I now have all the content needed from Schwartz's Chapter 26. Let me write the comprehensive case-integrated answer.
Schwartz's Chapter 26 - Stomach: Explained & Applied to the Case
Authors: Robert E. Roses and Daniel T. Dempsey
Chapter Overview
Chapter 26 of Schwartz's Principles of Surgery covers the stomach comprehensively - from anatomy and physiology to the full spectrum of gastric diseases. The key topics are: anatomy, acid physiology, gastric mucosal barrier, peptic ulcer disease (PUD), its complications (bleeding, perforation, obstruction), surgical treatment, and gastric neoplasms. This case centers on PUD complicated by perforation, so the most relevant sections are those on NSAID-mediated injury, pathophysiology of ulceration, and perforated peptic ulcer.
PART 1: Key Chapter Concepts
Anatomy
The stomach is divided into the cardia, fundus, body (corpus), antrum, and pylorus. The lesser curvature is supplied by the left and right gastric arteries; the greater curvature by the left and right gastroepiploic arteries. The short gastric arteries supply the fundus. Venous drainage parallels the arterial supply and ultimately drains into the portal system.
Gastric Acid Physiology
Acid is secreted by parietal cells (oxyntic cells) located in the body and fundus. Stimulation occurs via three pathways:
- Neural: Vagal stimulation via acetylcholine
- Hormonal: Gastrin from antral G-cells
- Paracrine: Histamine from ECL cells (the dominant pathway for gastrin)
Basal Acid Output (BAO) is normally 2-3 mEq/hr; Maximal Acid Output (MAO) following stimulation is ~20-30 mEq/hr.
Gastric Mucosal Barrier - "Why We Don't Digest Ourselves"
This is the most critical concept for understanding this case.
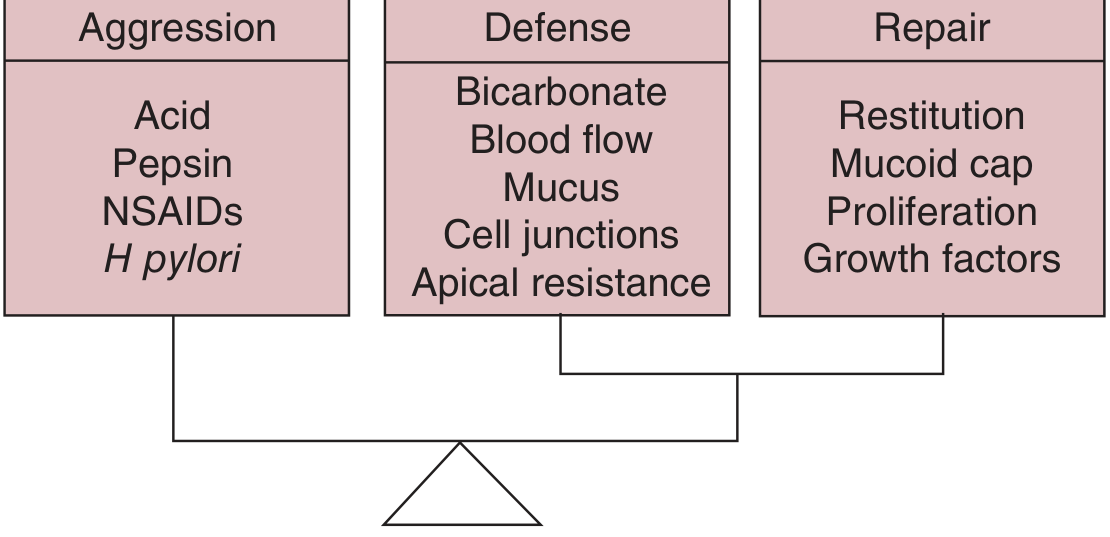
As shown above, peptic ulcer ultimately results from an imbalance between aggressive and defensive forces:
| Aggressive | Defensive | Repair |
|---|
| Acid | Bicarbonate secretion | Restitution |
| Pepsin | Blood flow | Mucoid cap |
| NSAIDs | Mucus layer | Proliferation |
| H. pylori | Cell junctions / Apical resistance | Growth factors |
The mucosal defense components include:
- Mucous barrier (traps bicarbonate close to epithelium)
- Bicarbonate secretion (maintains a near-neutral pH at the cell surface)
- Epithelial barrier with tight junctions
- Hydrophobic phospholipids
- Rapid restitution of injured cells
- Microcirculation (reactive hyperemia)
- Prostaglandins - THE KEY MEDIATOR affected by NSAIDs
(Schwartz's Principles of Surgery, 11th ed., p. 1109)
NSAIDs and Peptic Ulcer Disease - The Core Mechanism
"Chronic use of NSAIDs (including aspirin) increases the risk of peptic ulcer disease about fivefold and upper GI bleeding at least twofold." - Schwartz's, p. 1121
NSAIDs cause GI injury through two mechanisms:
- Topical/direct injury - Weak acids that become ion-trapped in gastric epithelial cells, causing direct cellular damage
- Systemic COX-1 inhibition - NSAIDs inhibit cyclooxygenase-1 (COX-1), the constitutive isoform responsible for producing prostaglandins (PGE2, PGI2) in the gastric mucosa. These prostaglandins:
- Stimulate mucus and bicarbonate secretion
- Maintain mucosal blood flow
- Inhibit acid secretion
- Promote epithelial restitution
When COX-1 is blocked by NSAIDs → prostaglandin production falls → mucus and bicarbonate secretion decrease → mucosal blood flow decreases → the barrier fails → acid penetrates → ulceration.
Risk factors for NSAID-induced GI complications (from Schwartz's, p. 1121):
- Age >60
- Prior GI event
- High NSAID dose (directly relevant here)
- Concurrent steroid intake
- Concurrent anticoagulant intake
The risk in elderly patients on NSAIDs is 10 times that of controls for requiring an operation from a GI complication, and 4.5 times higher for death from a GI cause. (Schwartz's, p. 1121)
Peptic Ulcer Disease - Pathophysiology
PUD involves focal defects in gastric or duodenal mucosa that extend into the submucosa or deeper. The two dominant causes are:
- H. pylori infection
- NSAID/aspirin use
Type V gastric ulcers (by the modified Johnson classification) are medication-induced and can occur anywhere in the stomach.
Complications of PUD (in decreasing frequency):
- Bleeding (most common, most deaths)
- Perforation (second most common; now more common indication for surgery)
- Obstruction
"As with bleeding ulcer, NSAID and/or aspirin use have been inextricably linked with perforated PUD, especially in the elderly population." (Schwartz's, p. 1134)
Perforated Peptic Ulcer - Schwartz's Full Coverage
Perforation occurs when an ulcer erodes through the entire wall of the stomach or duodenum, releasing gastric contents into the peritoneal cavity. This causes chemical peritonitis initially (sterile, from acid and enzymes), which within hours becomes bacterial peritonitis.
Clinical features:
- Sudden onset of severe, steady, knife-like epigastric pain (this is the classic description)
- Rapid progression to diffuse abdominal pain
- Board-like rigidity of the abdomen (guarding/rigidity)
- Referred pain to the shoulder (diaphragmatic irritation)
- Signs of peritonitis: tenderness, rebound, guarding
- As time passes: pallor, diaphoresis, tachycardia, hypotension (shock)
- Free air under the diaphragm on imaging
Surgery is almost always indicated. Nonsurgical management is reserved for the stable patient without peritonitis in whom a sealed perforation is radiologically confirmed.
PART 2: Case Application
Clinical Recap
65-year-old male with chronic gouty arthritis, on Ibuprofen (an NSAID) self-medicating with double or triple doses almost daily for recurrent flares. Presents with sudden-onset epigastric stabbing and steady pain that worsened over 2 hours, with pallor and diaphoresis, screaming in pain.
Question 1: Additional History to Extract
As clinical clerk, you need to gather:
Pain History (OLDCARTS):
- Onset: Was it truly sudden ("like a knife") or gradual?
- Prior episodes of epigastric pain, heartburn, or dyspepsia?
- Any hematemesis (vomiting blood) or melena (black tarry stools)?
- Does anything relieve the pain (food, antacids)?
NSAID Intake Details:
- Exact dose and frequency (how many tabs per episode)
- Duration of regular daily use
- Any concomitant alcohol use
- Any prior GI events (bleeding, hospitalization)
Medical/Surgical History:
- Any prior GI endoscopy? Prior PUD diagnosis?
- Any other medications (steroids, anticoagulants, aspirin)?
- Smoking history (independent risk factor for PUD)
- Comorbidities: hypertension, diabetes, cardiovascular disease
Family History: GI cancers, peptic ulcer disease
Review of Systems:
- Weight loss, anorexia (rule out malignancy)
- Urinary symptoms
- Fever/chills
- Any referred shoulder pain (diaphragm irritation from free air)
Question 2: Necessary Assessment
Vital Signs (PRIORITY):
- Blood pressure, heart rate, respiratory rate, temperature, O2 saturation
- The pallor and diaphoresis suggest hemodynamic instability - assess for shock (hypotension + tachycardia)
Physical Examination:
| Area | Expected Finding |
|---|
| General | Ill-appearing, diaphoretic, pale, in acute distress |
| Abdomen | Board-like rigidity (involuntary guarding), diffuse tenderness with rebound, absent bowel sounds (ileus from peritonitis) |
| Epigastrium | Maximum tenderness |
| Liver dullness | May be absent on percussion (Traube's space) - indicates free air |
| Rectal exam | Check for melena (blood in stool = concurrent bleed) |
| Cardiovascular | Tachycardia, possibly hypotension |
Question 3: Initial Impression
PERFORATED PEPTIC ULCER - most likely a perforated duodenal or prepyloric gastric ulcer (Type III Johnson) given:
- Sudden onset of severe, stabbing, steady epigastric pain - the classic presentation of perforation
- Rapid deterioration over 2 hours with signs of peritonitis (pallor, diaphoresis, screaming pain)
- Strong predisposing etiology (chronic high-dose NSAID use)
Differential diagnoses to consider:
- Acute pancreatitis (epigastric pain, but usually radiates to back, more gradual)
- Acute myocardial infarction (can present as epigastric pain in elderly)
- Mesenteric ischemia (more diffuse, pain out of proportion to exam)
- Bleeding peptic ulcer without perforation
- Aortic aneurysm rupture
Question 4: Risk Factor Correlation
| Risk Factor | Relevance from Chapter 26 |
|---|
| Age 65 | Age >60 increases NSAID GI complication risk 5x vs controls; risk of needing operation is 10x higher (Schwartz's p. 1121) |
| Chronic NSAID use (Ibuprofen) | NSAIDs inhibit COX-1 → decrease prostaglandin synthesis → break down mucosal defense (mucus, bicarbonate, blood flow) |
| Double/triple dosing | High NSAID dose is explicitly listed as a risk factor for GI complications (Schwartz's, p. 1121) |
| Daily use | Chronic, near-daily exposure without PPI prophylaxis - highest risk scenario |
| No PPI co-prescription | PPIs or high-dose H2RAs should always accompany NSAIDs in high-risk patients; omission here likely contributed to ulceration |
| No regular follow-up | Missed opportunity to detect and treat ulcer before perforation |
| Possible H. pylori co-infection | Older males, especially in developing-country settings, have high H. pylori prevalence; co-infection with NSAID use dramatically amplifies risk |
The mechanism is a failure of mucosal defense - Ibuprofen suppressed prostaglandin production, reducing mucus and bicarbonate secretion and compromising the mucosal blood flow. High doses overwhelmed any residual defense, leading to ulceration and ultimately full-thickness perforation.
Question 5: Diagnostic Modalities
Immediate/Bedside:
- Erect Chest X-ray - Look for free air under the diaphragm (pneumoperitoneum) - present in ~70-80% of perforations. This is the single most important initial test.
- ECG - Rule out NSTEMI/STEMI (epigastric presentation)
Laboratory:
| Test | Purpose |
|---|
| CBC | Leukocytosis (infection/peritonitis); anemia (bleeding) |
| Serum amylase/lipase | Rule out pancreatitis |
| Comprehensive metabolic panel | BUN/Cr (elevated BUN/Cr ratio suggests upper GI bleed), electrolytes |
| Serum lactate | Assess for sepsis/ischemia |
| ABG | Metabolic acidosis if shocked |
| PT/INR, aPTT | Pre-operative coagulation status |
| Type and crossmatch | Pre-operative preparation |
| Blood cultures | If sepsis suspected |
| H. pylori serology or stool antigen | To guide post-operative eradication therapy |
Imaging:
| Modality | Finding |
|---|
| Erect CXR | Free air under diaphragm (pneumoperitoneum) |
| CT Abdomen/Pelvis with IV contrast | Gold standard - identifies free air, free fluid, perforation site, extent of peritoneal contamination |
| Left lateral decubitus X-ray | Alternative if erect CXR equivocal |
| Upright abdominal X-ray | Adjunct |
Note: Upper GI endoscopy is generally contraindicated in suspected perforation as insufflation worsens pneumoperitoneum.
Risk Stratification:
- AIMS65 score for inhospital mortality and length of stay
- Blatchford score and Rockall score if bleeding is also suspected (Schwartz's, p. 1131)
Question 6: Management Plans
IMMEDIATE - Resuscitation (ABCs):
- IV access - Two large-bore IVs
- Aggressive IV fluid resuscitation - Crystalloids; correct hypotension/shock
- NPO (nothing by mouth)
- Nasogastric tube (NGT) - Decompress stomach, reduce ongoing spillage
- Urinary catheter - Monitor urine output (target >0.5 mL/kg/hr)
- High-dose IV Proton Pump Inhibitor - e.g., Pantoprazole or Omeprazole IV
- IV Antibiotics - Broad-spectrum (e.g., Piperacillin-tazobactam or Cefazolin + Metronidazole) to cover GI flora
- Analgesia - IV opioids (morphine/tramadol) for pain control
- Surgical consultation - URGENT
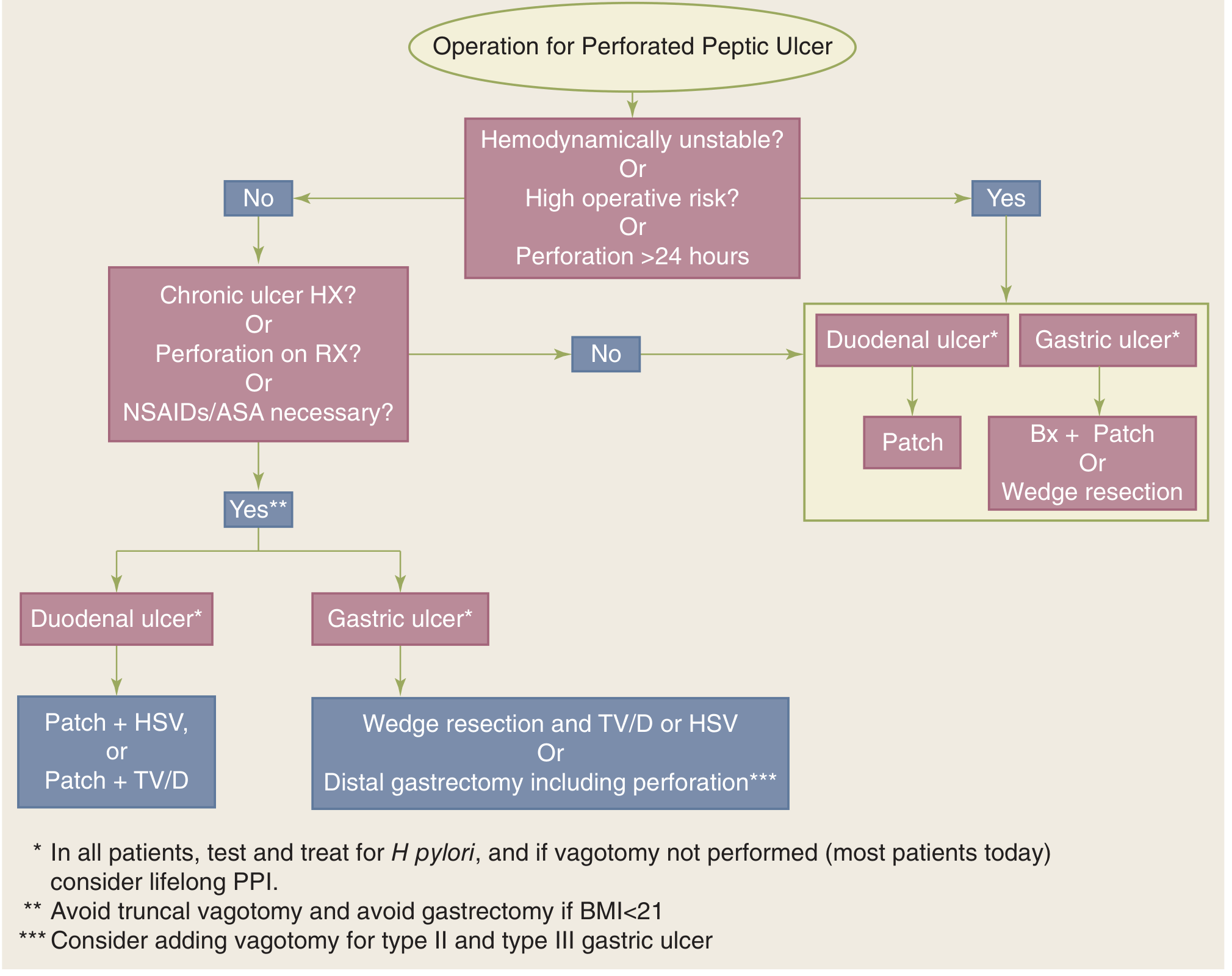
DEFINITIVE - Surgical Management:
Per Schwartz's Fig. 26-44 (shown below):
Given this patient is:
- Elderly (65 yo) with likely hemodynamic instability
- Presenting ~2 hours after onset with escalating symptoms
- High operative risk
The likely procedure is simple patch closure (Graham patch/omentopexy) of the perforation:
- Close perforation with omental patch
- Lavage the peritoneal cavity thoroughly
- Consider adding highly selective vagotomy (HSV) if patient is stable and has chronic ulcer history
For duodenal ulcer: patch + HSV or patch + truncal vagotomy and drainage
For gastric ulcer: wedge resection or distal gastrectomy if stable
Post-operative Plans:
- Continue IV PPI; transition to oral PPI long-term
- Stop all NSAIDs - Switch gout management to colchicine or allopurinol (discuss with rheumatology)
- Test and treat for H. pylori (rapid urease test on intraoperative biopsy or post-op serology; treat with triple therapy if positive)
- ICU or monitored bed post-operatively
- Monitor for complications: anastomotic leak, wound infection, sepsis
- Nutritional support
- Consider lifelong PPI if H. pylori negative (since NSAID-associated ulcer and cannot guarantee complete NSAID cessation)
- Patient education on NSAID dangers and importance of follow-up
Summary Table: Case vs. Chapter 26 Correlation
| Chapter Concept | Case Application |
|---|
| Mucosal defense (prostaglandins) | Ibuprofen → COX-1 inhibition → prostaglandin deficiency → mucosal failure |
| Type V gastric ulcer (NSAID-induced) | Most likely ulcer type in this patient |
| Risk factors for NSAID-GI complications | Age 65, high dose, chronic daily use = highest risk tier |
| PUD complications: perforation (2nd most common) | Sudden severe epigastric pain → chemical peritonitis → surgical emergency |
| Clinical signs of perforation | Stabbing steady pain, pallor, diaphoresis, rigidity |
| Diagnosis | Erect CXR (free air), CT abdomen, labs |
| Medical Rx | IV PPI, NGT, antibiotics, NPO, fluid resuscitation |
| Surgical Rx | Graham patch ± HSV; consider definitive ulcer operation if stable |
| Post-op Rx | PPI long-term, H. pylori test-and-treat, NSAID cessation |
All clinical content referenced from Schwartz's Principles of Surgery, 11th Edition, Chapter 26 - Stomach (Robert E. Roses and Daniel T. Dempsey), pp. 1099-1154.