Diabetic keto acidosis treatment
Reading File
Finding Sources
Searching PubMed
"diabetic ketoacidosis"[MeSH Terms] AND treatment
Reading File
Reading File
Finding Sources
Reading File
Loading Image
I now have comprehensive textbook content and a clear DKA treatment algorithm. Let me compile a thorough response.
Diabetic Ketoacidosis (DKA) - Treatment
Overview
DKA is an acute, life-threatening complication of diabetes characterized by hyperglycemia, ketosis, and metabolic acidosis. Management ideally takes place in an ICU. The three pillars of treatment are: fluid replacement, insulin administration, and potassium repletion.
Treatment Algorithm
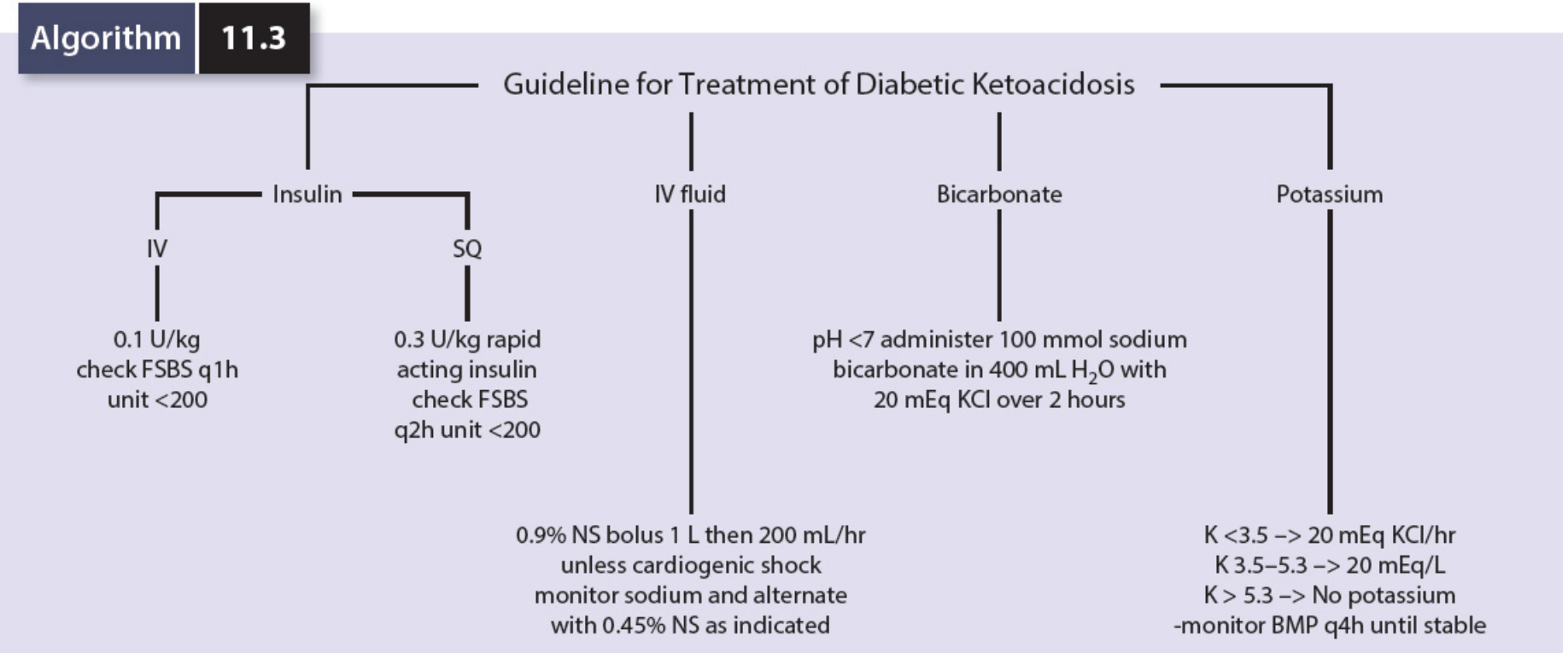
Algorithm 11.3 - Mulholland and Greenfield's Surgery
1. Initial Workup
Before starting treatment, confirm the diagnosis and identify the precipitant:
- Serum glucose, electrolytes, ketones, arterial blood gas
- CBC with differential, urinalysis, chest X-ray, ECG
- Beta-hydroxybutyrate levels (more reliable than urine ketones)
- Look for precipitants: infection, missed insulin, MI, pancreatitis, new-onset T1DM
Diagnostic criteria:
- Blood glucose >250 mg/dL
- pH <7.3
- Serum bicarbonate <18 mEq/L
- Anion gap >10-12
- Ketonemia/ketonuria
2. IV Fluids
The first priority is restoring circulating volume and then replacing total-body water deficit (usually 7-9% of body weight).
| Phase | Fluid | Rate |
|---|---|---|
| Immediate bolus | 0.9% NS | 1 L (children: 20 mL/kg) over 1-3 hours |
| Volume repletion | 0.9% NS | 500-1000 mL/h (if cardiac and renal function normal) |
| After initial repletion | 0.45% NS (or 0.9% NS if hyponatremic) | 150-500 mL/h |
| When glucose ≤300 mg/dL | Switch to D5W/0.45% NS | Continue until ketoacidosis resolves |
- Adjust rate based on BP and urine output
- Avoid correcting osmolality faster than 3 mOsm/kg/h
- Aim for positive fluid balance over 12-24 hours
- Serum sodium should rise as hyperglycemia corrects - if it doesn't, suspect overhydration
3. Insulin
Do NOT start insulin if K+ < 3.3-3.5 mEq/L - correct potassium first.
- Bolus: 0.1 units/kg IV regular insulin
- Infusion: 0.1 units/kg/h IV (regular insulin 100 units in 100 mL 0.9% NS at 10 mL/h = 10 units/h)
- Target glucose fall: 50-75 mg/dL/h (do not exceed 100 mg/dL/h - risk of osmotic encephalopathy)
When glucose reaches <250 mg/dL:
- Add dextrose (D5W) to prevent hypoglycemia while continuing insulin
- Consider the "two-bag approach" - separate dextrose infusion + reduced insulin at 0.05 units/kg/h (allows independent titration; shown to shorten treatment duration)
- Subcutaneous (SQ) approach for mild-moderate DKA: 0.3 units/kg rapid-acting insulin SQ, check glucose q2h
Stopping the insulin drip:
- Continue infusion until HCO3- >15 mEq/L, anion gap closed, and clinical improvement
- Give SC basal insulin 2 hours before stopping the IV infusion to prevent rebound ketosis
4. Potassium
DKA causes total-body potassium depletion (3-10 mEq/kg), even if serum K+ appears normal or high at presentation (due to transcellular shifts from insulin deficiency and acidosis). Insulin drives K+ into cells, causing serum K+ to fall during treatment.
| Serum K+ | Action |
|---|---|
| < 3.3-3.5 mEq/L | Replace K+ BEFORE starting insulin; 20 mEq KCl/hr |
| 3.5-5.3 mEq/L | Add 20-40 mEq KCl to each liter of IV fluid |
| > 5.3 mEq/L | No potassium yet; monitor BMP every 4 hours until stable |
- Check ECG for hyper/hypokalemia changes
- Potassium phosphate (KPhos) is preferred if co-existing hypophosphatemia
5. Bicarbonate
Not routinely recommended. Administer only in selected situations:
- pH <6.9, or HCO3- <5 mEq/L
- Shock or coma
- Severe cardiac or respiratory dysfunction
- Severe hyperkalemia
Dose: 50-100 mEq NaHCO3 in 1 L 0.45% NS over 30-60 min. Always add 10 mEq KCl to avoid hypokalemia. Follow arterial pH.
6. Phosphate & Magnesium
- Phosphate: Not routinely replaced, but potassium phosphate (KPhos) IV may be given in non-eating patients or if hypophosphatemia is significant
- Magnesium: 10-20 mEq MgSO4 IV if ventricular arrhythmias or documented deficiency
7. Monitoring
| Parameter | Frequency |
|---|---|
| Blood glucose | Every hour |
| Electrolytes, HCO3-, anion gap | Every 2-4 hours |
| Arterial blood gas | As needed (more frequently if severely acidotic) |
| Vital signs + urine output | Continuous |
| Fluid balance | Running total |
| Beta-hydroxybutyrate | Serial measurements helpful |
Telemetry is recommended given electrolyte instability.
8. Treat the Precipitant
Always search for and correct the underlying cause:
- Infections (most common) - start IV antibiotics promptly for documented/suspected infections; DKA itself causes leukocytosis, so fever is a meaningful sign
- Missed insulin doses
- New-onset Type 1 DM
- Myocardial infarction, stroke
- Drugs (steroids, SGLT2 inhibitors - euglycemic DKA)
- Pancreatitis (use lipase, not amylase, for diagnosis - amylase can be elevated in DKA)
9. Resolution Criteria (to stop insulin drip)
- Serum HCO3- >15 mEq/L (most reliable index of metabolic recovery)
- Anion gap closed (note: hyperchloremia from NS may close gap before true resolution - rely on HCO3-)
- Blood glucose <200-250 mg/dL
- Clinical improvement
10. Admit / Disposition
- ICU preferred for moderate-severe DKA
- Telemetry unit acceptable for stable patients
- Outpatient treatment may be considered in children only if: initial pH ≥7.35, HCO3- ≥20 mEq/L, tolerating oral fluids, symptoms resolved, reliable caregiver, no underlying precipitant
Recent Guideline Update (2024)
A 2024 consensus report on hyperglycemic crises (reviewed in Cleveland Clinic J Med 2025) has updated management recommendations, including guidance on SGLT2 inhibitor-associated euglycemic DKA. This should be considered when patients present with DKA but relatively normal glucose levels.
Sources:
- The Washington Manual of Medical Therapeutics, pp. 890-891
- Rosen's Emergency Medicine, Box 115.1
- Mulholland and Greenfield's Surgery, Algorithm 11.3
- Goldman-Cecil Medicine
Treatment for boils
Finding Sources
Searching PubMed
"furuncle" OR "boil" AND "skin abscess" AND treatment
Finding Sources
Searching PubMed
"skin abscess"[MeSH Terms] AND "incision and drainage"
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
I now have all the information needed for a comprehensive answer.
Treatment of Boils (Furuncles and Carbuncles)
Definitions
- Furuncle (boil): A deep abscess of a hair follicle, most commonly caused by Staphylococcus aureus (increasingly CA-MRSA). Presents as a painful, warm, erythematous, often fluctuant nodule. Common sites: axilla, inframammary region, buttocks, inner thigh.
- Carbuncle: A coalescence of multiple furuncles with loculations and connecting sinuses, often with multiple drainage points. Typically occurs on the back of the neck. More common in diabetics and middle-aged men.
Step 1: Confirm It Is a Boil, Not Cellulitis
Distinguishing an abscess from cellulitis is important because treatment differs:
- Boil/abscess: Fluctuant mass, hypoechoic on ultrasound with posterior acoustic enhancement
- Cellulitis: No central fluctuance, "cobblestoning" on ultrasound (interstitial edema)
- Bedside ultrasound with a high-frequency linear probe is the best tool when diagnosis is uncertain
Step 2: Primary Treatment - Incision and Drainage (I&D)
I&D is the first-line and definitive treatment for any fluctuant boil.
Needle aspiration alone is NOT adequate - blunt dissection is needed to disrupt loculations.
I&D Procedure:
- Attain adequate analgesia - local ring block with bupivacaine (25-gauge needle, allow 20 min), or procedural sedation. Adjuncts: ibuprofen + acetaminophen ± oxycodone ± low-dose diazepam
- Prep skin with povidone-iodine (nonsterile procedure)
- Incision - single incision along cutaneous tension lines (leaves smaller scar)
- Blunt dissection - use small clamp to probe cavity and disrupt loculations
- Irrigation - optional but may further break loculations
- Packing - traditional practice; packing is typically removed by the patient at home after 2-4 days. Evidence supporting packing is limited; loop drainage is a less painful alternative
Small, non-fluctuant furuncles: May resolve with warm compresses alone - no immediate I&D needed.
Step 3: Antibiotics
Antibiotics are not routinely required after I&D of an uncomplicated boil. A majority of patients (70-90%) achieve clinical cure with I&D alone.
When to add antibiotics:
| Indication | Action |
|---|---|
| Surrounding cellulitis or lymphadenitis | Antibiotics indicated |
| Systemic illness (fever, tachycardia) | Antibiotics indicated |
| Multiple sites of infection | Antibiotics indicated |
| Immunosuppression or significant comorbidities | Antibiotics indicated |
| Location difficult to drain (face, hand, genitalia) | Antibiotics indicated |
| Extremes of age | Antibiotics indicated |
| Septic phlebitis | Antibiotics indicated |
| Poor response to I&D alone | Add/change antibiotics |
| Furuncle not yet fluctuant | Consider antibiotics |
| Furuncle on the face | Consider antibiotics |
Antibiotic choices (oral):
| Drug | Adult Dose | Coverage | Notes |
|---|---|---|---|
| TMP-SMX (Trimethoprim-sulfamethoxazole) | 160 mg TMP BD | MSSA + MRSA | First choice for CA-MRSA; avoid in G6PD deficiency |
| Doxycycline | 100 mg BD | MSSA + MRSA | Empty stomach; sun sensitivity; ≥8 yrs only |
| Clindamycin | 300-450 mg TDS | MSSA + Strep ± MRSA | Variable MRSA coverage (check local sensitivity) |
| Cephalexin | 500 mg QID | MSSA + Strep | No MRSA coverage |
| Dicloxacillin | 250-500 mg QID | MSSA | Take on empty stomach; no MRSA coverage |
| Amoxicillin-clavulanate | 875 mg BD | MSSA + Strep + anaerobes | No MRSA coverage |
Key point: CA-MRSA now accounts for the majority of skin abscesses in the US. TMP-SMX or doxycycline should be favored when MRSA is a concern.
Step 4: Special Situations
Carbuncles:
- Have multiple interconnecting sinuses and tend to recur despite drainage and antibiotics
- Surgical drainage and resection of the lesion are often necessary
- Antibiotic cover required more often than for simple furuncles
Recurrent furuncles:
- Send wound cultures at time of I&D
- Screen for nasal carriage of S. aureus - decolonization with intranasal mupirocin + chlorhexidine body wash is recommended
- Screen for diabetes, HIV, or other immunodeficiency
Facial boils:
- Do NOT attempt home squeezing or self-drainage - risk of cavernous sinus thrombosis via facial veins
- Antibiotic therapy should be added
Diabetic patients:
- Higher risk of carbuncle formation and complications
- Lower threshold for antibiotic use and specialist referral
Pilonidal abscess:
- Treat acutely as a standard cutaneous abscess (I&D)
- Refer for surgical excision of the underlying cyst in recurrent cases
Step 5: Monitoring and Follow-Up
- Discharge after I&D of an uncomplicated boil is appropriate
- Patient removes packing at home after 2-4 days
- Return if: persistent or worsening pain, spreading redness, fever, or failure to improve
- Wound culture: Not routinely needed for uncomplicated first-episode boils, but indicated for recurrent infections, treatment failure, or when dual antibiotic coverage is being considered
When to Admit
Consider hospital admission for:
- Systemic sepsis
- Rapidly spreading infection or necrotizing fasciitis features (severe pain out of proportion, skin discoloration, crepitus)
- Immunocompromised patient with severe infection
- Failed outpatient I&D + antibiotics
Sources:
- Rosen's Emergency Medicine, Ch. 126
- Textbook of Family Medicine, 9e, p. 937
- Miller's Review of Orthopaedics, 9e, Table 1.28
- Sherris & Ryan's Medical Microbiology, 8e
Doxycycline duration
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
I have good data from the library. Let me compile a comprehensive, well-organized answer from all the sources gathered.
Doxycycline - Duration by Indication
Doxycycline is a broad-spectrum tetracycline antibiotic used across many infectious and non-infectious conditions. The treatment duration varies enormously depending on the indication. The standard adult dose is 100 mg twice daily (BD) unless otherwise noted.
Infections - Short Course (1-14 days)
| Condition | Dose | Duration | Notes |
|---|---|---|---|
| Chlamydia trachomatis (urethritis/cervicitis) | 100 mg BD | 7 days | CDC recommended |
| Chlamydial epididymitis | 100 mg BD | 10 days | With ceftriaxone 500 mg IM once |
| Pelvic inflammatory disease (PID) | 100 mg BD | 14 days | Usually combined with ceftriaxone |
| Sexually transmitted proctitis | 100 mg BD | 7 days | With ceftriaxone 500 mg IM once |
| Community-acquired pneumonia | 100 mg BD | 5-7 days | Atypical organisms, Mycoplasma |
| Chlamydia pneumoniae | 100 mg BD | 10-14 days | |
| Psittacosis (Chlamydophila psittaci) | 100 mg BD | 7-10 days | Azithromycin is alternative |
| Q fever (acute) | 100 mg BD | 14 days | Coxiella burnetii; quinolones also effective |
| Rocky Mountain Spotted Fever (RMSF) | 100 mg BD | 5-14 days | Continue until afebrile 3 days; doxycycline is drug of choice including in children |
| Rickettsial infections (general) | 100 mg BD | 5-14 days | Defervescence usually within 1-2 days |
| Skin/soft tissue infections (MRSA) | 100 mg BD | 5-7 days | After I&D of abscess |
| Leptospirosis | 100 mg BD | 7 days | Also used for prophylaxis (single 200 mg dose) |
| Plague (post-exposure prophylaxis) | 100 mg BD | 7 days | Treatment course is 10-14 days |
| Anthrax (post-exposure prophylaxis) | 100 mg BD | 60 days | Or ciprofloxacin; long course due to spore germination risk |
Infections - Intermediate Course (2-6 weeks)
| Condition | Dose | Duration | Notes |
|---|---|---|---|
| Lyme disease (erythema migrans) | 100 mg BD | 10-14 days | Some guidelines use up to 21 days |
| Lyme disease (early disseminated) | 100 mg BD | 14-21 days | Longer if CNS/cardiac involvement |
| Brucellosis | 100 mg BD | 6 weeks | Combined with rifampin or streptomycin |
| Trench fever (Bartonella quintana, bacteremic) | 200 mg/day PO | 28 days | Combined with gentamicin IV 14 days |
| Tularemia (less severe) | 100 mg BD | 14-21 days | Ciprofloxacin is an alternative |
| Q fever (chronic / pregnancy) | TMP-SMX preferred in pregnancy | Duration of pregnancy | Doxycycline avoided in pregnancy |
| Granuloma inguinale / Donovanosis | 100 mg BD | ≥3 weeks | Until lesions heal completely |
Chronic / Long-term Use
| Condition | Dose | Duration | Notes |
|---|---|---|---|
| Acne vulgaris | 50-100 mg BD | 3-6 months | Systemic tetracyclines; used for moderate-severe or topical-resistant acne |
| Rosacea | 40 mg once daily (subantimicrobial) or 100 mg BD | Months to years | Low-dose (40 mg) minimizes antibiotic resistance; isotretinoin for resistant cases |
| Malaria prophylaxis | 100 mg once daily | Start 1-2 days before travel, continue 4 weeks after departure | Effective against all Plasmodium species including chloroquine-resistant strains |
| Scrub typhus / Melioidosis (prophylaxis in hyperendemic areas) | 100 mg BD | Situational |
Key Pharmacology Points Relevant to Duration
- Long half-life (~18-22 hours): Once or twice-daily dosing is sufficient; better compliance than older tetracyclines
- Photosensitivity: Risk increases with prolonged use - patients should use sun protection
- Food interactions: Can be taken with food (unlike tetracycline HCl), which improves GI tolerance during long courses
- Esophageal ulceration: Take with full glass of water and remain upright for 30 min - important in long-term users
- Children <8 years: Generally avoided due to dental staining/bone effects - except in life-threatening rickettsial disease (RMSF) where it is still the drug of choice
- Pregnancy: Avoid after 1st trimester (teratogenic, dental discoloration)
- Resistance risk: Long courses (e.g., for acne) increase risk of resistance development; subantimicrobial dosing (40 mg) for rosacea avoids this
Summary Quick Reference
| Duration | Indications |
|---|---|
| 7 days | Chlamydia, STI proctitis, leptospirosis treatment |
| 10-14 days | Chlamydia pneumoniae, leptospirosis, early Lyme disease, psittacosis, plague treatment |
| 14 days | Acute Q fever, PID, RMSF (min) |
| 14-21 days | Tularemia, Lyme (disseminated) |
| 28-42 days | Trench fever (bacteremic), brucellosis |
| 60 days | Anthrax post-exposure prophylaxis |
| 3-6 months | Acne vulgaris |
| Ongoing | Malaria prophylaxis (while at risk + 4 wks after), rosacea maintenance |
Sources:
- Goldman-Cecil Medicine, Chapters on STIs, Parasitic Diseases, and Zoonoses
- Harrison's Principles of Internal Medicine, 22e (2025)
- Goodman & Gilman's Pharmacological Basis of Therapeutics
- Fitzpatrick's Dermatology
- Red Book 2021 - Report of the Committee on Infectious Diseases
For boils
Based on the previous conversation, this is asking specifically about doxycycline duration for boils (furuncles/skin abscesses).
From the textbook content already retrieved in this session:
Doxycycline Duration for Boils (Furuncles/Skin Abscesses)
Standard Duration: 5-7 days
- Dose: Doxycycline 100 mg orally, twice daily (BD)
- Duration: 5-7 days after incision and drainage (I&D)
Important Points
Antibiotics are not always needed. The primary treatment for a boil is I&D. Doxycycline (or TMP-SMX) is added only when:
- Surrounding cellulitis is present
- Systemic signs (fever, tachycardia)
- MRSA is suspected or confirmed
- Multiple sites of infection
- Immunocompromised patient
- Facial or genital boil
- Poor response to I&D alone
Why doxycycline specifically? Doxycycline covers both MSSA and CA-MRSA, making it a good empiric choice when MRSA is a concern. TMP-SMX (co-trimoxazole) is the alternative with similar MRSA coverage.
| Drug | MSSA | MRSA | Strep | Duration |
|---|---|---|---|---|
| Doxycycline | ✓ | ✓ | ± | 5-7 days |
| TMP-SMX | ✓ | ✓ | ✗ | 5-7 days |
| Clindamycin | ✓ | ± | ✓ | 5-7 days |
| Cephalexin | ✓ | ✗ | ✓ | 5-7 days |
Note: For patients ≥8 years only - avoid doxycycline in children under 8 and in pregnancy.
- Rosen's Emergency Medicine, Table 126.2
This is a shared conversation. Sign in to Orris to start your own chat.