Prolonged QT interval in ecg of chest heaviness
Reading File
Finding Sources
Finding Sources
Searching PubMed
"prolonged QT interval" AND "chest pain" AND ischemia
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Loading Image
Finding Sources
Now I have comprehensive information to give a thorough, well-structured answer.
Prolonged QT Interval on ECG with Chest Heaviness
This is a clinically urgent combination. Chest heaviness together with a prolonged QT raises the possibility of acute myocardial ischemia as both the cause of the QT prolongation and as an independent emergency. The risk is life-threatening arrhythmia - particularly torsades de pointes (TdP) and ventricular fibrillation.
Understanding the QT Interval
The QT interval represents the total period of ventricular electrical activity - from depolarization (start of QRS) to the end of repolarization (end of T wave). The heart rate strongly influences it, so the corrected QT (QTc) using Bazett's formula must always be calculated:
QTc = QT / √(R-R interval)
Normal QTc values (Tintinalli's Emergency Medicine):
- Adult males: ≤ 440 ms
- Adult females: ≤ 460 ms
- Risk threshold: QTc > 480-499 ms = moderate risk; QTc > 500 ms = significantly elevated risk of torsades
ECG example of a prolonged QT interval (QTc = 550 ms):

Why Does Chest Heaviness + Prolonged QT Matter?
Myocardial ischemia is a recognized acquired cause of QT prolongation. From multiple authoritative sources (Ganong's Physiology, Tintinalli's, Braunwald's):
"Long QT syndrome can be caused by a number of different drugs, by electrolyte abnormalities, and by myocardial ischemia." - Ganong's Review of Medical Physiology
"Acquired long QT syndrome can occur from electrolyte abnormalities, medication effects, and other disease states, such as acute coronary syndrome and severe left ventricular dysfunction." - Tintinalli's Emergency Medicine
A patient presenting with chest heaviness must therefore be evaluated for ACS first. QT prolongation in this context may be a secondary ECG marker of ongoing ischemia.
Causes of Prolonged QT (Differential Diagnosis)
| Category | Examples |
|---|---|
| Ischemia / Cardiac | Acute coronary syndrome, myocarditis, severe LV dysfunction |
| Electrolyte disorders | Hypokalemia, hypomagnesemia, hypocalcemia |
| Drugs | Procainamide, quinidine, erythromycin, azole antifungals, tricyclic antidepressants, phenothiazines, class IA/IC antiarrhythmics, organophosphates |
| Congenital syndromes | Romano-Ward syndrome, Jervell-Lange-Nielsen syndrome (+ congenital deafness) |
| Other | Hypothyroidism, anorexia nervosa, psychotropic medications |
- Rosen's Emergency Medicine, p. 1991-1996
- Tintinalli's Emergency Medicine, p. 2271
The Main Arrhythmic Danger: Torsades de Pointes
Torsades de pointes (TdP) is a polymorphic ventricular tachycardia that occurs in the setting of prolonged QT. Its defining features (Rosen's EM):
- Ventricular rate > 200 bpm
- Undulating ("twisting") QRS axis - polarity of complexes shifts around the baseline
- Paroxysms typically < 90 seconds (but can degenerate into VF)
Women are at greater risk. Acquired TdP is much more common than congenital and is pause-dependent (triggered by slow heart rate). Common triggers: hypokalemia, hypomagnesemia, and QT-prolonging drugs - especially in combination.
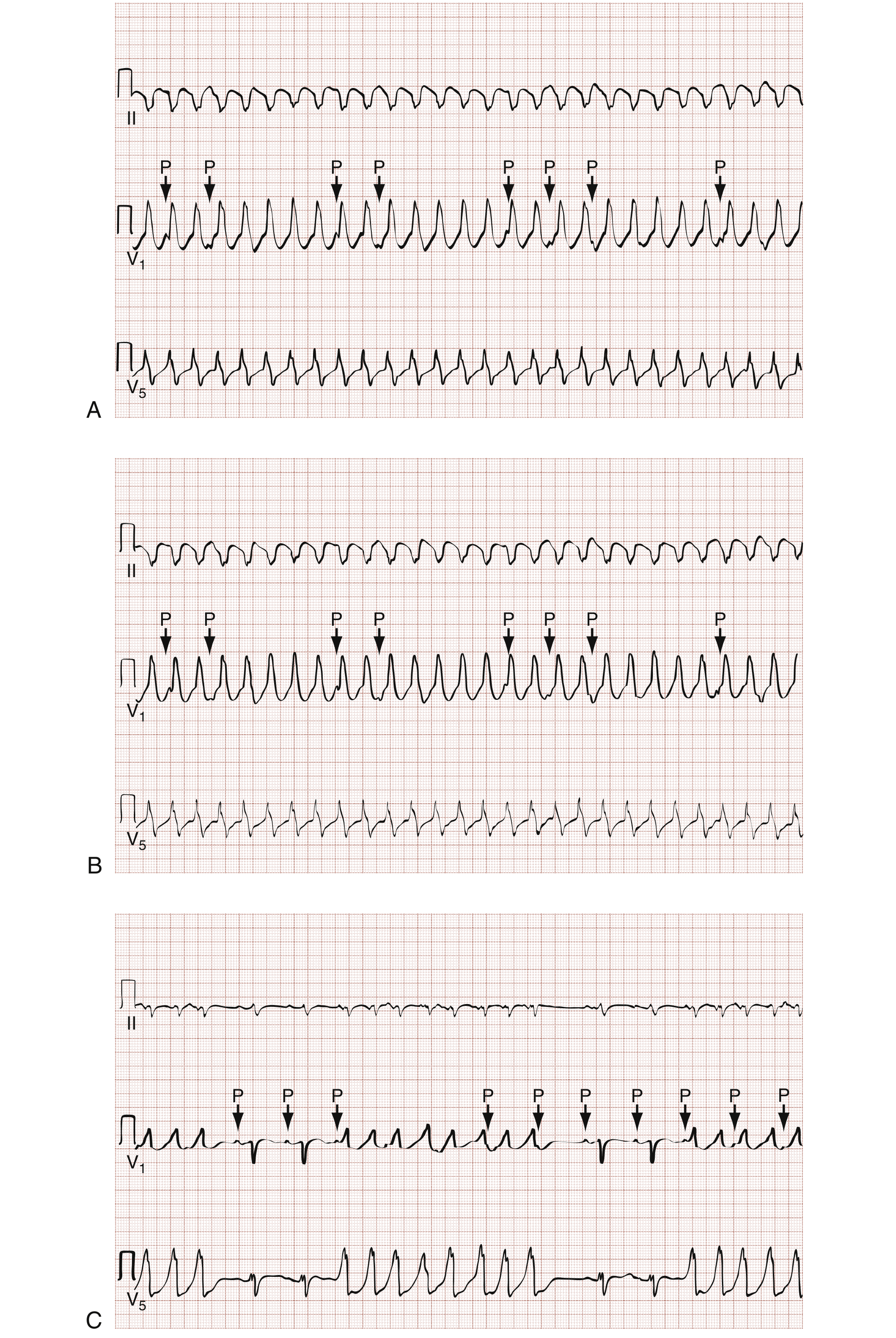
ECG of ventricular tachycardia (including intermittent/nonsustained forms):
Clinical Features to Elicit
In a patient with chest heaviness + long QT, ask about:
- Palpitations, syncope, dizziness, near-faints - suggestive of VT episodes
- Exertional symptoms - congenital LQTS; ischemia
- Family history of sudden unexplained death, cardiac disease, or congenital deafness
- Drug history - any new medications (especially antibiotics, antipsychotics, antiarrhythmics)
- Recent diarrhea/vomiting - electrolyte depletion
Schwartz Scoring for Congenital LQTS (if ACS excluded)
| Feature | Points |
|---|---|
| QTc ≥ 480 ms | 3 |
| QTc 460-479 ms | 2 |
| QTc 450-459 ms (male) | 1 |
| T-wave alternans | 1 |
| Notched T waves in ≥ 3 leads | 1 |
| Syncope (stress-provoked) | 2 |
| Syncope (not stress-provoked) | 1 |
| Family history of LQTS | 1 |
| Family history of sudden death < 30 y | 0.5 |
Score ≥ 3.5 = high probability of congenital LQTS.
Immediate Management
Priority 1: Rule Out ACS
- 12-lead ECG, serial troponins, continuous monitoring
- Look for ST changes, new Q waves, T-wave inversions alongside the long QT
- Do NOT give QT-prolonging drugs (e.g., azithromycin, ondansetron) pending workup
For Torsades de Pointes (Rosen's EM / Tintinalli's):
| Situation | Treatment |
|---|---|
| Stable, acquired TdP | IV Magnesium sulfate 1-2 g IV push (even without hypomagnesemia) |
| Electrolyte abnormalities | Correct K+, Mg2+, Ca2+ |
| Heart rate too slow | Overdrive pacing OR isoproterenol infusion (raise rate to 100-120 bpm) to shorten repolarization |
| Unstable / sustained TdP | Electrical cardioversion (synchronization may not be possible) |
| Congenital LQTS | Beta-blockers (reduce sympathetic triggers) |
Drugs to AVOID:
- Class IA antiarrhythmics: procainamide, quinidine, disopyramide
- Class IC agents
- Amiodarone (if TdP-related)
- Any further QT-prolonging medication
"Lidocaine is the safest medication for patients with prolonged QT interval-induced ventricular tachycardia or fibrillation." - Rosen's Emergency Medicine
Long-Term Management
- Congenital LQTS: Beta-blockers (first-line); pacemaker or ICD for refractory cases
- Acquired LQTS: Remove the offending drug/cause; correct electrolytes; avoid recurrence
- Refer to cardiology / electrophysiology
- Restrict competitive sports in all patients with diagnosed LQTS
- Patient education: avoid QT-prolonging drugs (check CredibleMeds)
Bottom line: Chest heaviness + prolonged QT is a red flag presentation. Treat it as a potential ACS first, immediately correct any electrolyte abnormalities, stop all QT-prolonging drugs, have magnesium sulfate at bedside, and monitor continuously. If TdP occurs, IV magnesium and overdrive pacing are the primary interventions.
- Rosen's Emergency Medicine, pp. 1996-2000; 2402-2426
- Tintinalli's Emergency Medicine, pp. 2271-2282
- Ganong's Review of Medical Physiology, p. 533
- Roberts & Hedges' Clinical Procedures in Emergency Medicine, pp. 4400-4406
This is a shared conversation. Sign in to Orris to start your own chat.