Anemia profile
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the material needed for a comprehensive anemia profile. Let me compile the full response.
Anemia - Complete Profile
Definition
Anemia is defined as a reduction in blood hemoglobin concentration (or hematocrit) below the normal range for a given age, sex, and physiologic state. Practically, this means Hb < 13.5 g/dL in adult males and < 12 g/dL in adult females.
Classification
1. By MCV (Morphologic / Wintrobe Classification)
| Type | MCV | Key Causes |
|---|---|---|
| Microcytic | < 80 fL | Iron deficiency, Thalassemia, Anemia of chronic disease (ACD), Sideroblastic anemia |
| Normocytic | 80-100 fL | Aplastic anemia, Renal disease, Endocrinopathies, Myeloma, Marrow invasion, Pure red cell aplasia |
| Macrocytic | > 100 fL | Oval macrocytes: B12 deficiency, Folate deficiency, Chemotherapy, Myelodysplasia; Round macrocytes: Alcohol, Liver disease, Hypothyroidism, Reticulocytosis, Dysproteinemia |
2. By Mechanism (Pathophysiologic Classification)
| Mechanism | Examples |
|---|---|
| Blood loss | Acute trauma; chronic GI/gynecological bleeding |
| Hemolysis (increased destruction) | Hereditary spherocytosis, G6PD deficiency, Sickle cell, Thalassemia, AIHA, PNH, TTP/HUS |
| Decreased production | Iron/B12/folate deficiency, aplastic anemia, ACD, EPO deficiency, marrow infiltration |
3. By Reticulocyte Count (Functional)
- Hyperproliferative (reticulocytes ↑): Hemolysis or blood loss - the marrow is responding normally
- Hypoproliferative (reticulocytes ↓ or normal): Defective production - marrow failure, nutritional deficiency, or chronic disease
Major Anemia Types - Detailed
A. Iron Deficiency Anemia (IDA)
Most common anemia worldwide.
Causes:
- Dietary lack (infants, vegans, elderly, impoverished)
- Impaired absorption (sprue, gastrectomy, celiac)
- Increased requirement (pregnancy, infancy, adolescence)
- Chronic blood loss - most common cause in developed countries (GI lesions, gynecologic bleeding)
Iron deficiency in adult males or postmenopausal females must be attributed to GI blood loss until proven otherwise - to prematurely ascribe another cause risks missing a GI cancer.
Iron Metabolism:
- Normal daily requirement: ~1 mg absorbed; dietary intake 10-20 mg/day (only 10-15% absorbed)
- Heme iron (from meat) is ~20% absorbable vs 1-2% for non-heme iron
- Storage iron: Ferritin (main storage, correlates with body stores) and Hemosiderin (aggregated ferritin, Prussian blue positive)
- Absorption enhanced by: ascorbic acid, citric acid, amino acids
- Absorption inhibited by: tannins (tea), carbonates, oxalates, phosphates
Stages of Iron Deficiency:
- Pre-latent: Iron stores deplete; serum ferritin falls; no anemia yet
- Latent: Serum iron falls, TIBC rises, transferrin saturation falls below 15%; no anemia
- Overt IDA: Hemoglobin falls; microcytic hypochromic anemia appears
Lab Findings in IDA:
| Parameter | Finding |
|---|---|
| Hb / Hct | Decreased |
| MCV | Low (microcytic) |
| MCH / MCHC | Low (hypochromic) |
| Serum iron | ↓ |
| TIBC (Transferrin) | ↑ |
| Transferrin saturation | < 15% |
| Serum ferritin | ↓ (< 12 µg/L) |
| Serum hepcidin | ↓ (reduced iron inhibits hepcidin synthesis) |
| Reticulocytes | Low initially, rise after treatment |
Peripheral Blood Smear - IDA:

Hypochromic microcytic RBCs - the zone of central pallor is greatly enlarged. "Pencil cells" (elongated poikilocytes) are characteristic. Fully hemoglobinized cells visible from a recent transfusion.
Clinical Features:
- General anemia symptoms: fatigue, pallor, dyspnea on exertion
- Koilonychia (spoon nails), alopecia
- Atrophic glossitis, angular cheilitis
- Pica (craving for clay, ice [pagophagia], flour)
- Plummer-Vinson syndrome (triad): microcytic anemia + esophageal web + atrophic glossitis
- Central nervous system: pica, restless leg syndrome
Treatment: Oral iron supplementation - reticulocytosis appears in 5-7 days, Hb normalizes in 6-8 weeks; continued for 3+ months to replete stores.
B. Megaloblastic Anemia (B12 / Folate Deficiency)
Pathogenesis: Impaired DNA synthesis (thymidine synthesis requires B12 and folate as cofactors) → nuclear maturation delay while cytoplasmic maturation continues → nuclear-cytoplasmic asynchrony → ineffective hematopoiesis + pancytopenia.
Causes of Megaloblastic Anemia:
| B12 Deficiency | Folate Deficiency | Other |
|---|---|---|
| Inadequate diet (strict vegetarians) | Inadequate diet, alcoholism, infancy | Methotrexate, hydroxyurea |
| Pernicious anemia (autoimmune - anti-IF antibodies) | Malabsorption (celiac, sprue) | 5-FU, other chemotherapy |
| Gastrectomy | Anticonvulsants, oral contraceptives | Myelodysplasia |
| Ileal resection / Crohn's disease | Increased requirements (pregnancy, hemolysis, cancer) | |
| Bacterial overgrowth / Fish tapeworm | Hemodialysis (increased loss) |
Lab Findings:
| Parameter | Finding |
|---|---|
| MCV | ↑ (macrocytic, often > 110 fL) |
| Peripheral smear | Macro-ovalocytes, hypersegmented neutrophils (≥5 lobes) |
| WBC / Platelets | ↓ (pancytopenia from ineffective hematopoiesis) |
| LDH | ↑↑ (from ineffective hematopoiesis / intramedullary cell death) |
| Indirect bilirubin | ↑ (mild hemolysis) |
| Reticulocytes | Low (despite hypercellular marrow) |
| Serum B12 | ↓ in B12 deficiency |
| Serum folate / RBC folate | ↓ in folate deficiency |
| Methylmalonic acid (MMA) | ↑ in B12 deficiency only (not in folate deficiency) |
| Homocysteine | ↑ in both B12 and folate deficiency |
Key Peripheral Smear Finding - Megaloblastic Anemia:
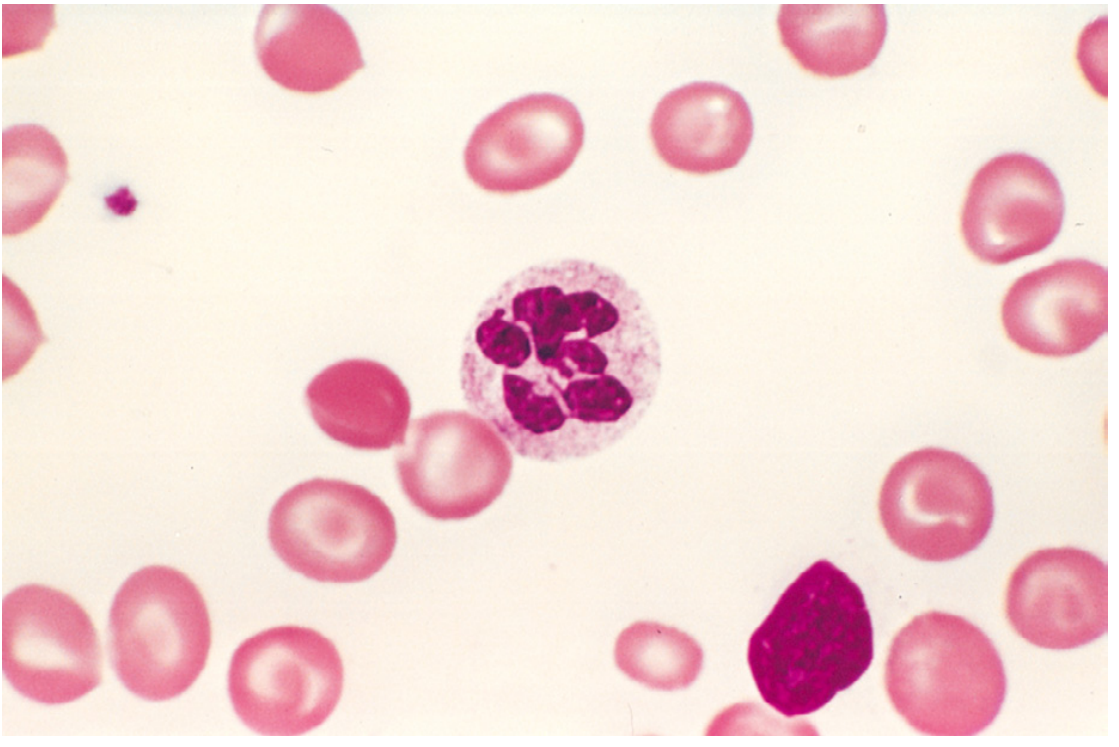
Hypersegmented neutrophil (≥5 nuclear lobes) - a hallmark of megaloblastic anemia. Macro-ovalocytes are also seen in the background.
B12 vs Folate Deficiency - Key Distinctions:
| Feature | B12 Deficiency | Folate Deficiency |
|---|---|---|
| Neurological signs | Yes - subacute combined degeneration (posterior + lateral columns) | No neurological signs |
| MMA | ↑ | Normal |
| Homocysteine | ↑ | ↑ |
| Onset | Slow (years - large hepatic stores) | Faster (weeks to months - small stores) |
Pernicious Anemia (PA):
- Autoimmune atrophic gastritis → loss of parietal cells → intrinsic factor (IF) deficiency → B12 malabsorption
- Antibodies: Anti-parietal cell antibodies (~90%); Anti-intrinsic factor antibodies (more specific, ~60%)
- Associated with other autoimmune diseases (thyroiditis, Addison's, vitiligo)
- Treatment: IM/SC hydroxocobalamin or cyanocobalamin (bypasses gut absorption defect)
C. Anemia of Chronic Disease (ACD) / Anemia of Inflammation
Pathogenesis: Inflammation → IL-6 → ↑ hepatic hepcidin → hepcidin blocks ferroportin on macrophages → iron sequestered in storage pool → iron-starved erythroid precursors (functional iron deficiency despite adequate total body iron).
Associated Conditions:
- Chronic infections (osteomyelitis, TB, bacterial endocarditis, lung abscess)
- Chronic immune disorders (rheumatoid arthritis, IBD, SLE)
- Neoplasms (Hodgkin lymphoma, lung and breast carcinomas)
Lab Findings:
| Parameter | ACD | IDA |
|---|---|---|
| Serum iron | ↓ | ↓ |
| TIBC | ↓ (or normal) | ↑ |
| Serum ferritin | ↑ (or normal) | ↓ |
| Storage iron (Prussian blue) | ↑ in marrow macrophages | Absent |
| Hepcidin | ↑ | ↓ |
| Morphology | Normocytic normochromic (may be mildly microcytic) | Microcytic hypochromic |
Treatment: Treat underlying disease; erythropoietin-stimulating agents in cancer patients.
D. Hemolytic Anemias
Two major categories of hemolysis:
Extravascular Hemolysis (Spleen/macrophage mediated)
- RBCs destroyed by splenic macrophages
- Findings: Splenomegaly, jaundice (↑ unconjugated bilirubin), pigment gallstones (chronic)
- Iron is efficiently recycled - NO iron deficiency
Intravascular Hemolysis (RBCs lyse within vessels)
- RBCs burst in circulation
- Findings: Hemoglobinemia, hemoglobinuria (pink/red urine), hemosiderinuria, ↓ haptoglobin, ↓ iron stores (iron lost in urine)
- Haptoglobin is ↓ in BOTH types
General hemolytic anemia findings:
- ↑ Reticulocytes (regenerative response)
- ↑ LDH, ↑ indirect bilirubin
- ↓ Haptoglobin
- Marrow erythroid hyperplasia
- Possible extramedullary hematopoiesis (liver, spleen, lymph nodes) in severe cases
Common subtypes:
| Anemia | Defect | Key Feature |
|---|---|---|
| Hereditary spherocytosis | Spectrin/ankyrin mutations → membrane defect | Spherocytes, osmotic fragility ↑, splenomegaly |
| G6PD deficiency | Hexose monophosphate shunt enzyme defect | Heinz bodies, bite cells; triggered by oxidant stress (primaquine, fava beans, infections) |
| Sickle cell disease | HbS (Glu→Val substitution) | Sickle cells, vaso-occlusive crises, autosplenectomy, HbS on electrophoresis |
| Thalassemia | Deficient α or β globin synthesis | Target cells, microcytosis; thalassemia major requires transfusions |
| Autoimmune hemolytic anemia | Warm (IgG) or Cold (IgM) antibodies against RBCs | Positive direct Coombs (DAT) test |
| TTP / HUS | Microangiopathic; thrombotic occlusion fragments RBCs | Schistocytes (helmet cells), thrombocytopenia |
| PNH | Acquired mutation (PIG-A) - loss of GPI-anchored proteins (CD55, CD59) | Complement-mediated hemolysis; thrombosis; flow cytometry diagnostic |
E. Aplastic Anemia
Definition: Chronic primary hematopoietic failure → pancytopenia (anemia + neutropenia + thrombocytopenia) from bone marrow hypoplasia.
Mechanism: Mostly autoimmune - T cells attack stem cells. Also: stem cell intrinsic defects.
Causes:
| Acquired | Inherited |
|---|---|
| Idiopathic (~70%) | Fanconi anemia (DNA repair defect; autosomal recessive) |
| Drugs: chloramphenicol, benzene, alkylating agents, gold salts, phenylbutazone | Telomerase defects (dyskeratosis congenita) |
| Viral infections (hepatitis B/C, CMV, EBV, parvovirus B19) | |
| Whole-body irradiation |
Lab: Pancytopenia + hypocellular bone marrow biopsy (marrow replaced by fat cells) + absent/reduced reticulocytes.
Treatment: Bone marrow transplant (young patients with matched donor) or immunosuppression (anti-thymocyte globulin + cyclosporine + eltrombopag).
Summary Comparison Table
| Feature | IDA | ACD | Megaloblastic | Hemolytic | Aplastic |
|---|---|---|---|---|---|
| MCV | ↓ | N or ↓ | ↑ | N or ↑ | N |
| Serum iron | ↓ | ↓ | N | N | N |
| TIBC | ↑ | ↓/N | N | N | N |
| Ferritin | ↓ | ↑/N | N | N | N |
| Reticulocytes | ↓ | ↓ | ↓ | ↑ | ↓ |
| Haptoglobin | N | N | N | ↓ | N |
| LDH | N | N | ↑↑ | ↑ | N |
| Bilirubin (indirect) | N | N | ↑ | ↑ | N |
| B12/Folate | N | N | ↓ | N | N |
| Bone marrow | Erythroid hyperplasia | Erythroid hyperplasia | Megaloblasts; hypercellular | Erythroid hyperplasia | Hypocellular (fat cells) |
Key Clinical Pearls
- Ferritin is an acute-phase reactant - it may be normal or elevated in ACD even with concurrent iron deficiency. Serum transferrin receptor (sTfR) or sTfR/log ferritin ratio helps distinguish IDA from ACD.
- Methylmalonic acid distinguishes B12 from folate deficiency - MMA is elevated only in B12 deficiency; homocysteine is elevated in both.
- Hypersegmented neutrophils (≥5 lobes, or any 6-lobed neutrophil) are the earliest and most sensitive sign of megaloblastic change.
- In hemolytic anemia, a low haptoglobin is the most sensitive single test; schistocytes on smear indicate microangiopathic process.
- Reticulocyte production index (RPI) < 2 = hypoproliferative (production problem); > 3 = hyperproliferative (loss/destruction problem).
- IDA in an adult male or postmenopausal female = GI bleeding until proven otherwise - always investigate for colorectal cancer.
Sources: Robbins, Cotran & Kumar - Pathologic Basis of Disease (9780443264528); Harrison's Principles of Internal Medicine 22E (9781265977061); Robbins & Kumar Basic Pathology (9780323790185)
This is a shared conversation. Sign in to Orris to start your own chat.