The auscultation for the heart valves clinical anatomy
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have all the key content and the anatomical diagram. Here is the full, comprehensive answer:
Auscultation of Heart Valves: Clinical Anatomy
The Five Classic Auscultatory Areas
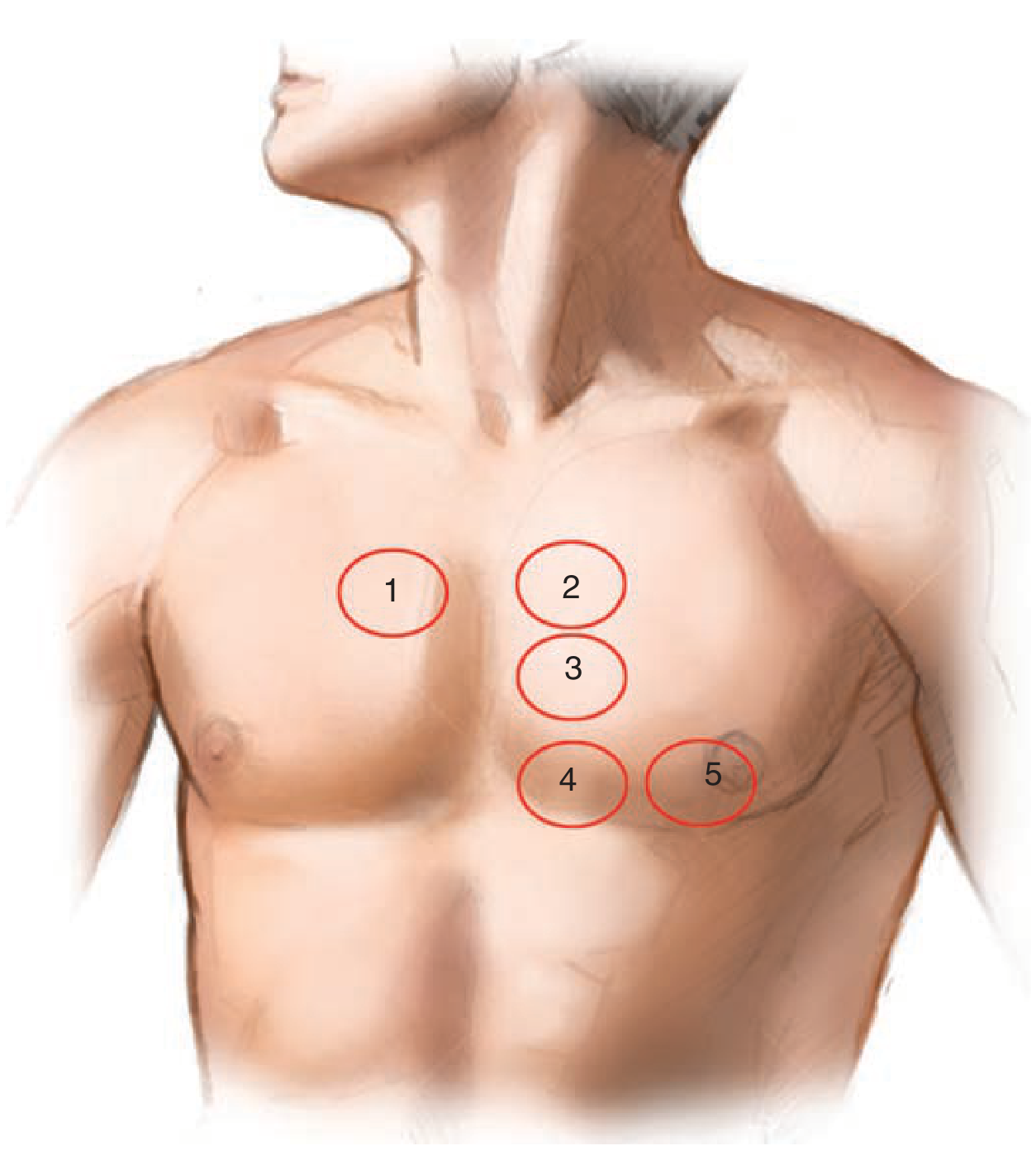
Figure 2-15: (1) Aortic, (2) Pulmonic, (3) Accessory Aortic, (4) Tricuspid, (5) Mitral - Fuster and Hurst's The Heart, 15th Ed.
Key concept: Auscultatory areas do NOT correspond to the anatomical location of the valves. They are the sites on the chest wall where sounds from each valve are best conducted and heard.
| Area | Location | Valve Sounds Best Heard |
|---|---|---|
| Aortic | 2nd ICS, right parasternal line | Aortic valve (AS murmur, A2) |
| Pulmonic | 2nd ICS, left parasternal line | Pulmonic valve (P2, PS murmur) |
| Accessory Aortic (Erb's point) | 3rd ICS, left parasternal line | Aortic regurgitation |
| Tricuspid | 5th ICS, left parasternal line | Tricuspid valve murmurs |
| Mitral (Apex) | Over the apical impulse (~5th ICS, midclavicular line) | Mitral valve (MR, MS rumble) |
ICS = intercostal space
Why Sounds Are Heard Where They Are
Sound from each valve is conducted downstream in the direction of turbulent blood flow:
- Aortic stenosis murmur: heard at the base (right 2nd ICS) and radiates to the carotid arteries
- Mitral regurgitation murmur: heard at the apex and radiates to the left axilla
- Aortic regurgitation murmur: heard along the left sternal border (3rd-4th ICS) when caused by valve disease; when caused by aortic root dilation, it may be more audible along the right sternal border
- Tricuspid regurgitation: can radiate to the right sternal border; increases with inspiration (Carvallo's sign)
Technique
Auscultation must be performed in three positions:
- Sitting up, leaning forward - best for aortic regurgitation and pericardial rubs; base of heart sounds
- Supine - standard for most heart sounds
- Left lateral decubitus - brings the apex closer to the chest wall; best for mitral murmurs (especially the low-pitched MS rumble) and S3/S4 gallops
Stethoscope use:
- Diaphragm (firm pressure): high-pitched sounds - most murmurs, S1, S2, aortic regurgitation, ejection clicks, opening snaps
- Bell (light pressure): low-pitched sounds - S3, S4, mitral stenosis diastolic rumble, vascular bruits. If excessive pressure is applied to the bell, it acts like a diaphragm and low-pitched sounds are lost
The stethoscope should NOT jump between areas - it should be marched continuously from the apex to the sternum and up the parasternal line, to avoid missing localized findings.
Heart Sounds and Their Valve Origins
S1 (First Heart Sound)
- Produced by closure of the mitral and (to a lesser extent) tricuspid valves - marks the end of diastole/start of systole
- Louder in mitral stenosis (when leaflets are mobile)
- Softer in mitral regurgitation (poor leaflet coaptation)
S2 (Second Heart Sound)
- Produced by closure of the aortic valve (A2) followed by the pulmonic valve (P2)
- Physiologic splitting: On inspiration - increased RV filling delays P2, causing audible splitting (A2 then P2). On expiration - both coincide and S2 is single
- Fixed splitting: A2-P2 interval unchanged with respiration - seen in atrial septal defect and right bundle branch block
- Paradoxical splitting: S2 splits on expiration and becomes single on inspiration - delayed A2 (e.g., severe AS, HOCM, LBBB)
- Loud A2: systemic hypertension
- Soft/absent A2: severe calcific aortic stenosis
- Loud P2: pulmonary hypertension
Opening Snap
- High-pitched sound in early diastole - heard before rapid filling begins
- Mitral opening snap: heard best at the apex
- Tricuspid opening snap: left 3rd-4th ICS
- Distinguished from a loud P2 by its longer interval from S2 and its location
S3 (Third Heart Sound)
- Low-pitched sound in early diastole - corresponds to rapid ventricular filling
- Normal in children and young adults; pathological after age ~40
- Causes: mitral regurgitation (increased filling volume), heart failure (elevated filling pressures)
- Left ventricular S3: heard at the apex with the bell
- Right ventricular S3: heard at the 4th ICS, left parasternal border with the bell
S4 (Fourth Heart Sound)
- Low-pitched sound in late diastole - from atrial contraction against a stiff ventricle
- Nearly ubiquitous in hypertension, heart failure, ischemic heart disease
Murmur Characteristics at Each Valve
Aortic Stenosis (AS)
- Harsh systolic ejection murmur, late-peaking
- Best heard at the right 2nd ICS, radiates to carotids
- Gallavardin phenomenon: high-frequency components radiate to apex and can mimic MR
- Louder and later-peaking = more severe
- Decreases with standing/Valsalva; increases with squatting
Aortic Regurgitation (AR)
- High-pitched, blowing diastolic murmur, begins immediately after A2
- Best heard at the left sternal border (3rd-4th ICS), with patient sitting up and leaning forward in deep exhalation
- Duration correlates better with severity than intensity
- Austin Flint murmur: a mid-to-late diastolic low-pitched rumble at the apex in severe AR (AR jet impinging on the mitral valve)
Mitral Stenosis (MS)
- Low-pitched diastolic rumble with pre-systolic accentuation (in sinus rhythm)
- Best heard at the apex, with patient in left lateral decubitus, using the bell
- Preceded by an opening snap
- Louder S1 when leaflets remain mobile
Mitral Regurgitation (MR)
- High-pitched, blowing pansystolic murmur
- Best heard at the apex, radiates to the left axilla
- Intensity unaffected by beat-to-beat variation (unlike AS)
Tricuspid Regurgitation (TR)
- Pansystolic murmur at the lower left sternal border (tricuspid area)
- Increases with inspiration (Carvallo's sign) - distinguishes TR from MR
Pulmonic Stenosis (PS)
- Systolic ejection murmur at the left 2nd ICS
- Often preceded by an ejection click
Murmur Grading (Levine Scale)
| Grade | Description |
|---|---|
| I | Faint; heard only after a few seconds of focused auscultation |
| II | Moderately loud; heard immediately |
| III | Loud; no thrill |
| IV | Loud; associated with a palpable thrill |
| V | Very loud; heard with stethoscope edge barely on skin |
| VI | Heard without stethoscope touching chest |
Systolic murmurs are graded I-VI; diastolic murmurs I-IV.
Prosthetic Valve Sounds
- All mechanical valves produce a crisp high-pitched closing click
- Older ball-cage and tilting-disk prostheses also produce an opening click
- Newer bileaflet valves are typically silent on opening
- Any regurgitant murmur from a prosthetic valve is pathological (paravalvular leak, leaflet dysfunction)
- Normal prostheses have an intrinsic mild ejection murmur (aortic/pulmonic position) or a soft diastolic rumble (mitral/tricuspid position)
Sources: Fuster and Hurst's The Heart, 15th Ed. | Goldman-Cecil Medicine, International Edition | Braunwald's Heart Disease, 11th Ed.
summary
Auscultation of Heart Valves - Summary
5 Auscultatory Areas
(Not the anatomical valve locations - where sounds are best heard)
| # | Area | Location | Best For |
|---|---|---|---|
| 1 | Aortic | 2nd ICS, right sternal border | AS murmur, A2 |
| 2 | Pulmonic | 2nd ICS, left sternal border | P2, PS murmur |
| 3 | Erb's Point | 3rd ICS, left sternal border | Aortic regurgitation |
| 4 | Tricuspid | 5th ICS, left sternal border | TR/TS murmurs |
| 5 | Mitral (Apex) | 5th ICS, midclavicular line | MR, MS rumble |
Heart Sounds - Origins
| Sound | Cause | Key Point |
|---|---|---|
| S1 | Mitral + tricuspid closure | Loud in MS; soft in MR |
| S2 | Aortic (A2) + pulmonic (P2) closure | Physiologic split on inspiration |
| S3 | Rapid early diastolic filling | Pathological >40 yrs (heart failure, MR) |
| S4 | Atrial contraction vs stiff ventricle | Hypertension, ischemia |
| Opening snap | Stenotic AV valve opening | MS at apex; TS at left 3rd-4th ICS |
Key Murmurs
| Valve Lesion | Timing | Character | Radiation |
|---|---|---|---|
| Aortic stenosis | Systolic ejection | Harsh, late-peaking | Carotids |
| Aortic regurgitation | Early diastolic | High-pitched, blowing | Left sternal border |
| Mitral stenosis | Mid-diastolic | Low rumble + opening snap | None |
| Mitral regurgitation | Pansystolic | Blowing | Left axilla |
| Tricuspid regurgitation | Pansystolic | Increases with inspiration | Right sternal border |
3 Patient Positions
- Supine - standard
- Left lateral decubitus - mitral murmurs, S3/S4
- Sitting, leaning forward - aortic regurgitation, pericardial rub
Stethoscope
- Diaphragm - high-pitched sounds (most murmurs, S1, S2, AR)
- Bell (light pressure) - low-pitched sounds (S3, S4, MS rumble)
Murmur Grading
- I-III: no thrill | IV-VI: thrill present | Grade VI heard without stethoscope
hemoptasis
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Excellent - I now have comprehensive content and the management algorithm. Here is the full structured answer:
Hemoptysis
Definition
Hemoptysis is the expectoration of blood originating from the lower respiratory tract (from the glottis to the alveolus). It ranges from blood-streaked sputum to massive, life-threatening hemorrhage.
Massive hemoptysis = >150-200 mL in 24 hours OR a rate ≥100 mL/h. Patients rarely die of exsanguination - they die of asphyxiation from blood filling the airways.
Hemoptysis vs. Pseudohemoptysis
| Feature | Hemoptysis | Hematemesis | Epistaxis |
|---|---|---|---|
| Color | Bright red | Dark/coffee-ground | Red, from nose |
| pH | Alkaline | Acidic | - |
| Consistency | Frothy, mixed with sputum | Contains food particles | - |
| Microscopy | Hemosiderin-laden macrophages | - | - |
| Associated symptoms | Cough, dyspnea | Nausea, GI history | Nasal symptoms |
~10% of presumed hemoptysis cases are actually pseudohemoptysis.
Anatomy of Bleeding
- Most hemoptysis arises from the bronchial circulation (high-pressure, originates from the aorta)
- The pulmonary circulation is low-pressure; massive bleeding from it is less common
- Bronchial arteries neovascularize tumors, dilated airways (bronchiectasis), and cavitary lesions - making these vulnerable to rupture
Causes (Etiology)
Infections (Most common globally)
| Cause | Mechanism |
|---|---|
| Viral/bacterial bronchitis | Most common cause of minor hemoptysis in developed countries |
| Bronchiectasis (incl. cystic fibrosis) | Dilated, inflamed, highly vascular bronchial arteries; can cause massive hemoptysis |
| Tuberculosis | Cavitary disease; Rasmussen's aneurysm (pulmonary artery erosion into TB cavity) |
| Aspergilloma (mycetoma) | Neovascularization of preexisting cavities; life-threatening |
| Lung abscess / necrotizing pneumonia | S. aureus, Klebsiella, anaerobes |
| Endemic fungi (Histoplasma, Coccidioides) | Cavitary disease |
| Paragonimiasis | Mimics TB; common in Southeast Asia |
Malignancy
- Bronchogenic carcinoma (any histology) - common cause, both massive and non-massive
- Squamous cell / small cell carcinoma - central tumors that erode into major pulmonary vessels
- Carcinoid tumors - highly vascular, arise in proximal airways
- Pulmonary metastases - melanoma, sarcoma, breast, colon
- Kaposi's sarcoma in HIV/AIDS
Age clue: Hemoptysis before age 40 - think infections. After age 40-45 or with smoking history - think bronchogenic carcinoma.
Vascular
| Cause | Notes |
|---|---|
| Pulmonary embolism | Parenchymal infarction; "pink frothy" sputum in pulmonary edema |
| Mitral stenosis | Elevated pulmonary venous pressure |
| AVM (arteriovenous malformation) | Hereditary hemorrhagic telangiectasia |
| Aortobronchial fistula | Aortic aneurysm eroding into bronchus; initially minor then massive |
| Diffuse alveolar hemorrhage (DAH) | SLE, GPA, anti-GBM disease (Goodpasture), cocaine, stem cell transplant, vaping |
Autoimmune / Pulmonary-Renal Syndromes
- Granulomatosis with polyangiitis (GPA) - formerly Wegener's
- Anti-GBM (Goodpasture) disease - hemoptysis + hematuria
- Both can cause DAH
Other / Mechanical
- Catamenial hemoptysis - pulmonary endometriosis; cyclical, with menses
- Foreign body aspiration
- Iatrogenic: pulmonary artery catheter rupture, post-lung biopsy, post-pulmonary vein isolation
- Coagulopathy / anticoagulation / antiplatelet therapy
- COPD - unexplained, usually not recurrent
Management Algorithm
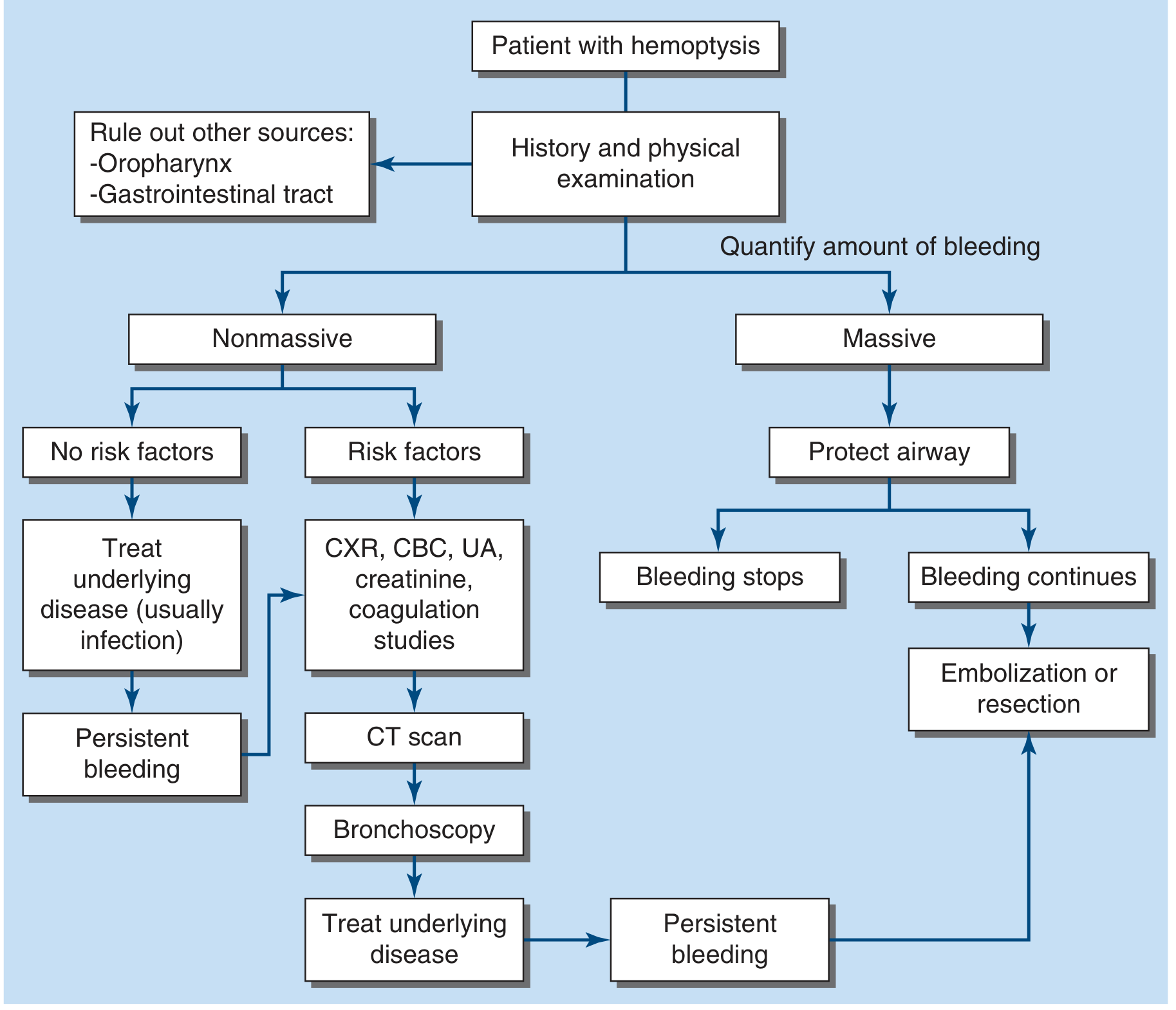
Figure 41-1: Approach to hemoptysis management - Harrison's Principles of Internal Medicine, 22nd Ed.
Evaluation
History
- Volume and frequency (quantify with references: 1 cup = 236 mL)
- Smoking history, weight loss (malignancy)
- Fever, productive cough (infection)
- Prior lung disease (bronchiectasis, CF, TB, cancer)
- Immobilization (PE), anticoagulants, autoimmune history
- Cyclical pattern with menses (catamenial)
Physical Examination
- Assess for life threat: hypoxemia, tachycardia, hemodynamic instability
- Examine nasal/oral cavities (rule out epistaxis)
- Lung auscultation: lateralizing crackles, wheeze
- Cardiac: murmurs (mitral stenosis)
- Skin: telangiectasias (HHT), purpura (vasculitis), ecchymoses (coagulopathy), clubbing
Laboratory
- CBC, coagulation studies (PT/INR, aPTT), BMP, urinalysis
- Sputum cultures, AFB smear/culture (if TB suspected)
- ANA, ANCA, anti-GBM antibodies (if vasculitis/Goodpasture suspected)
- D-dimer / BNP if PE or CHF suspected
Imaging
| Modality | Role |
|---|---|
| CXR | First-line but poor sensitivity; may show mass, infiltrate, cavity |
| CT chest (with contrast/angiography) | Identifies cause and localizes bleeding in 70-88% of cases; best for bronchiectasis, malignancy, cavitary disease |
| CT angiography | Visualizes bronchial/non-bronchial arteries; guides embolization |
| Bronchoscopy | Localizes bleeding in airways; less sensitive than CT for parenchymal causes; role in massive hemoptysis for airway management and ablative therapy |
Management
Non-Massive Hemoptysis
- No risk factors (young, non-smoker, normal CXR): treat underlying infection, close follow-up
- With risk factors (age >40, smoker, abnormal CXR): CT chest + bronchoscopy + treat underlying cause
Massive Hemoptysis - Emergency Approach
1. Protect the airway (top priority)
- Place patient in lateral decubitus, bleeding side DOWN - prevents blood spilling into the unaffected lung
- Supplemental oxygen
- Avoid aggressive sedation - cough reflex is the patient's own airway clearance mechanism
2. Intubation (if bleeding overwhelms airway)
- Single-lumen ET tube (≥8 Fr) - easier placement, allows bronchoscopy
- Double-lumen ET tube (DLT) - isolates each hemithorax independently; requires expertise
- Endobronchial blocker - balloon tamponade of bleeding segment via bronchoscope
3. Bronchial Artery Embolization (BAE)
- First-line definitive procedure for massive hemoptysis
- Controls bleeding in 75-90% of patients
- Rebleeding rate: 20-50% without definitive surgery
- Complications: post-embolization syndrome (fever, pleuritic pain, dysphagia - resolves in 5-7 days), rare: spinal cord infarction, esophageal/bronchial necrosis
4. Surgery
- Salvage strategy after failed embolization
- Better outcomes in elective (non-urgent) setting
5. Endobronchial therapies (via bronchoscope)
- Nd:YAG laser, argon plasma coagulation, electrocautery - for localized endobronchial lesions
- Cryoprobe - for clot removal
Specific Therapies
- Anticoagulation reversal if on anticoagulants
- Blood products: FFP, platelets for coagulopathy/thrombocytopenia
- Desmopressin (DDAVP) - for platelet dysfunction in renal failure
- Immunosuppression - for vasculitis/DAH
- Tranexamic acid - antifibrinolytic; used increasingly but evidence still evolving
- Bevacizumab/VEGF inhibitors - associated with life-threatening hemoptysis in squamous NSCLC - use with caution or avoid
Key Points
- Death from hemoptysis = asphyxiation, not exsanguination
- Bronchial (high-pressure) circulation = source of most massive hemoptysis
- Life-threatening hemoptysis = only 5-15% of all hemoptysis cases
- CT chest identifies the source in ~70-88% of cases; superior to bronchoscopy for parenchymal causes
- BAE is the first-line intervention; surgery is reserved for failure/recurrence
- Always rule out pseudohemoptysis (epistaxis, hematemesis) before workup
Sources: Harrison's Principles of Internal Medicine, 22nd Ed. | Murray & Nadel's Textbook of Respiratory Medicine | Fishman's Pulmonary Diseases and Disorders
This is a shared conversation. Sign in to Orris to start your own chat.