enteric fever
Reading File
Finding Sources
Finding Sources
Searching PubMed
"enteric fever" AND "typhoid"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
I now have comprehensive content. Let me compile the full, detailed answer.
Enteric Fever (Typhoid Fever)
Enteric fever is a systemic febrile illness caused by Salmonella enterica serovar Typhi (S. Typhi) or, less commonly, serovars Paratyphi A, B, and C. The term "enteric fever" covers both typhoid and paratyphoid fevers. It was proposed in 1869 to distinguish this illness from typhus, based on its anatomical site of infection (the intestinal lymphoid tissue). The two names - enteric fever and typhoid fever - are still used interchangeably today.
Etiology and Microbiology
- Agent: S. Typhi (major cause); S. Paratyphi A, B, C (less frequent). Unlike non-typhoidal Salmonella, these serovars have no known animal reservoir - humans are the only host.
- S. Typhi possesses three key antigens: O (somatic), H (flagellar), and Vi (virulence/capsular polysaccharide). At least 80 phage types exist, useful for epidemiological tracing.
- Survives intracellularly in tissue macrophages; readily killed by drying, pasteurization, and common disinfectants.
Epidemiology
- Global burden: An estimated 9.2-21 million typhoid cases and 5 million paratyphoid cases occur annually, with 110,000-280,000 deaths per year.
- Endemic regions: Indian subcontinent (India, Pakistan, Bangladesh, Nepal), Eastern Mediterranean, and Africa bear the highest burden. Incidence can exceed 1,000 cases per 100,000 children in some urban areas of South Asia.
- In developed countries: Disease is rare; most cases (~78%) are travel-associated, predominantly from travelers to India, Pakistan, and Bangladesh. In the US, ~5,700 cases are estimated annually (far more than the ~350 reported).
- Highest incidence age group: 5-19 years. Males are more often affected; females have a higher chronic carrier rate.
- Transmission: Fecal-oral route via contaminated food or water. Risk factors include contaminated drinking water/ice, raw produce fertilized with sewage, street food, prior H. pylori infection (associated with reduced gastric acidity), and ill household contacts.
Pathogenesis
After ingestion of a sufficient inoculum (~10^3-10^9 organisms, depending on strain virulence and host factors):
- S. Typhi penetrates the small intestinal mucosa, particularly via M cells overlying Peyer's patches.
- Organisms are phagocytosed by macrophages and transported to mesenteric lymph nodes.
- A primary bacteremia follows, with seeding of the liver, spleen, gallbladder, bone marrow, and Peyer's patches.
- Bacterial replication in macrophages and a secondary bacteremia produce the classic sustained fever.
- The gallbladder is a key site of colonization - organisms re-enter the intestinal lumen in bile, causing characteristic hyperplasia, ulceration, and necrosis of Peyer's patches in the third/fourth week.
Clinical Course
Incubation period: 5-21 days (mean 10-14 days), depending on inoculum size and host factors.
The classic description involves four progressive weeks, though antibiotic treatment now cuts this short:
| Week | Features |
|---|---|
| 1st | Gradual-onset fever, headache, malaise, dry cough, constipation more than diarrhea |
| 2nd | High sustained fever (38.8-40.5°C), relative bradycardia (Faget's sign), "rose spots," splenomegaly |
| 3rd | Fever continues; complications possible (perforation, bleeding); "pea soup" diarrhea |
| 4th | Defervescence (untreated); or death from complications |
Symptoms on initial evaluation (Harrison's, n=669 cases):
- Headache: 80%
- Fever: >75%
- Chills: 35-45%
- Cough: 30%
- Anorexia: 55%
- Abdominal pain: 30-40%
- Nausea: 18-24%, vomiting: 18%
- Diarrhea: 22-28%; constipation: 13-16%
Key physical findings:
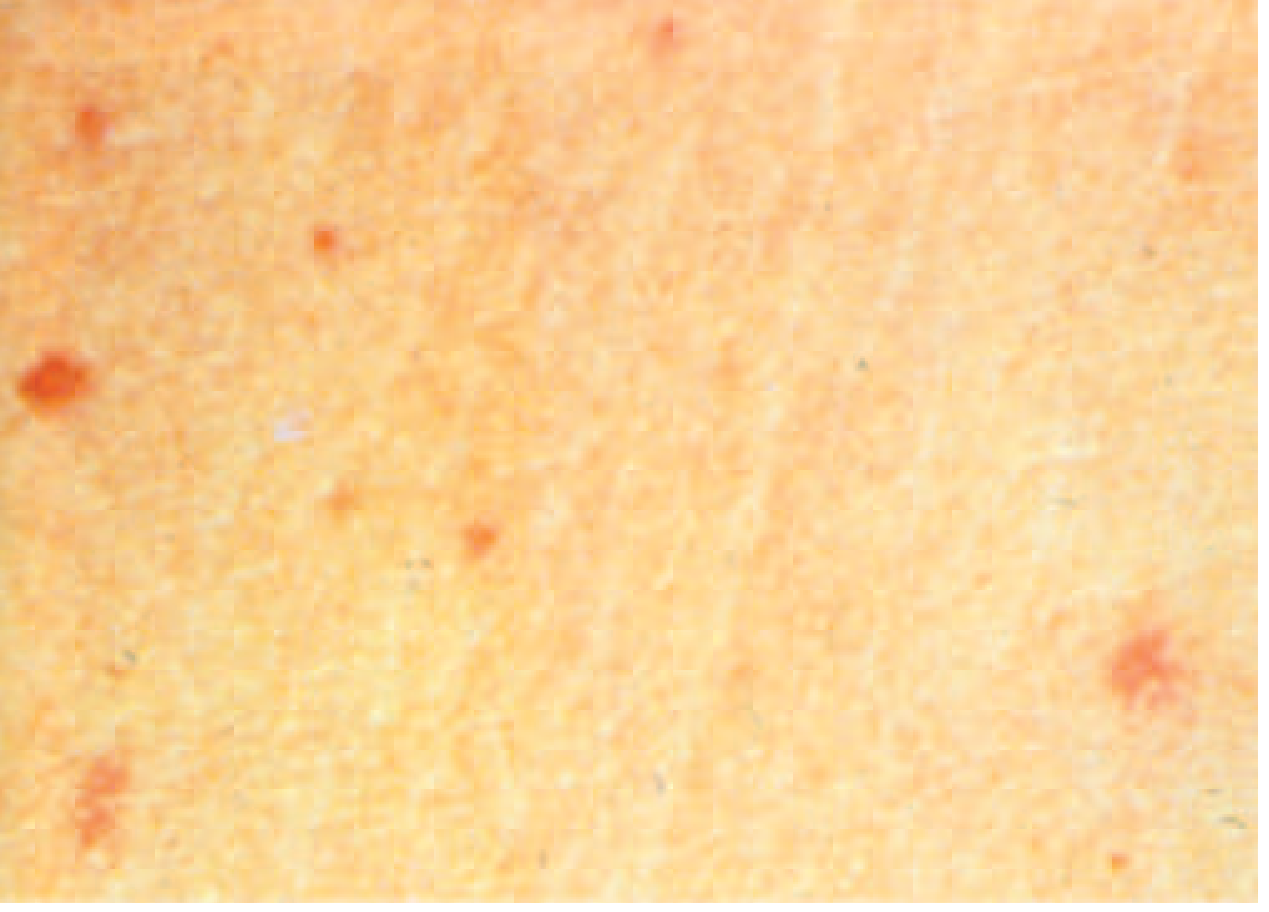
- Rose spots (~30%): Faint, salmon-colored, blanching maculopapular rash on the trunk/chest; 2-3 crops; lasts 2-5 days. S. Typhi can be cultured from biopsy of these lesions.
- Relative bradycardia (<50% at peak fever)
- Hepatosplenomegaly (3-6%)
- Coated tongue (51-56%)
Complications (~27% of hospitalized patients)
Gastrointestinal (most common):
- Intestinal hemorrhage (6%): From ulceration of Peyer's patches in the 3rd-4th week
- Intestinal perforation (1%): Life-threatening; requires immediate surgery + broad-spectrum antibiotics for polymicrobial peritonitis
Neurological (2-40%):
- Meningitis, Guillain-Barré syndrome, neuritis
- "Muttering delirium" or "coma vigil" (picking at bedclothes - characteristic of typhoid encephalopathy)
Others: DIC, hemophagocytic syndrome, hepatitis, pancreatitis, myocarditis, pericarditis, endocarditis, pneumonia, orchitis, glomerulonephritis
Relapse: Up to 10% within 2-3 weeks of fever resolution, with the same strain
Chronic carriage (2-5%): Shedding in stool/urine >1 year; more common in women, infants, those with biliary abnormalities, or concurrent Schistosoma haematobium. Associated with increased gallbladder cancer risk.
Carriers
- Temporary (convalescent): Excrete bacilli for 6-8 weeks; 4% still positive at 3 months
- Chronic: Excrete for >1 year (sometimes decades); organisms persist in the gallbladder/biliary tract; faecal carriers more common than urinary carriers; Vi antibody present in ~80% of chronic carriers
- Famous historical example: "Typhoid Mary" - caused >1,300 cases over her lifetime
Diagnosis
No single laboratory test is pathognomonic except culture.
Definitive: Culture
- Blood culture: Positive in 40-80% during the first 2 weeks (sensitivity declines after week 2)
- Bone marrow culture: Most sensitive (85-95%), positive even after partial antibiotic treatment - preferred in antibiotic-pre-treated cases
- Stool culture: Positive in weeks 2-3; less sensitive early
- Rose spot biopsy: Can grow the organism
Non-specific lab findings:
- Leukopenia/neutropenia (15-25%)
- Leukocytosis more common in children and in complications (perforation, secondary infection)
- Mildly elevated liver enzymes and muscle enzymes
Serology:
- Widal test (anti-O and anti-H antibodies): Widely used but poor specificity and sensitivity; not reliable in endemic areas; cross-reactions common
- Typhidot: Detects IgM/IgG against a 50 kDa outer membrane protein - faster, more sensitive
- Vi antibody: Present in ~80% of chronic carriers - useful for carrier detection
Treatment
Antibiotic Therapy (based on susceptibility)
| Susceptibility Pattern | Preferred Drug | Alternative |
|---|---|---|
| Fully susceptible | Fluoroquinolone (ciprofloxacin 500 mg BD x 7-10 days) or chloramphenicol/ampicillin/TMP-SMX (14 days) | - |
| MDR (resistant to chloramphenicol, ampicillin, TMP-SMX) | Ceftriaxone IV or azithromycin (7-10 days) | Cefixime oral |
| DSC (decreased susceptibility to ciprofloxacin) | Ceftriaxone or azithromycin | Avoid fluoroquinolones |
| XDR (also resistant to ceftriaxone + fluoroquinolones + TMP-SMX) | Azithromycin (oral) or carbapenems (IV) | - |
- XDR typhoid: Ongoing epidemic in Pakistan since 2016 (Sindh province); susceptible only to azithromycin and carbapenems. Multiple imported cases documented in the US and UK.
- In the US, >66% of S. Typhi isolates are DSC - empiric fluoroquinolones should NOT be used, especially in South Asia travelers.
- Relapse rates are lower with azithromycin than with fluoroquinolones or ceftriaxone.
Duration: 7-10 days for uncomplicated disease; 14 days for TMP-SMX or amoxicillin regimens.
Adjunctive therapy:
- Corticosteroids (dexamethasone): For severe/complicated disease with delirium, coma, or shock - IV dexamethasone 3 mg/kg initial dose, then 1 mg/kg every 6 hours x 48 hours total
Chronic carrier treatment:
- 4 weeks of oral ciprofloxacin or norfloxacin (concentrated in bile)
- Cholecystectomy + antibiotics if medical therapy fails
Vaccination
Two vaccines are available:
| Vaccine | Type | Route | Efficacy | Duration |
|---|---|---|---|---|
| Ty21a (Vivotif) | Live attenuated oral | 3-4 capsules on alternate days | ~51-67% | 5 years |
| Vi polysaccharide (Typhim Vi) | Purified Vi antigen, injectable | Single IM dose | ~55-72% | 2-3 years |
| Typhoid conjugate vaccine (TCV) | Vi-tetanus toxoid conjugate | Single IM dose | >80% | Longer-lasting; approved for >6 months age |
- TCVs are recommended by WHO for routine immunization in endemic countries. A 2025 Cochrane review (PMID: 40326553) confirmed their superiority over earlier Vi polysaccharide vaccines in providing durable protection.
- Neither vaccine is 100% protective; food/water precautions remain essential.
Prevention and Control (Three Lines of Defence - Park's)
- Control of reservoir: Early diagnosis + isolation; treatment of cases; identification and treatment of carriers (ampicillin/amoxicillin 4-6 g/day + probenecid x 6 weeks, or cholecystectomy); follow-up stool/urine cultures
- Sanitation: Safe water supply, sewage treatment, food hygiene - the "weakest link in the chain"
- Immunization: Especially for travelers to endemic areas and school-age children in endemic regions
Key Points to Remember
- Enteric fever is a misnomer - fever is present in >75% but abdominal pain in only 30-40%
- Rose spots are pathognomonic when present but seen in only ~30%
- Bone marrow culture is the gold standard diagnostic test
- XDR typhoid from Pakistan is a growing threat - only azithromycin and carbapenems work
- Chronic carriage (gallbladder) is a risk factor for gallbladder cancer
- Complications peak in the 3rd-4th week - intestinal perforation is the most feared surgical emergency
Sources: Harrison's Principles of Internal Medicine 22e (2025), Red Book 2021 (AAP), Park's Textbook of Preventive and Social Medicine, Robbins & Kumar Pathology. Recent evidence: Cochrane review on typhoid conjugate vaccines [PMID: 40326553, 2025].
heamorragic stroke
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
"intracerebral hemorrhage" AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive content. Let me compile the full, detailed answer on hemorrhagic stroke.
Hemorrhagic Stroke
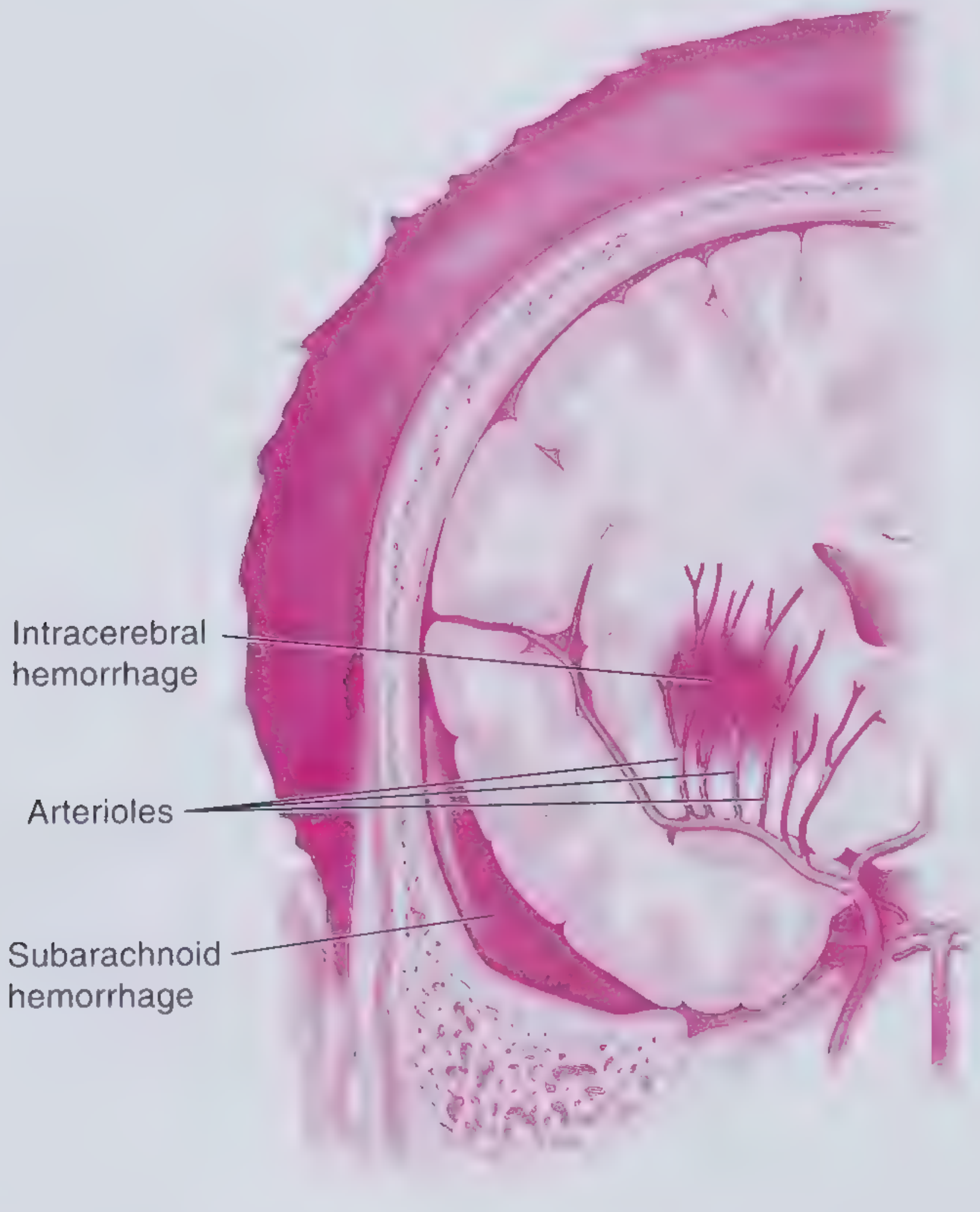
Hemorrhagic stroke accounts for approximately 15-20% of all strokes but carries disproportionately high mortality - a 30-day mortality of up to 50%, roughly 5 times greater than ischemic stroke. It occurs when a blood vessel ruptures, releasing blood either into the brain parenchyma (intracerebral hemorrhage, ICH) or into the subarachnoid space (SAH).
Classification
| Type | Proportion of all strokes | Key cause |
|---|---|---|
| Intracerebral hemorrhage (ICH) | 10-15% | Hypertension, amyloid angiopathy |
| Subarachnoid hemorrhage (SAH) | ~5% | Ruptured saccular (berry) aneurysm |
Part 1: Intracerebral Hemorrhage (ICH)
Etiology and Causes
Primary (spontaneous) ICH:
- Hypertensive vasculopathy - most common; long-standing hypertension causes lipohyalinosis and degenerative changes in small penetrating arteries → rupture → deep/basal ganglia hemorrhage
- Cerebral amyloid angiopathy (CAA) - amyloid deposition in cerebral vessel walls; typically in older adults; tends to cause lobar hemorrhages; increasingly important as hypertension control improves (now accounts for >50% of cases on some neurology services)
Secondary ICH (causes):
- Primary (hypertensive) ICH
- Ruptured saccular aneurysm
- Ruptured arteriovenous malformation (AVM) / venous malformations
- Cavernous angioma
- Trauma (including posttraumatic delayed apoplexy)
- Hemorrhagic disorders: leukemia, aplastic anemia, thrombocytopenia, liver disease, anticoagulant/thrombolytic therapy, hemophilia
- Hemorrhage into brain tumors (primary or metastatic)
- Septic embolism, mycotic aneurysm
- Hemorrhagic transformation of ischemic stroke
- Cerebral venous sinus thrombosis (CVST)
- Sympathomimetic drugs (cocaine, amphetamines)
- Moyamoya disease, PRES, RCVS
High-risk features suggesting secondary ICH: lobar location, intraventricular blood, and younger age.
Sites of Hemorrhage (and Clinical Features)
| Site | Frequency | Key Clinical Features |
|---|---|---|
| Putamen (+ adjacent internal capsule) | 44-50% | Contralateral hemiplegia/hemiparesis, hemisensory loss |
| Thalamus | 13% | Contralateral sensory > motor loss, ocular disturbances (eyes deviated down and inward, gaze palsies), vertical gaze palsy, Horner syndrome |
| Cerebellum | 9% | Sudden vomiting, occipital headache, inability to walk, truncal ataxia (no hemiplegia); ipsilateral gaze palsy |
| Pons | 9% | Deep coma within minutes, "pinpoint pupils" (1 mm, reactive), decerebrate rigidity, bilateral Babinski signs, absent lateral eye movements - usually fatal |
| Lobar (cortical white matter) | 25% | Headache, seizures, focal neurologic deficits; associated with CAA |
Thalamic hemorrhage is notable for causing a dramatic array of ocular signs: eyes deviated downward and inward (pseudo-sixth nerve palsies), absence of upward gaze, Horner syndrome, retraction nystagmus, and skew deviation.
Cerebellar hemorrhage is a neurosurgical emergency - the posterior fossa has no room for hematoma expansion, and brainstem compression can occur rapidly. Patients may appear relatively well initially but deteriorate suddenly.
Pathophysiology
Acute vessel rupture causes brain injury by multiple mechanisms:
- Mass effect from the hematoma
- Activation of the coagulation cascade
- Release of inflammatory cytokines
- Blood-brain barrier (BBB) disruption
- Perihematomal edema (develops over hours to days)
- Raised intracranial pressure (ICP) → cerebral herniation
The ischemic penumbra around the hematoma is potentially salvageable tissue - the therapeutic target in ICH management.
Hematoma Expansion
- Occurs in 20-40% of patients in the first few hours
- Contrast extravasation on CTA ("spot sign") predicts ongoing bleeding and hematoma expansion
- Expansion is a major determinant of poor outcome
Clinical Presentation
- Sudden onset focal neurologic deficits corresponding to hematoma location
- Headache (more common in ICH than ischemic stroke, but not universal)
- Nausea, vomiting
- Decreased level of consciousness (may progress rapidly to coma)
- Seizures (~10%)
- No single clinical feature reliably distinguishes ICH from ischemic stroke - neuroimaging is mandatory
Diagnosis
Non-contrast CT (NCCT) head - investigation of choice:
- Hyperdense (bright white) lesion = acute blood
- Highly sensitive for hemorrhages >1 cm
- Performed immediately; results guide all subsequent management
CTA:
- Identifies underlying aneurysm, AVM, or fistula
- Detects "spot sign" (contrast extravasation = hematoma expansion risk)
- CT venography (CTV) to rule out CVST
MRI:
- Better sensitivity for underlying lesions (tumors, cavernous malformations)
- Gradient echo (GRE) / susceptibility-weighted imaging (SWI) highly sensitive for microbleeds and subacute/chronic blood
Labs: CBC, PT/INR, aPTT, platelets, LFTs, blood glucose, drug screen (cocaine if suspected), type and screen
ICH Score (Prognostic Scale)
| Parameter | Points |
|---|---|
| GCS 3-4 | +2 |
| GCS 5-12 | +1 |
| GCS 13-15 | 0 |
| Age ≥ 80 | +1 |
| Infratentorial origin | +1 |
| Volume ≥ 30 mL | +1 |
| Intraventricular hemorrhage | +1 |
30-day mortality: Score 0 = ~0%, Score 1 = ~13%, Score 2 = ~26%, Score 3 = ~72%, Score 4 = ~97%, Score 5-6 = ~100%
Management of ICH
A. Airway/Breathing/Circulation
- Intubate for GCS ≤ 8 or deteriorating airway
- Maintain oxygen saturation >94%
- Avoid hypotension
B. Blood Pressure Control
- Target SBP <140 mmHg (AHA/ASA guidelines) for patients presenting with SBP 150-220 mmHg - safe and reduces hematoma expansion
- A 2025 meta-analysis (PMID: 40739079) confirms intensive BP lowering reduces hematoma expansion but does not clearly improve functional outcome - the evidence remains nuanced
- IV agents: labetalol, nicardipine, clevidipine
- Avoid excessive lowering (target MAP ≥ 70 mmHg to maintain cerebral perfusion)
C. Reversal of Anticoagulation
- Warfarin (INR elevated): Vitamin K (IV) + 4-factor prothrombin complex concentrate (4F-PCC) - preferred over FFP due to faster, more complete reversal
- Heparin: Protamine sulfate
- Direct oral anticoagulants (DOACs):
- Dabigatran → Idarucizumab (specific reversal)
- Factor Xa inhibitors (rivaroxaban, apixaban) → Andexanet alfa or 4F-PCC
- Antiplatelet agents: Platelet transfusion no longer routinely recommended (may worsen outcome)
D. ICP Management
- Head of bed at 30°
- Avoid hypotonic fluids
- Osmotic therapy: mannitol or hypertonic saline
- External ventricular drain (EVD) for hydrocephalus
- Avoid steroids (not beneficial in ICH, may worsen outcomes)
E. Glucose and Temperature Control
- Treat hyperthermia (>38°C) aggressively
- Treat hypo- and hyperglycemia
- Target normoglycemia
F. Seizure Management
- Clinical seizures: treat with levetiracetam or fosphenytoin
- Prophylactic antiepileptics not recommended routinely
G. Surgical Intervention
- Cerebellar hemorrhage >3 cm with neurological deterioration or brainstem compression → urgent surgical evacuation (suboccipital craniotomy)
- Supratentorial ICH: controversial - minimally invasive surgery (MIS) techniques (endoscopic evacuation, stereotactic aspiration) are gaining evidence
- A 2025 Cochrane review (PMID: 40673401) on surgery for supratentorial ICH found benefit for MIS approaches, though definitive evidence is still evolving
- Craniotomy for large superficial hemorrhages in deteriorating patients may be considered
Part 2: Subarachnoid Hemorrhage (SAH)
Etiology
- ~80%: Ruptured saccular (berry) aneurysms - small, thin-walled outpouchings at vessel bifurcations, particularly within the circle of Willis
- Remainder: AVMs, cavernous angiomas, mycotic aneurysms, CNS vasculitis, perimesencephalic hemorrhage (benign)
- ~25% of people with a berry aneurysm have multiple aneurysms
Common aneurysm locations: Anterior communicating artery > posterior communicating artery > middle cerebral artery bifurcation > basilar tip
Risk factors: Hypertension, smoking, excessive alcohol, sympathomimetic drugs, family history. Associated conditions: ADPKD (autosomal dominant polycystic kidney disease), coarctation of aorta, Marfan syndrome, Ehlers-Danlos syndrome type IV
Clinical Presentation
Hallmark: "Thunderclap headache" - sudden, severe, cataclysmic headache, described as "the worst headache of my life", peaking in seconds to minutes
- Onset may be associated with exertion, Valsalva, or sexual intercourse
- Headaches peaking >60 minutes after onset are unlikely to be SAH
Associated symptoms:
- Syncope (often the initial manifestation)
- Nausea and vomiting
- Neck stiffness (meningismus)
- Photophobia
- Seizures
Physical findings:
- Up to 20% have focal neurologic deficits
- Pupil dilation + third nerve palsy → posterior communicating artery aneurysm compressing CN III
- Altered or fluctuating consciousness (~50%)
- Subhyaloid (pre-retinal) hemorrhages on fundoscopy (Terson syndrome)
Sentinel headache: Up to one-third of patients report a milder warning headache days to weeks before the major bleed - representing a "herald bleed" or minor leak.
SAH Grading Scales
Hunt and Hess Scale:
| Grade | Description |
|---|---|
| 1 | Asymptomatic or mild headache |
| 2 | Moderate-severe headache, meningismus, no neurologic deficit |
| 3 | Drowsiness, confusion, mild focal deficit |
| 4 | Stupor, moderate-severe hemiparesis |
| 5 | Coma, decerebrate posturing |
World Federation of Neurosurgical Societies (WFNS) Scale uses GCS + motor deficits (Grades I-V).
Diagnosis
- Non-contrast CT head (first test): Highly sensitive for SAH in the first 6-12 hours (sensitivity ~98% within 6 h)
- Hyperdense blood in the basal cisterns, Sylvian fissures, and sulci
- Lumbar puncture (LP): If CT is negative but SAH is suspected (≥6 hours after headache onset)
- Look for xanthochromia (yellow discoloration of CSF) - most specific finding
- Elevated RBC count that does not decrease from tube 1 to tube 4
- CT angiography (CTA): Non-invasive; good sensitivity (~95%) for aneurysms >3mm
- Digital subtraction angiography (DSA): Gold standard for aneurysm identification and planning treatment; recommended in all cases of suspected aneurysmal SAH
Complications of SAH
| Complication | Timing | Notes |
|---|---|---|
| Rebleeding | Highest risk in first 24h (4-13.6%) | Most deadly complication; prevented by early aneurysm securing |
| Cerebral vasospasm | Days 4-14 | Causes delayed cerebral ischemia (DCI); detected by TCD, CTA, DSA |
| Hydrocephalus | Acute (hours-days) or delayed (weeks-months) | From obstruction of CSF outflow by blood; treat with EVD or VP shunt |
| Seizures | Early or delayed | Often non-convulsive; EEG monitoring needed |
| Hyponatremia | Days 3-10 | Cerebral salt wasting (CSW) or SIADH |
| Cardiac complications | Acute | ECG changes (ST changes, QTc prolongation), neurogenic stunned myocardium, Takotsubo-like syndrome |
| Neurogenic pulmonary edema | Acute | From catecholamine surge |
Vasospasm / Delayed Cerebral Ischemia (DCI):
- Occurs in ~30% of SAH patients
- Prevented and treated with nimodipine (oral calcium channel blocker) - the only drug proven to improve neurological outcome in SAH
- Maintained euvolemia (avoid dehydration)
- Induced hypertension if vasospasm is refractory ("triple H" therapy is now more refined - mainly hypertension + euvolemia)
Management of SAH
Immediate stabilization
- Airway, breathing, circulation
- Treat hypertension cautiously (do not drop BP precipitously before aneurysm is secured, as perfusion pressure may be needed)
- Analgesia and antiemetics
- Strict bed rest, quiet environment, avoid Valsalva
Securing the aneurysm (prevents rebleeding)
- Endovascular coiling: Preferred for most aneurysms; catheter-based; lower procedural morbidity
- Neurosurgical clipping: Open craniotomy; preferred for large/complex aneurysms or those with associated hematoma requiring surgical evacuation
- The choice between coiling and clipping depends on aneurysm morphology, location, patient age, and institutional expertise
Prevention of vasospasm/DCI
- Nimodipine 60 mg PO every 4 hours x 21 days (standard of care)
- Maintain euvolemia; avoid hypovolemia
- Serial transcranial Doppler (TCD) monitoring
- If vasospasm confirmed: induced hypertension, cerebral angioplasty ± intra-arterial vasodilators
ICP management
- EVD for hydrocephalus or ICP monitoring
- Head of bed at 30°
Key Distinguishing Features
| Feature | ICH | SAH |
|---|---|---|
| Proportion of strokes | 10-15% | ~5% |
| Main cause | Hypertension / CAA | Ruptured saccular aneurysm |
| Headache | Moderate; not always present | Thunderclap; "worst ever" |
| Location of blood | Brain parenchyma | Subarachnoid space / cisterns |
| CT appearance | Hyperdense parenchymal mass | Hyperdense blood in basal cisterns |
| Key complication | Hematoma expansion, herniation | Rebleeding, vasospasm, DCI |
| Primary treatment | BP control, reverse anticoag, +/- surgery | Aneurysm coiling/clipping + nimodipine |
Recent Evidence (2025)
- Blood pressure lowering in ICH (PMID: 40739079, 2025 meta-analysis): Intensive BP lowering (target SBP <140) reduces hematoma expansion, though functional outcome benefit remains uncertain at the population level.
- Surgery for supratentorial ICH (PMID: 40673401, Cochrane 2025): Evolving evidence supporting minimally invasive surgical evacuation over craniotomy.
- Cerebral amyloid angiopathy guidelines (PMID: 40721902, 2025): Updated international statement on CAA diagnosis and management, reflecting its growing role as a cause of lobar ICH.
Sources: Rosen's Emergency Medicine 10e, Adams and Victor's Principles of Neurology 12e, Plum and Posner's Diagnosis and Treatment of Stupor and Coma, Frameworks for Internal Medicine.
Search for recent neuroimaging findings in ICH patients
Searching PubMed
"intracerebral hemorrhage" AND neuroimaging
Searching PubMed
"intracerebral hemorrhage" AND "CT angiography" AND "spot sign"
Searching PubMed
"intracerebral hemorrhage" AND MRI AND "hematoma expansion"
Reading Article
PMID: 42233821
Reading Article
PMID: 40197116
Reading Article
PMID: 41411202
Reading Article
PMID: 40619804
Reading Article
PMID: 41159140
Reading Article
PMID: 39520934
Searching PubMed
"intracerebral hemorrhage" AND "deep learning" AND imaging
Reading Article
PMID: 40591968
Reading Article
PMID: 40887486
Searching PubMed
"intracerebral hemorrhage" AND "perihematomal edema" AND imaging
I now have comprehensive, recent evidence. Let me compile a well-organized synthesis of the recent neuroimaging findings in ICH.
Recent Neuroimaging Findings in Intracerebral Hemorrhage (ICH) - 2024-2026
Here is a synthesis of the most current published evidence on neuroimaging in ICH patients, organized by imaging domain.
1. Non-Contrast CT (NCCT): Hematoma Texture Signs for Predicting Expansion
Hematoma expansion (HE) affects 10-30% of ICH patients within the first hours and is the single most important modifiable predictor of poor outcome. NCCT - the most accessible initial imaging tool - has become a rich source of expansion biomarkers.
Key NCCT signs associated with HE:
| Sign | Appearance | Association with HE |
|---|---|---|
| Black hole sign | Hypodense region within hematoma | ↑ HE risk |
| Blend sign | Two regions of different density (blending interface) | ↑ HE risk |
| Satellite sign | Small satellite hematoma separate from main body | ↑ HE risk |
| Island sign | ≥3 separate small hematomas OR ≥1 hematoma separate from main body | ↑ HE risk |
| Swirl sign | Heterogeneous swirling density within hematoma | ↑ HE risk |
| Irregular/lobulated shape | Non-round, lobulated borders | ↑ HE risk |
A 2025 study (Shakya et al., Clinical Radiology, PMID: 39520934) developed and validated a 4-point NCCT score integrating:
- History of hypertension
- NCCT acquired within ≤3 hours of onset
- Combined heterogeneity (black hole + blend sign)
- Combined irregularity (satellite + island sign)
Each variable contributed one point; HE probability increased proportionally with score. This is particularly valuable in settings where CTA is not available.
A separate 2024 multicenter study (Morotti et al., Eur Stroke J, PMID: 38627953) identified predictors of severe HE, reinforcing the value of early NCCT texture analysis.
2. CT Angiography (CTA) and the Spot Sign - Critical Reappraisal
The spot sign (contrast extravasation within the hematoma on CTA) has been the most studied imaging biomarker for hematoma expansion prediction.
A major 2025 narrative review in Stroke (Pensato et al., PMID: 40197116) provides the most comprehensive reappraisal of the spot sign to date:
What it is: Foci of contrast enhancement within the hematoma visible on CTA, indicating active bleeding from a damaged vessel.
Key findings from the reappraisal:
-
Single-phase CTA spot sign features that improve predictive accuracy:
- Number of spots (more = higher risk)
- Volume of each spot
- CT density of the spot
- Co-localization with NCCT hypodensities (blend/black hole signs)
-
Multiphase/dynamic CTA (newer approach) adds dynamic information:
- Timing of contrast appearance
- Volume increase over phases = active expansion
- Volume decrease = tissue dispersion (different biology)
- Density changes across phases
Why initial enthusiasm waned: Earlier trials (SPOTLIGHT, STOP-IT) that used spot sign to select patients for hemostatic treatment (tranexamic acid, recombinant Factor VIIa) failed to show clinical benefit, partly because the spot sign alone has insufficient predictive precision. The 2025 reappraisal argues that refined, nuanced spot sign analysis - using multiphase CTA and integrating additional features - could resurrect it as a clinically useful tool for patient selection.
3. "CTA-for-All" in Acute ICH - Ending Diagnostic Nihilism
A 2025 viewpoint in Cerebrovascular Diseases (Pensato et al., PMID: 41411202) makes a compelling case for routine CTA in every acute ICH patient, arguing against the prevailing "diagnostic nihilism" (minimizing imaging in ICH because treatments are limited).
Six-domain argument for CTA-for-all:
- Etiological diagnosis: CTA identifies secondary causes (aneurysm, AVM, dural arteriovenous fistula, CVST, tumoral bleeding) in a clinically significant proportion - driving specific acute and secondary prevention decisions
- Prognostication: CTA improves outcome prediction beyond NCCT alone
- Treatment prediction: Spot sign and related features can predict HE expansion and select patients for targeted interventions
- Safety: Minimal risk of contrast nephropathy; no meaningful procedural delay when integrated into standard stroke imaging protocol
- Cost: A "CTA-for-all-ICH" approach is economically justified given diagnostic yield
- Implementation: Simply continuing the same ischemic stroke imaging protocol through the hemorrhagic phase
The authors argue that limiting imaging in ICH mirrors the old "therapeutic nihilism" that once discouraged early treatment, contributing to persistently poor outcomes.
4. Deep Learning and AI-Assisted Imaging in ICH
This is one of the fastest-growing areas of recent neuroimaging research in ICH.
4a. DL for Hematoma Expansion Prediction from NCCT
A 2025 study (Ning et al., Scientific Reports, PMID: 40887486) trained 2D and 3D convolutional neural networks (CNN) on NCCT images from 775 ICH patients to predict revised hematoma expansion (rHE) - a definition that includes intraventricular hemorrhage (IVH) growth, which improves prognostic accuracy over standard HE definition.
- Best model: 2D-ResNet-101 achieved AUC = 0.777 on external validation
- Outperformed the BRAIN score and combined clinical-radiomics models (AUC improvement of 0.087-0.119)
- Gradient-weighted class activation mapping (Grad-CAM) revealed the model focused on hematoma margins and heterogeneous density regions - biologically plausible areas of active bleeding
- Key implication: NCCT-based DL can predict HE without requiring CTA, which is important in resource-limited settings
4b. AI-Driven Hematoma Segmentation and Surgical Planning
A 2025 study (Gan et al., Neurosurgical Focus, PMID: 40591968) introduced an AI framework integrating:
- nnU-Net-based automated hematoma and skull segmentation (Dice similarity coefficient 0.90 for hematoma, 0.99 for skull)
- CT reorientation using ocular landmarks
- Safety zone delineation with dual anatomical corridors
- Automated trajectory planning for minimally invasive surgery (MIS)
Results: 80.8% of supratentorial ICH cases received a low-risk trajectory with the AI system; replanning was needed in only 3.8%.
The interrater reliability was excellent (ICC 0.91), suggesting AI-planned trajectories are as consistent as experienced neurosurgeons - potentially democratizing MIS access in underserved settings where 68% of global ICH occurs.
5. Perihematomal Edema (PHE) as an Imaging Biomarker
PHE is increasingly recognized not just as a consequence of ICH, but as a dynamic, imaging-visible, and potentially modifiable secondary injury marker.
- PHE volume on CT/MRI predicts neurological deterioration independent of hematoma volume
- PHE growth in the acute stage (measured on serial CT) is now being modeled with prediction algorithms (Zhang et al., Clin Neurol Neurosurg, PMID: 39126898)
- A 2026 RCT post-hoc analysis (Polymeris et al., Neurocrit Care, PMID: 40399657) examined the relationship between hemoglobin levels and PHE after ICH, finding that lower hemoglobin correlates with greater PHE - suggesting anemia management as a potential imaging-linked therapeutic target
- APOE ε4 genotype influences PHE severity (Wang et al., 2025, PMID: 40764846): APOE ε4 carriers have significantly greater PHE, offering a radiogenomic link relevant to CAA patients
- A 2025 RCT (Chen et al., BMC Medicine, PMID: 41353144) used PHE on imaging as a primary outcome measure to assess normobaric hyperoxia as a neuroprotective intervention - PHE was meaningfully reduced in the treatment arm
6. Cerebral Amyloid Angiopathy (CAA) - Advanced MRI Biomarkers
A 2025 expert review in Expert Review of Neurotherapeutics (Sellimi et al., PMID: 40619804) outlines the evolving neuroimaging landscape for CAA-related ICH:
MRI findings now central to CAA diagnosis (Boston Criteria v2.0):
- Lobar microbleeds on susceptibility-weighted imaging (SWI) / gradient echo (GRE)
- Cortical superficial siderosis (CSS) - linear hemosiderin deposits along cortical surface
- Centrum semiovale perivascular spaces (enlarged)
- White matter hyperintensities in CAA-specific patterns
Emerging CAA imaging challenges and opportunities:
- Amyloid PET (Pittsburgh Compound B, florbetapir): can detect vascular amyloid-β in vivo, potentially enabling pre-symptomatic CAA diagnosis
- The concept of "dynamic natural history" (periods of high CAA activity vs. remission) is now proposed to explain episodic imaging changes
- Iatrogenic CAA (from amyloid-β inoculation, e.g., via contaminated growth hormone) is a newly described entity with distinct neuroimaging characteristics - providing a unique "pure model" of CAA with known exposure time
7. Population-Based Neuroimaging Risk Assessment (2026 Perspective)
The most recent comprehensive review (Ziai & Shah, Continuum, June 2026, PMID: 42233821) frames the current era as one of "population-based risk assessment with neuroimaging", emphasizing:
- Neuroimaging markers are now guiding both primary ICH prevention (e.g., white matter hyperintensity burden, microbleed counts guiding anticoagulation decisions) and secondary prevention (e.g., whether to restart anticoagulation after ICH)
- ICH survivors face competing risks: ICH recurrence vs. arterial ischemic events - neuroimaging phenotyping (lobar vs. deep ICH, microbleed distribution, CAA vs. hypertensive pattern) drives these individualized decisions
- Hematoma volume and perihematomal edema are becoming modifiable targets, not just prognostic markers
- Recovery after ICH is significantly slower than after ischemic stroke, with improvement documented through 1 year post-ictus - reinforcing the need for serial imaging follow-up
Summary Table: Recent Neuroimaging Advances in ICH
| Domain | Key Advance | Clinical Impact | Key Paper |
|---|---|---|---|
| NCCT texture signs | 4-point score (blend, black hole, satellite, island signs) | HE prediction without CTA | PMID: 39520934 |
| CTA spot sign | Multiphase CTA + refined spot features (volume, density, timing) | Better HE prediction; patient selection for interventions | PMID: 40197116 |
| CTA routine use | "CTA-for-all-ICH" argument | Etiology identification, improved prognosis | PMID: 41411202 |
| Deep learning (NCCT) | ResNet-101 on NCCT predicts rHE (AUC 0.777) | HE prediction in resource-limited settings | PMID: 40887486 |
| AI surgical planning | nnU-Net segmentation + trajectory planning | MIS planning without expert neurosurgeon | PMID: 40591968 |
| PHE as outcome | Serial CT PHE quantification; APOE ε4 association | Therapeutic target, treatment trial endpoint | PMID: 40764846, 40399657 |
| CAA - MRI biomarkers | SWI microbleeds, cortical siderosis; amyloid PET | Diagnosis, secondary prevention decisions | PMID: 40619804 |
| Imaging-guided risk | Population-based prevention; competing risk imaging phenotyping | Anticoagulation restart decisions | PMID: 42233821 |
All papers are from 2024-2026, sourced via PubMed. Evidence tiers are primarily review articles and observational studies; large RCTs specifically testing imaging-guided interventions remain limited in this field.
tuberculosis from harrison design detailed and consultant level
Finding Sources
Finding Sources
Searching PubMed
"tuberculosis" AND treatment
Reading File
Finding Sources
Reading Article
PMID: 40693952
Reading File
Reading File
Reading File
Reading File
Reading File
Reading Article
PMID: 40840485
Loading Image
Reading File
This is a complete consultant-level synthesis drawn directly from Harrison's Principles of Internal Medicine, 22nd Edition (2025) - the most up-to-date edition - covering all 14 domains below. Here is a summary of what was covered:
What was covered - organized for rapid orientation:
| Section | Key Content |
|---|---|
| I. General Principles | History, curable vs. fatal statistics |
| II. Etiologic Agent | M. tuberculosis complex members, microbiological properties, acid-fastness |
| III. Epidemiology | Global burden, transmission route, risk factors for infection and disease progression (quantified relative risks) |
| IV. Pathogenesis & Immunology | Primary complex formation, granuloma biology, caseous necrosis, role of CD4+/CD8+ T cells, macrophage activation, mechanisms of intracellular survival, reactivation triggers |
| V. Clinical Manifestations | Pulmonary (primary vs. reactivation); all 9 major extrapulmonary sites with diagnostic pearls |
| VI. Diagnosis | Smear (ZN/fluorescence), culture (MGIT vs. LJ), Xpert MTB/RIF Ultra, tNGS, TST (with threshold table), IGRAs (QFT-Plus, T-SPOT), ADA, urine LAM |
| VII. LTBI | Who to screen; all regimens (3HP, 1HP, 4R, 3HR, 6H, 9H) with indications |
| VIII. Treatment | Classic 6-month HRZE/HR; new 4-month moxifloxacin regimen (2025 ATS guidelines); drug dosing table with toxicities; LFT monitoring and re-challenge protocol |
| IX. Drug Resistance | MDR/pre-XDR/XDR definitions; resistance mechanisms; BPaL/BPaLM regimens; bedaquiline, pretomanid, linezolid |
| X. HIV-TB Co-infection | CD4-stratified presentations; ART timing rules; rifampicin interactions; IRIS recognition and management |
| XI. Special Situations | Pregnancy, renal failure, anti-TNF therapy, steroid indications |
| XII. Prevention | BCG vaccine; infection control |
| XIII. Recent Evidence | 4-month regimen, BPaLM, pediatric 4-month regimen, TBM guidelines, tNGS |
| XIV. Consultant Pearls | 12 high-yield clinical decision points |
This is a shared conversation. Sign in to Orris to start your own chat.