facial recess approach (posterior tympanotomy): thin posterior canal wall and drill facial recess (between facial nerve and chorda tympani) to expose sinus tympani, hypotympanum, round window
- Ossicular assessment: evaluate continuity; remove matrix from ossicular surfaces; preserve stapes superstructure
- Ossicular chain reconstruction (if needed): PORP (partial ossicular replacement prosthesis) or TORP (total), incus interposition, or stage for later reconstruction
- Tympanoplasty: temporalis fascia underlay graft to reconstruct TM; gelfoam packing in middle ear
- Canal packing: ribbon gauze or BIPP packing; skin closure with absorbable sutures; head bandage
Post-operative:
- Oral antibiotics (5–7 days); analgesia; antiemetics
- Canal packing removed at 2–3 weeks in clinic
- Audiogram at 6–8 weeks
- Second-look surgery at 12 months to detect residual disease (or DWI-MRI as non-invasive alternative)
- Regular follow-up every 6 months
SURGERY 2: CANAL WALL-DOWN (CWD) — MODIFIED RADICAL MASTOIDECTOMY (MRM) / RADICAL MASTOIDECTOMY (Open Cavity / Exteriorization)
| Parameter | Details |
|---|---|
| Anaesthesia | General anaesthesia, endotracheal intubation; hypotensive technique; facial nerve monitoring mandatory |
| Indications | Extensive cholesteatoma involving mastoid; revision surgery; poor ET function; labyrinthine fistula; only-hearing ear (relative); unreliable patient (cannot return for follow-up); sclerotic/poorly pneumatized mastoid; petrous apex involvement; intracranial complications |
Difference — Radical vs. Modified Radical:
- Radical mastoidectomy: posterior canal wall removed + middle ear mucosa stripped + TM removed; middle ear obliterated; Eustachian tube plugged; no hearing reconstruction — reserved for extreme disease
- MRM (standard): posterior canal wall taken down, middle ear mucosa preserved where possible, TM remnant preserved, hearing reconstruction attempted
Pre-operative:
- HRCT temporal bone (essential for surgical planning)
- PTA + tympanometry; speech audiometry
- Informed consent: mastoid cavity requiring lifelong cleaning, water precautions, possible permanent hearing loss, facial nerve risk, cavity problems (chronic discharge, recurrent infection)
- Treat active infection preoperatively
- NPO 6–8 hrs; anaesthetic assessment; mark operative side; hair shaving; IV antibiotics at induction
Operative Steps (MRM):
- Post-aural incision; periosteal elevation; identify landmarks (spine of Henle, linea temporalis, Macewen's triangle)
- Cortical mastoidectomy: complete air cell exenteration including tip cells, Trautmann's triangle (retrolabyrinthine cells); identify facial nerve, lateral SCC, sigmoid sinus, tegmen
- Lowering of the facial ridge: the posterior bony canal wall is drilled down flush with the level of the facial nerve — the key distinguishing step of canal-wall-down surgery; this externalizes the middle ear and mastoid into a single cavity
- Meatoplasty: conchal cartilage and/or skin removed to enlarge the external meatus adequately for cavity drainage, inspection, and cleaning; pinna sutured forward if necessary
- Removal of all cholesteatoma matrix from middle ear, epitympanum, mastoid
- Saucerization: all bony overhangs and ledges smoothed to create a self-cleansing, bowl-shaped cavity without recesses where keratin can re-accumulate
- Tympanoplasty (in MRM): temporalis fascia or perichondrium to reconstruct TM remnant; middle ear reconstructed if ET function adequate
- In radical mastoidectomy: middle ear obliterated; ET orifice plugged with muscle/fascia
- Cavity lined with a split-thickness skin graft or allowed to epithelialize spontaneously
- BIPP or ribbon gauze packing; wound closure; mastoid dressing
Post-operative:
- IV/oral antibiotics; analgesia
- Pack removal and first cavity inspection at 2–3 weeks
- Cavity cleaning under microscope at 6 weeks, then every 3 months for life
- Water precautions — ear plug always when bathing/swimming
- Audiogram at 6–8 weeks; hearing aid if required
- No second-look surgery needed — cavity is directly visible on clinic examination
- Watch for cavity problems: persistent discharge, polyps, recurrent infection
SURGERY 3: ENDOSCOPIC EAR SURGERY (EES) — Modern Adjunct
Transcanal endoscopic approach used for:
- Limited attic cholesteatoma (primary acquired, early congenital)
- Superior visualization of sinus tympani, hypotympanum, anterior epitympanum
- Avoids post-aural incision; can be combined with mastoidectomy (combined approach)
Surgical Decision Summary Table
| Factor | Canal Wall-Up (CWU) | Canal Wall-Down (CWD) |
|---|---|---|
| Residual disease | 11–27% | 2–10% |
| Recurrence rate | 5–13% | Rare |
| Second-look needed | Yes (or DWI-MRI) | Not required |
| Cavity problems | None | Common (lifelong cleaning) |
| Hearing outcome | Better preserved | Slightly worse |
| Normal anatomy | Preserved | Altered |
| Best for | Limited disease, reliable patient | Extensive/revision, complications, unreliable follow-up |
Quick Clinical Summary
| Point | Key Fact |
|---|---|
| Definition | Destructive keratinizing squamous epithelial cyst — NOT a tumor |
| Bone erosion mechanism | RANKL-mediated osteoclastogenesis (not pressure necrosis) |
| Most common symptom | Foul-smelling, scanty, persistent otorrhea |
| Most common ossicular erosion | Long process of incus |
| Pathognomonic otoscopic sign | Attic retraction with scutal erosion |
| Most common complication | Labyrinthine fistula (horizontal SCC, 7–10%) |
| Best post-op imaging | Non-EPI DWI-MRI for residual/recurrent disease |
| Definitive treatment | Surgery only — no pharmacological cure |
| GA type used | General anaesthesia with facial nerve monitoring |
— Cummings Otolaryngology Head and Neck Surgery, pp. 2688–2695; K.J. Lee's Essential Otolaryngology, pp. 441–452
This is a shared conversation. Sign in to Orris to start your own chat.