Acute ischemia of lower limbs
Reading File
Finding Sources
Finding Sources
Searching PubMed
"acute limb ischemia"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Searching Images
acute limb ischemia management algorithm revascularization
Finding Sources
Reading File
I now have comprehensive information to deliver a thorough, well-structured answer. Let me compile it.
Acute Ischemia of the Lower Limbs (ALI)
Acute limb ischemia (ALI) is defined as an arterial occlusion with associated ischemic symptoms present for less than 2 weeks, resulting in abrupt cessation or marked diminution of blood flow that threatens limb viability. It is a surgical emergency — irreversible muscle and nerve injury can occur within 6 hours of severe arterial insufficiency.
Epidemiology: ~1.5 cases per 10,000 persons/year. Perioperative mortality: 20–40%; limb loss: 12–50%. The 30-day amputation rate is 10–30%, with a 15% 1-year mortality.
Etiology
1. Embolism
The most common cardiac sources of arterial emboli:
- Atrial fibrillation (thrombus in atrial appendage)
- Acute myocardial infarction (mural thrombus)
- Ventricular aneurysm, cardiomyopathy
- Infective/marantic endocarditis
- Prosthetic heart valves
- Atrial myxoma
Non-cardiac embolic sources include atherosclerotic plaques and aneurysms of the aorta/large vessels. Paradoxical embolism (venous thrombus via patent foramen ovale) is less common.
Emboli lodge at vessel bifurcations due to reduced caliber. In the lower extremity, the order of frequency is:
Femoral artery > Iliac artery > Aorta > Popliteal/tibioperoneal arteries
2. In situ Thrombosis
Occurs most frequently in:
- Atherosclerotic vessels at the site of a plaque or aneurysm
- Arterial bypass grafts
- Native vessels with hypercoagulable states (polycythemia, thrombophilia)
- Thrombosed popliteal artery aneurysm (an important, often overlooked cause)
3. Other Causes
- Trauma: arterial disruption, intimal flap, catheter-related injury
- Aortic dissection: intimal flap obstructing flow
- Hemodynamic: shock, vasopressor use (low-flow states)
- Entrapment syndromes: popliteal artery entrapment by abnormal medial gastrocnemius head
- Thoracic outlet syndrome: subclavian artery occlusion
Clinical Features — The "Six Ps"
| Sign | Details |
|---|---|
| Pain | Sudden, severe; onset within 1 hour |
| Pulselessness | Absent distal to occlusion |
| Pallor | Pale, cold skin |
| Poikilothermia | Coolness; temperature gradient marks level of occlusion |
| Paresthesia | Numbness, tingling — indicates nerve ischemia |
| Paralysis | Late sign; indicates severe, prolonged ischemia |
The temperature border (transition from cool to warm) localizes the occlusion level. Continuous-wave Doppler assessment (multiphasic vs. monophasic vs. absent) helps quantify degree of insufficiency.
Rutherford Classification (Grading Severity)
| Category | Description | Sensory Loss | Muscle Weakness | Arterial Doppler | Venous Doppler |
|---|---|---|---|---|---|
| I — Viable | Not immediately threatened | None | None | Audible | Audible |
| IIa — Marginally threatened | Salvageable if promptly treated | Minimal (toes)/none | None | Absent | Audible |
| IIb — Immediately threatened | Requires immediate revascularization | More than toes + rest pain | Mild–moderate | Absent | Audible |
| III — Irreversible | Major tissue loss/permanent nerve damage | Profound, anesthetic | Profound paralysis (rigor) | Absent | Absent |
Modified from Rutherford et al., J Vasc Surg 1997.
Diagnosis
- Clinical assessment is the most important step, defining cause, severity, and management strategy
- Continuous-wave Doppler: rapid bedside assessment
- CTA (CT angiography): often the fastest tool to guide operative approach (endovascular, open, or hybrid)
- Duplex ultrasound: identifies popliteal aneurysm thrombosis, graft occlusion
- MRA / Catheter-based arteriography: for detailed anatomical mapping when time allows
- Echocardiography: to identify embolic cardiac sources
- Workup for thrombophilia: if no obvious cause (hypercoagulable panel)
Embolism vs. Thrombosis: Key Distinguishing Features
| Feature | Embolism | Thrombosis |
|---|---|---|
| Onset | Sudden, severe | May be less acute (pre-existing collaterals) |
| Prior claudication | Absent | Often present |
| Contralateral pulses | Present | May be absent (bilateral PAD) |
| Cardiac disease (AF, MI) | Common | Less common |
| Doppler signals contralateral | Normal | Often abnormal |
Management
Step 1: Immediate Anticoagulation
IV unfractionated heparin immediately upon diagnosis → prevents clot propagation and recurrent embolism. Prefer agents that allow titration and rapid reversal.
Step 2: Stratify by Rutherford Class
Category III (Irreversible): Primary amputation — revascularization of a non-viable extremity risks multisystem organ failure and death. Rigor of muscles is a key sign of irreversibility.
Category I & II (Viable/Threatened): Proceed to revascularization:
Endovascular Options
- Catheter-directed thrombolysis (CDT): rtPA, reteplase, or tenecteplase. Best when:
- Recent arterial occlusion from thrombus in atherosclerotic vessel, bypass graft, or occluded stent
- Patient is high-risk for surgery
- Small distal vessels occluded (inaccessible surgically)
- Requires meticulous monitoring for hemorrhagic complications
- Ultrasound-assisted catheters (e.g., EKOS) may accelerate reperfusion
- Percutaneous mechanical thrombectomy: hydrodynamic or rotational devices; often combined with pharmacologic thrombolysis
Surgical Options (preferred when blood flow must be restored within 24 h)
- Fogarty balloon thromboembolectomy: standard for embolic occlusion — preferred in IIb where time for CDT would cause progression to irreversibility
- Arterial bypass (saphenous vein or prosthetic graft)
- Hybrid procedures: combination endovascular + open
Key principle: Surgical thromboembolectomy is preferred in Rutherford IIb (sensory/motor deficit, absent pedal signals) because catheter-based treatment takes too long — delay risks progression to irreversibility.
Step 3: Post-Revascularization
- Four-compartment fasciotomy of the lower extremity should always be considered after revascularization, especially if ischemia time >6 hours → prevents reperfusion-induced compartment syndrome
- Long-term anticoagulation: indicated when ALI is caused by cardiac thromboembolism (AF, prosthetic valve)
Complications
| Complication | Mechanism |
|---|---|
| Reperfusion injury | Ischemia–reperfusion → ROS, cytokine release, endothelial damage |
| Compartment syndrome | Muscle edema post-revascularization → fasciotomy indicated |
| Myoglobinuria/AKI | Rhabdomyolysis from ischemic muscle necrosis |
| Hyperkalemia | Release from necrotic cells |
| Multisystem organ failure | Systemic reperfusion syndrome |
| Recurrence | Especially in embolic etiology — address underlying source |
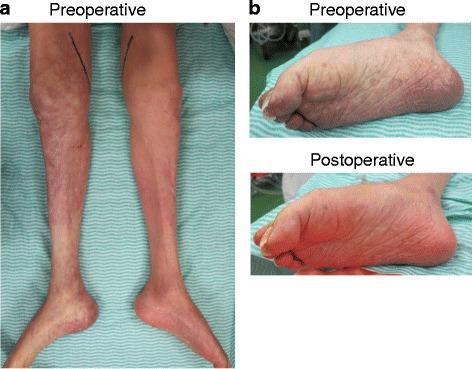
Clinical Images
Pre- and post-thromboembolectomy:
Advanced ischemia with fasciotomy and staged reconstruction:

Summary Algorithm
Suspected ALI
↓
IV Heparin immediately
↓
History + Exam + Doppler → Rutherford Class
↓
Class III (irreversible)? → Primary AMPUTATION
↓ No
Imaging: CTA / Arteriography (identify level & etiology)
↓
Embolism? Thrombosis?
↓ ↓
Fogarty CDT (if time allows)
Thromboembolectomy Mechanical thrombectomy
Surgical bypass
↓
Revascularization complete
↓
Fasciotomy if ischemia >6h
↓
Long-term anticoagulation if cardiac source
Sources:
- Sabiston Textbook of Surgery, 21st ed. (Rutherford Classification, surgical management)
- Harrison's Principles of Internal Medicine, 22nd ed. 2025 (etiology, treatment)
- Goldman-Cecil Medicine, International Edition (pathobiology, approach)
- Schwartz's Principles of Surgery, 11th ed.
This is a shared conversation. Sign in to Orris to start your own chat.