Diaphragm 1dt year anatomy answer
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Excellent - I now have comprehensive textbook content and diagrams. Here is the complete 1st year anatomy answer on the Diaphragm:
The Diaphragm - 1st Year Anatomy
Definition
The diaphragm is a dome-shaped musculotendinous partition that separates the thoracic cavity (above) from the abdominal cavity (below). It is the primary muscle of respiration.
Structure
The diaphragm consists of:
- A peripheral muscular part (the active contractile component)
- A central fibrous/tendinous part - the central tendon (clover-leaf shaped), into which all muscle fibers converge radially
The muscular part is divided into three portions based on origin:
| Part | Origin |
|---|---|
| Sternal part | Two small slips from the posterior surface of the xiphoid process |
| Costal part | Inner surfaces of the lower 6 ribs and their costal cartilages (ribs 7-12), interdigitating with transversus abdominis |
| Lumbar (vertebral) part | Via two crura (right and left) from lumbar vertebrae, plus medial and lateral arcuate ligaments |
The Crura
- Right crus - longer and broader; attached to bodies of L1, L2, L3 and intervening discs. The esophageal hiatus passes through the right crus.
- Left crus - attached to bodies of L1, L2 and their disc.
The two crura are connected across the midline by the median arcuate ligament, which arches over the aorta.
Arcuate Ligaments
- Median arcuate ligament - connects the two crura over the aorta (at T12)
- Medial arcuate ligament (psoas arcade) - thickening of fascia over psoas major; from body of L1 to transverse process of L1
- Lateral arcuate ligament (lumbocostal arcade) - thickening of fascia over quadratus lumborum; from transverse process of L1 to rib 12
Insertion
All peripheral muscle fibers converge into the central tendon - a strong fibrous aponeurosis in the center of the diaphragm. The fibrous pericardium is fused to its upper surface.
Domes
The diaphragm balloons upward on both sides to form two domes:
- Right dome - higher (reaches rib V / 5th intercostal space level) - pushed up by the liver
- Left dome - lower (5th intercostal space level in expiration) - pushed up by stomach/spleen
The right dome is higher than the left because of the underlying liver.
Openings (Apertures) - "I 8 10 12" Rule
The three major openings and their contents are among the highest-yield exam facts:
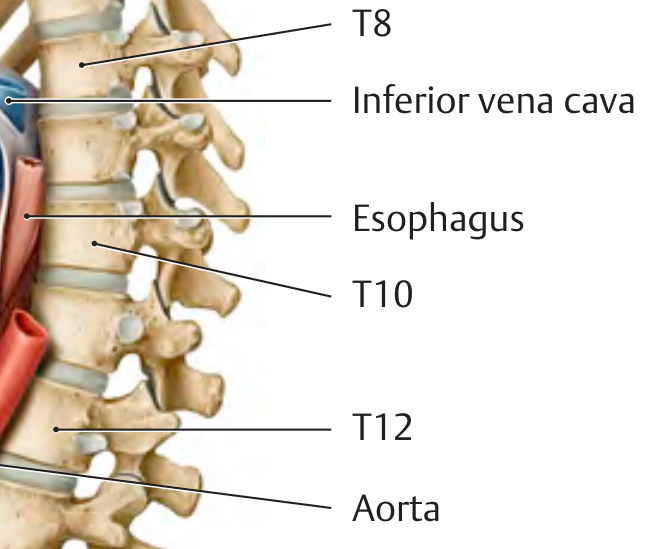
| Opening | Level | Structures Passing Through |
|---|---|---|
| Caval opening (Vena caval foramen) | T8 | Inferior vena cava (IVC) + right phrenic nerve |
| Esophageal hiatus | T10 | Esophagus + anterior and posterior vagal trunks + esophageal branches of left gastric artery/vein + lymphatics |
| Aortic hiatus | T12 | Aorta + thoracic duct + (sometimes) azygos vein |
Memory aid: I (IVC) 8 (T8), Eat (Esophagus) 10 (T10), Aorta (12) Twelve
Important notes:
- The aorta does NOT pass through the diaphragm - it passes posterior to it (between the two crura), so aortic pulsations do not affect its flow
- The left phrenic nerve passes through the muscular part of the left dome separately (not through the caval opening)
- Splanchnic nerves (greater, lesser, least) pass through the crura
- Sympathetic trunks pass posterior to the medial arcuate ligaments
- Hemi-azygos vein passes through the left crus
Superior and Inferior Diaphragm Views
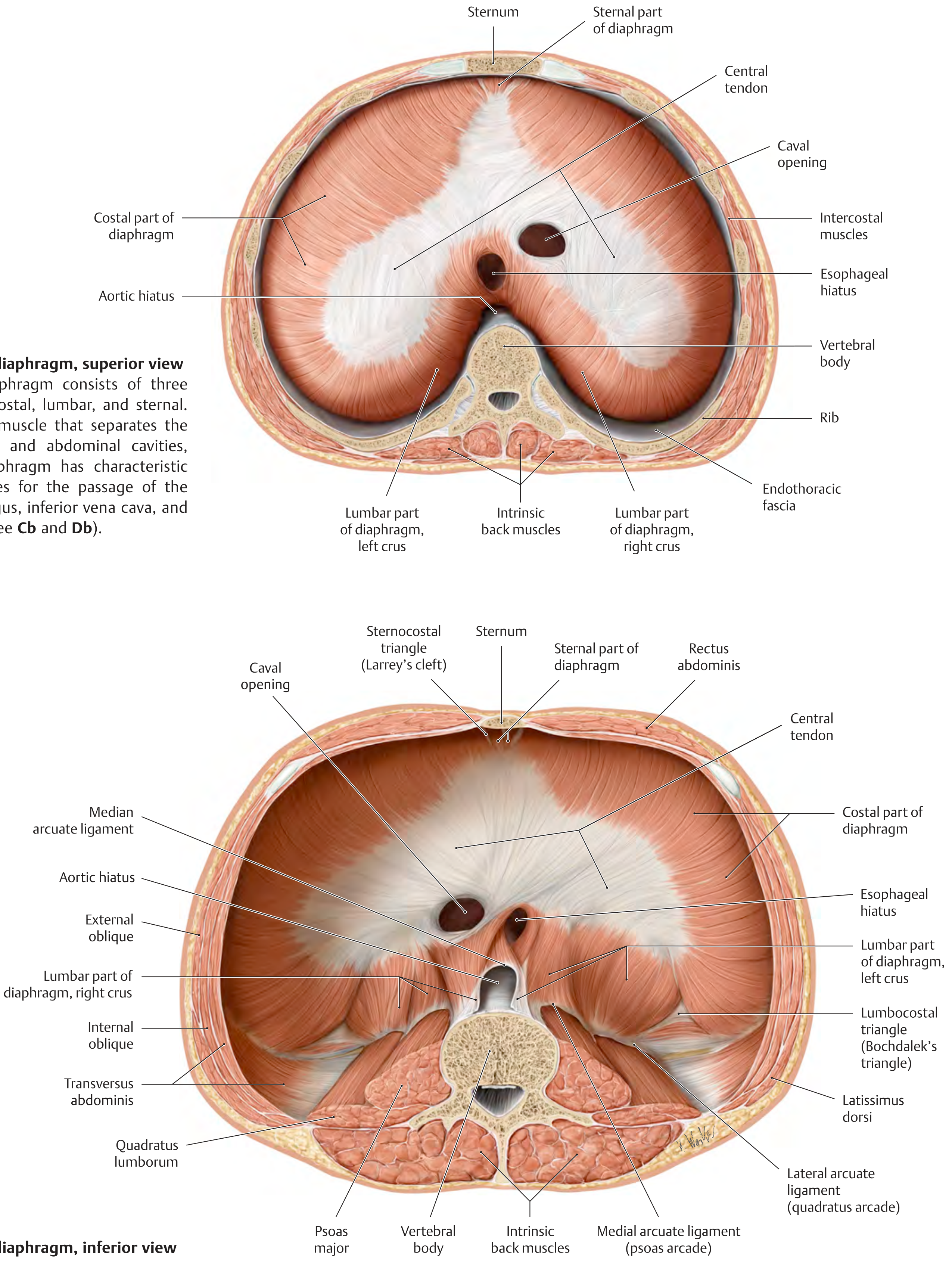
Note the Sternocostal triangle (Larrey's cleft / foramen of Morgagni) - a small gap between sternal and costal parts of the diaphragm on each side, transmitting the superior epigastric vessels. This is a site of potential anterior diaphragmatic hernia (Morgagni hernia).
Note also the Lumbocostal triangle (Bochdalek's triangle) - a gap between the costal and lumbar parts posterolaterally. This is the most common site of congenital diaphragmatic hernia (CDH), occurring in ~1 in 2200 neonates, more often on the left side.
Nerve Supply
Motor: Entirely by the phrenic nerves (C3, C4, C5 - "C3, 4, 5 keeps the diaphragm alive")
- Major contribution from C4
- Each phrenic nerve supplies the ipsilateral half of the diaphragm
Sensory:
- Central diaphragm (central tendon): phrenic nerve (C3-C5) - referred pain goes to shoulder tip (C4 dermatome)
- Peripheral diaphragm (costal part): lower intercostal nerves (T6-T12)
Embryological basis: The diaphragm develops from the septum transversum, which lies opposite C3-C5 somites in week 4. Myoblasts migrate in bringing phrenic nerve fibers with them. As the embryo grows, the diaphragm descends to its final position, stretching the phrenic nerves (hence ~30 cm long in adults).
Blood Supply
Superior surface:
- Musculophrenic artery (branch of internal thoracic artery)
- Pericardiacophrenic artery (branch of internal thoracic artery)
- Superior phrenic artery (branch of thoracic aorta)
Inferior surface:
- Inferior phrenic arteries - first branches of the abdominal aorta (or from celiac trunk)
Venous drainage parallels the arterial supply via companion veins.
Action / Function
- Primary muscle of inspiration - on contraction, the domes flatten/descend, increasing thoracic volume and decreasing intrathoracic pressure, drawing air into the lungs
- Venous return - descent of diaphragm enhances venous return to the heart by lowering thoracic pressure
- Assists in expulsive acts - coughing, sneezing, vomiting, micturition, defecation, parturition (by increasing intra-abdominal pressure)
Relations
- Superior: Heart (pericardium fused to central tendon), lungs (pleura), liver
- Inferior (abdominal surface): Liver (right), stomach + spleen (left), kidneys and suprarenal glands (posterior)
Weak Areas (Clinically Important)
| Weak Area | Location | Clinical Relevance |
|---|---|---|
| Sternocostal triangle (Larrey's cleft) | Between sternal & costal parts anteriorly | Morgagni hernia (anterior) |
| Lumbocostal triangle (Bochdalek's) | Between costal & lumbar parts posterolaterally | Most common CDH (posterior) |
| Esophageal hiatus | In right crus at T10 | Hiatal hernia (90% of diaphragmatic hernias; sliding type 85%) |
Development (Embryology)
The diaphragm develops from four sources:
- Septum transversum - main contribution; forms central tendon
- Pleuroperitoneal membranes - close the pleuroperitoneal canals
- Dorsal mesentery of the esophagus - forms the crura
- Body wall mesoderm - forms the peripheral muscular part (costal part)
Failure of closure of the pleuroperitoneal canal (especially on the left, as the right closes earlier) causes congenital diaphragmatic hernia (Bochdalek). Abdominal organs herniate into thorax, compressing the developing lungs and causing pulmonary hypoplasia - a life-threatening condition at birth.
High-Yield Summary for Exams
| Feature | Key Point |
|---|---|
| Type | Musculotendinous sheet |
| Nerve supply (motor) | Phrenic nerve C3, C4, C5 |
| Nerve supply (sensory, central) | Phrenic (C3-C5) - referred pain to shoulder |
| Nerve supply (sensory, peripheral) | Intercostal nerves T6-T12 |
| IVC opening | T8, in central tendon, right phrenic nerve passes through |
| Esophageal hiatus | T10, in right crus, vagal trunks pass with it |
| Aortic hiatus | T12, posterior to diaphragm, thoracic duct also passes |
| Right dome level | Rib V (higher, due to liver) |
| Left dome level | 5th intercostal space |
| Blood supply (inferior) | Inferior phrenic arteries from aorta |
| Most common congenital hernia site | Bochdalek (posterolateral, usually left) |
| Most common acquired hernia site | Esophageal hiatus (sliding hiatal hernia) |
Sources: Gray's Anatomy for Students (Gray's), General Anatomy and Musculoskeletal System (Thieme Atlas), The Developing Human - Clinically Oriented Embryology (Moore)
This is a shared conversation. Sign in to Orris to start your own chat.