Explain the structure configuration of hip joint in relation to weight bearing in unilateral and bilateral stance along with factors contributing for stability
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the material needed for a complete, well-illustrated answer. Let me compile it.
Hip Joint: Structure, Weight Bearing, and Stability
1. Basic Structural Configuration
The hip joint is a multiaxial ball-and-socket synovial joint between the spherical head of the femur and the acetabulum of the pelvic bone. It is designed primarily for stability and weight bearing, at some expense of mobility. It permits flexion, extension, abduction, adduction, medial/lateral rotation, and circumduction.
- Gray's Anatomy for Students, p. 661
Articular Surfaces
| Component | Detail |
|---|---|
| Femoral head | Nearly complete hemisphere; covered by hyaline cartilage except at the fovea |
| Acetabulum | "Cup" formed by ilium, ischium, and pubis; lined by the horseshoe-shaped lunate surface (widest superiorly, where load is greatest) |
| Acetabular fossa | Central non-articular area containing loose connective tissue and the ligament of the head of the femur |
The acetabulum nearly entirely encompasses the femoral head, which is the primary structural reason the hip is inherently more stable than the shoulder.
2. Capsule and Ligaments
The fibrous capsule is strong and thick. Medially it attaches to the acetabular margin and transverse acetabular ligament; laterally to the intertrochanteric line anteriorly and just proximal to the intertrochanteric crest posteriorly.
Three extracapsular ligaments spiral around the joint in a way that they become taut in extension, mechanically locking the joint during upright standing and reducing the muscular effort needed:
Iliofemoral Ligament (Y-ligament of Bigelow)
- Anterior to the joint; the strongest ligament in the body
- Triangular/Y-shaped; apex at anterior inferior iliac spine (AIIS) and acetabular margin; base at intertrochanteric line
- Superior band: taut in external rotation; inferior band: taut in extension
- Limits anterior translation during extension and external rotation
- Critical for standing posture (prevents hyperextension without continuous muscle work)
Pubofemoral Ligament
- Anteroinferior; from iliopubic eminence and obturator membrane to intertrochanteric region
- Taut in internal rotation and hyperabduction
- Weakest of the three
Ischiofemoral Ligament
- Reinforces the posterior capsule; from ischium posterior to acetabulum to the greater trochanter
- Limits posterior translation and internal rotation
- Prevents hyperextension posteriorly
All three ligament fiber bundles are oriented in a spiral/screw-home pattern so that full hip extension winds them tight, passively stabilizing the joint in the standing position.
- Imaging Anatomy - Bones, Joints, Vessels and Nerves, p. 739
- Gray's Anatomy for Students, p. 663
Zona Orbicularis
A deeper layer of circular transverse fibers encircles the femoral neck, forming the narrowest portion of the articular cavity. It merges with all three capsular ligaments and resists inferior distraction of the femoral head.
Acetabular Labrum
A fibrocartilaginous collar that deepens the socket, increases contact area, and creates a negative intra-articular pressure (suction-cup effect) that resists distraction. Inferiorly it bridges the acetabular notch as the transverse acetabular ligament, converting the notch into a foramen through which vessels and nerves pass.
Ligament of the Head of the Femur (Ligamentum Teres)
Runs from the fovea capitis to the acetabular fossa. Carries the acetabular branch of the obturator artery (small contribution to femoral head blood supply). Its mechanical role in stability is minor in adults but it limits adduction in flexion.
3. Weight Bearing: Bilateral Stance
In bilateral (double-limb) stance, body weight is distributed roughly equally across both hips. The pelvis is level and the center of gravity lies between the two feet, well within the base of support.
- The superiorly thickened lunate surface of each acetabulum bears most of the compressive load.
- Load on each femoral head is approximately one-third of body weight (body weight minus the weight of the legs divided by two).
- All three capsular ligaments contribute to passive stability; muscular demand is minimal.
- The spiral orientation of the ligaments passively locks the joint in extension with minimal energy cost.
4. Weight Bearing: Unilateral (Single-Limb) Stance
This is the biomechanically demanding situation - it represents the stance phase of normal walking, and the hip must withstand much greater forces.
The Lever Arm Problem
Body weight can be thought of as a load applied to a lever arm extending from the body's center of gravity to the center of the femoral head (the long arm). The hip abductors insert at the greater trochanter and act on a much shorter lever arm from the trochanter to the femoral head center.
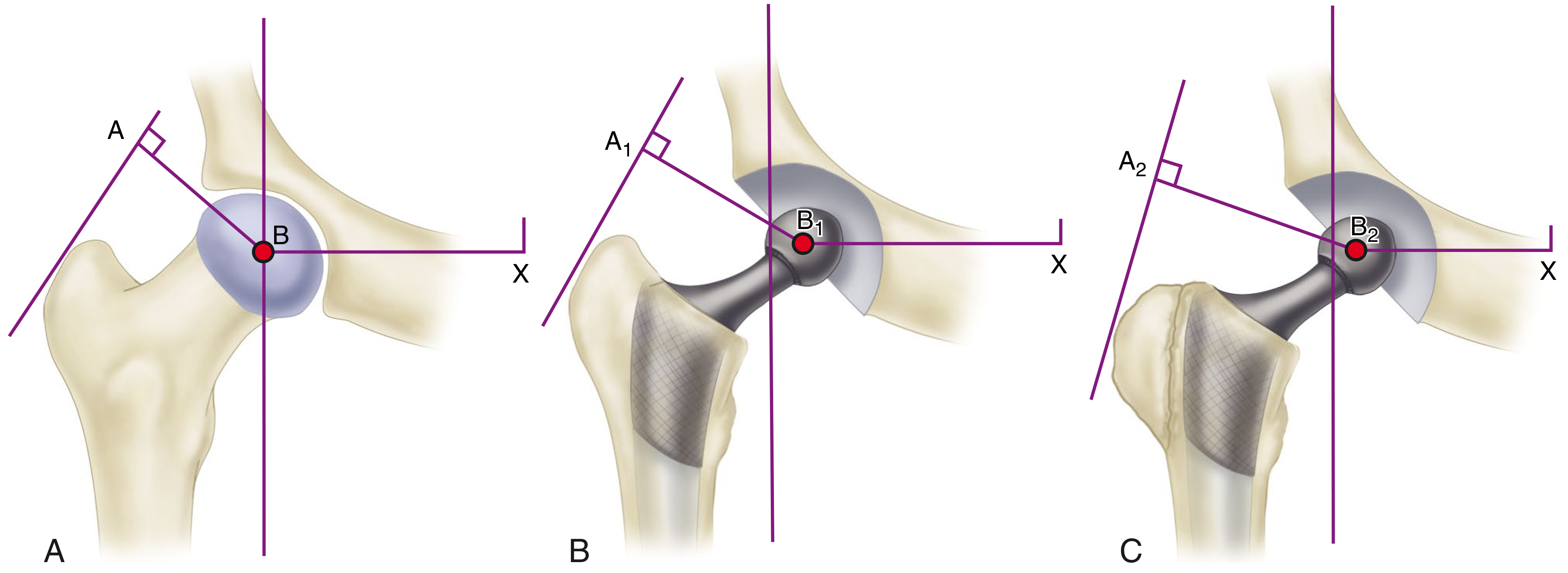
Lever arms at the hip. A = abductor force insertion; B = center of femoral head; X = body's center of gravity. The abductor lever arm (A-B) is much shorter than the body weight lever arm (B-X).
The ratio of the body weight lever arm to the abductor lever arm is approximately 2.5:1. This means:
-
The abductors must generate 2.5 × body weight of force to keep the pelvis level
-
Total joint contact force = abductor force + body weight superimposed = approximately 3 × body weight during single-leg stance
-
During running and jumping this can reach 8-10 × body weight
-
Campbell's Operative Orthopaedics, p. 227; Bailey and Love's, Summary Box 39.2
Hip Abductor Moment in Single-Limb Stance
The ground reaction force (GRF) passes medial to the hip joint axis of rotation, creating an external hip adduction moment that would rotate the pelvis clockwise (contralateral side drops). The hip abductors (gluteus medius, gluteus minimus, tensor fascia lata) must generate an equal and opposite internal hip abduction moment to keep the pelvis level.
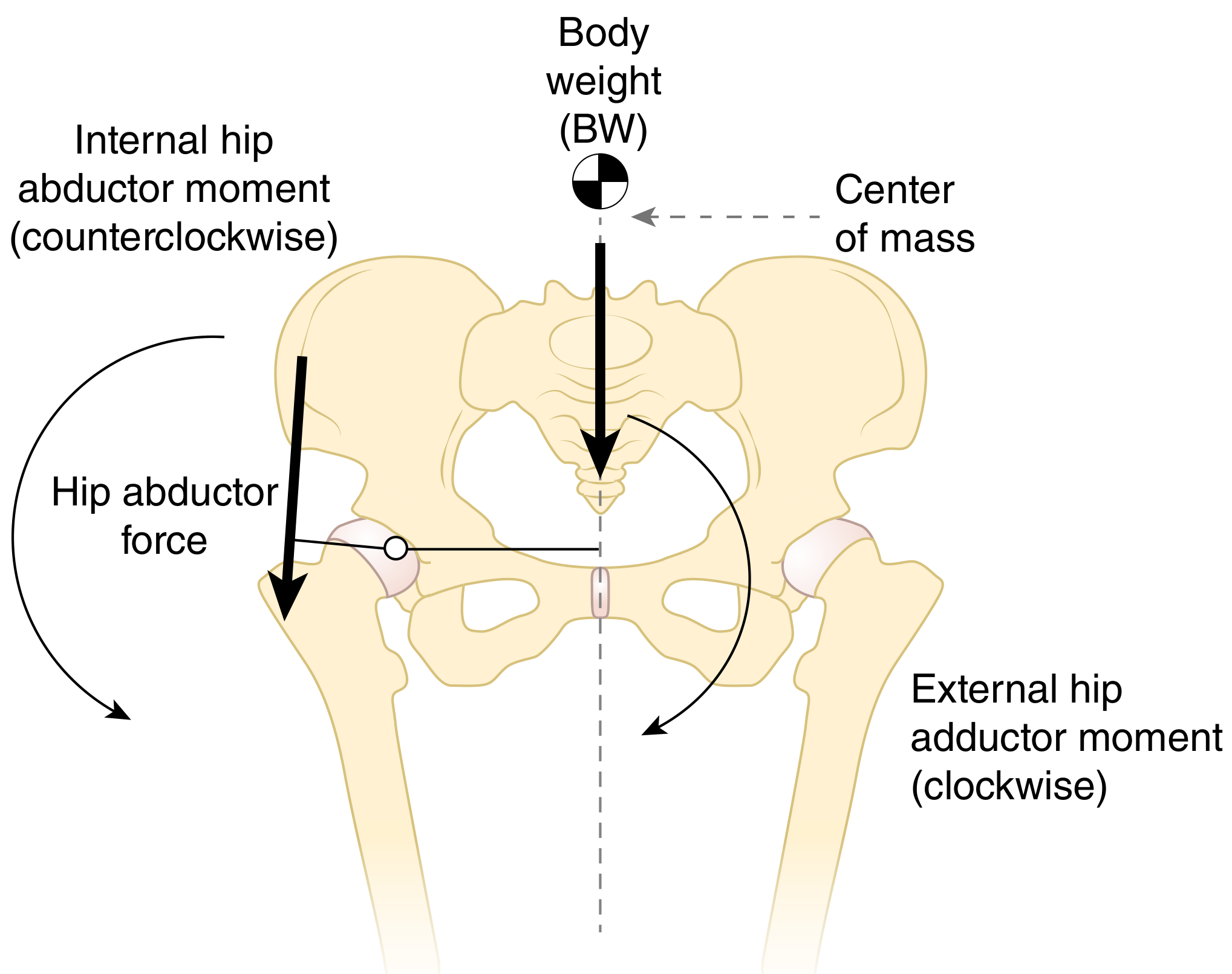
If the internal abductor moment equals the external adduction moment, the pelvis remains level. If it is insufficient, the contralateral pelvis drops - Trendelenburg sign.
Trendelenburg Sign
When the abductor mechanism fails (weak muscles, painful hip, disrupted lever arm), the unsupported side of the pelvis drops during single-leg stance on the affected side - this is a positive Trendelenburg sign. The patient may compensate by leaning the trunk over the affected hip (Trendelenburg lurch/gait) to shift the body's center of gravity over the stance leg, reducing the required abductor moment.
- Firestein & Kelley's Rheumatology, p. 131; Campbell's Operative Orthopaedics, p. exam chapter
5. Factors Contributing to Hip Joint Stability
Stability at the hip is achieved through multiple reinforcing mechanisms:
A. Bony Architecture
- Deep, cup-shaped acetabulum nearly fully encompasses the femoral head - greatest bony constraint of any synovial joint
- Superiorly thickened cartilage (lunate surface broadest superiorly) matches the weight-bearing zone
- The angle of inclination (normal ~126°) and angle of anteversion (~15°) orient the femoral head optimally within the acetabulum
B. Acetabular Labrum
- Deepens the socket by extending the articular surface by ~22%
- Creates a suction seal (negative intra-articular pressure) resisting distraction
- Acts as a gasket, retaining synovial fluid for lubrication
- Damage significantly reduces stability and predisposes to osteoarthritis
C. Capsule and Ligaments (Passive Stability)
- Thick fibrous capsule encasing the entire joint
- Spiral orientation of all three ligaments - become taut in extension (standing position), providing passive lock
- Iliofemoral ligament: primary anterior stabilizer (strongest in the body)
- Ischiofemoral ligament: primary posterior stabilizer
- Zona orbicularis: resists inferior subluxation
D. Muscular Stabilizers (Dynamic/Active Stability)
These are the primary dynamic stabilizers:
| Muscle Group | Role |
|---|---|
| Gluteus medius & minimus | Primary hip abductors; prevent pelvic drop in single-limb stance; most important dynamic stabilizers |
| Gluteus maximus | Powerful extensor; resists hip flexion forces |
| Short external rotators (piriformis, obturators, gemelli, quadratus femoris) | Act as a "rotator cuff" of the hip; compress femoral head into acetabulum |
| Iliopsoas | Anterior stabilizer in flexion; increases intra-articular pressure |
| Rectus femoris | Assists anterior stabilization |
The abductor complex (gluteus medius/minimus) is the key dynamic stabilizer during gait. Any disruption - muscle weakness, painful inhibition, trochanteric insufficiency, shortening of the lever arm by loss of femoral offset - results in Trendelenburg gait.
E. Atmospheric Pressure and Synovial Fluid
- Negative intra-articular pressure (maintained by the labral seal) contributes ~25% of resistance to distraction
- Synovial fluid provides lubrication and distributes load
F. Femoral Offset and Lever Arm Geometry
- Normal offset (horizontal distance from femoral head center to femoral shaft axis) is critical for abductor efficiency
- Reducing offset (as in coxa valga, or with a low-offset THA stem) shortens the abductor lever arm, requiring greater muscle force for the same moment, which increases joint contact force
- Coxa vara increases the abductor lever arm (A-B longer) - less force needed, but may affect joint congruence
Summary Table: Unilateral vs. Bilateral Stance
| Parameter | Bilateral Stance | Unilateral Stance |
|---|---|---|
| Base of support | Both feet - wide base | One foot - narrow base |
| Load per hip | ~1/3 body weight | ~3× body weight |
| Abductor demand | Minimal | High (must generate 2.5× BW) |
| Main stabilizing mechanism | Passive ligaments (spiral lock in extension) | Active abductor musculature |
| Pelvis | Level, no muscle-dependent stabilization needed | Level only if abductors generate adequate moment |
| GRF position | Between both feet | Medial to stance hip - creates adduction moment |
| Clinical test | Not applicable | Trendelenburg test |
Sources: - Gray's Anatomy for Students, pp. 661-664 - Campbell's Operative Orthopaedics 15th Ed, pp. 226-227 - Firestein & Kelley's Textbook of Rheumatology, pp. 130-131 - Bailey and Love's Short Practice of Surgery 28th Ed, Summary Box 39.2 - Imaging Anatomy - Bones, Joints, Vessels and Nerves, pp. 738-740
This is a shared conversation. Sign in to Orris to start your own chat.