I now have everything I need to write a comprehensive, exam-oriented answer on peptic ulcer for MBBS 2nd year. Let me compile it.
Peptic Ulcer Disease - MBBS 2nd Year Exam Guide
Definition
A peptic ulcer is an excoriated (mucosal break extending through the muscularis mucosae) area of the stomach or intestinal mucosa caused principally by the digestive action of gastric acid (HCl) and pepsin. In the absence of acid, peptic ulcers do not occur.
- Guyton & Hall Textbook of Medical Physiology, p. 825
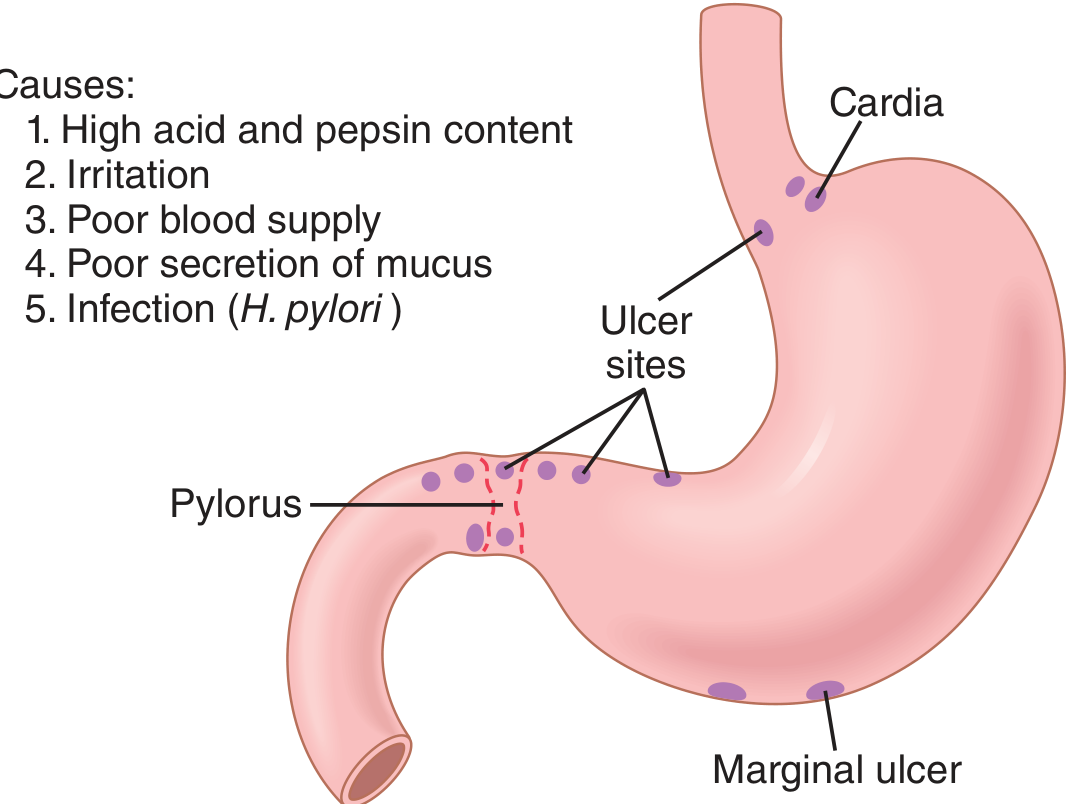
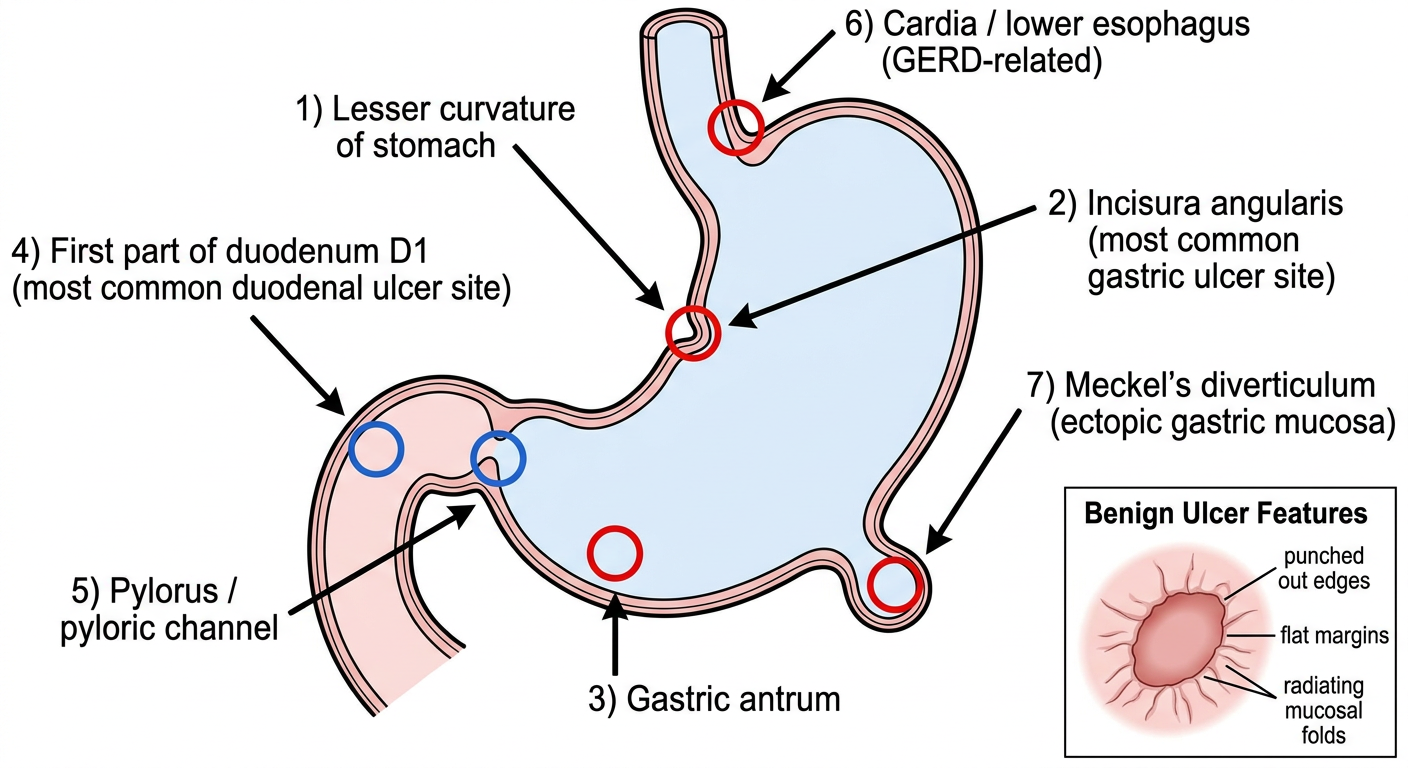
Sites (Common Locations)
Peptic ulcers occur wherever mucosa is exposed to acid-pepsin:
- Duodenum - First part (D1), most common overall
- Stomach - Lesser curvature (especially incisura angularis), antrum
- Lower esophagus - Due to acid reflux (GERD)
- Meckel's diverticulum - Contains ectopic gastric epithelium
- Stomal/marginal ulcer - At gastrojejunostomy site
The ulcer tends to occur at the junction between different epithelial types, in the mucosa least resistant to acid damage.
Epidemiology
- PUD affects >4 million people annually in the US
- Lifetime risk: ~10% in males, ~4% in females
- Duodenal ulcers are more common than gastric ulcers (DU:GU = ~4:1)
- Gastric ulcers: equal sex incidence, tend to occur in older patients and lower socioeconomic groups
Pathogenesis - The Key Concept
"Imbalance between mucosal protective factors and damaging factors"
Protective Factors
| Factor | Mechanism |
|---|
| Mucus layer | Forms gel barrier between lumen and epithelium |
| HCO3- secretion | Trapped in mucus; neutralizes any H+ that penetrates |
| Prostaglandin E2 | Stimulates mucus + HCO3- secretion; maintains mucosal blood flow |
| Mucosal blood flow | Delivers O2 and nutrients; removes back-diffused H+ |
| Epithelial tight junctions | Prevent luminal H+ from entering mucosa |
| Growth factors | Aid mucosal repair |
Damaging Factors
| Factor | Mechanism |
|---|
| H. pylori | Destroys mucosal barrier via urease (NH3), cytotoxins (CagA), phospholipases |
| NSAIDs/Aspirin | Inhibit COX → suppress prostaglandin synthesis → loss of mucosal protection |
| Excess HCl + Pepsin | Direct erosive action on unprotected mucosa |
| Smoking | Reduces mucosal blood flow; impairs healing |
| Alcohol | Breaks down mucosal barrier directly |
| Corticosteroids | Suppress prostaglandin synthesis; impair healing |
| Stress | Increases acid secretion via vagal stimulation |
Etiology
1. Helicobacter pylori (Most Important - 70-75% of PUD)
- Gram-negative, microaerophilic, spiral bacterium
- Urease splits urea → NH3, which neutralizes local acid, allows survival in gastric lumen
- NH3 and NH4+ are cytotoxic to epithelial cells
- Virulence factors: CagA toxin (breaks mucosal barrier), VacA (vacuolating cytotoxin)
- In gastric ulcer: directly colonizes antral mucosa, releases cytotoxins, destroys protective mucous barrier
- In duodenal ulcer (indirect mechanism):
- H. pylori in gastric antrum → inhibits somatostatin from D cells → somatostatin normally inhibits gastrin → "inhibition of inhibition" = excess gastrin secretion → excess HCl
- H. pylori spreads to duodenum → inhibits duodenal HCO3- secretion → inadequate neutralization of H+
- Only 5-10% of H. pylori-infected individuals develop ulcers (host factors + bacterial strain variation matter)
2. NSAIDs / Aspirin
- Inhibit COX-1 and COX-2 → reduced prostaglandin E2 synthesis
- Loss of mucosal protection (mucus, HCO3-, blood flow) → gastric ulcers more than duodenal
- Becoming the most common cause of gastric ulcers as H. pylori infection rates fall
3. Zollinger-Ellison Syndrome
- Gastrinoma (usually pancreatic islet cell tumor) secretes gastrin constitutively
- Massive, unregulated HCl secretion overwhelms all buffering
- Multiple peptic ulcers in stomach, duodenum, and even jejunum
- Gastrin is not feedback-inhibited by H+ (unlike physiologic G-cell secretion)
- Steatorrhea occurs because excessive H+ inactivates pancreatic lipase in the duodenum
4. Other Contributing Factors
- Hyperparathyroidism, CRF - hypercalcemia stimulates gastrin production
- Cirrhosis, COPD, CKD - associated with increased PUD risk
- Parietal cell hyperplasia - increased secretory capacity
Gastric Ulcer vs Duodenal Ulcer - High-Yield Comparison
| Feature | Gastric Ulcer | Duodenal Ulcer |
|---|
| Frequency | Less common | More common (4x) |
| Age | Older patients (50-60s) | Younger patients (30-50s) |
| Sex | Equal | More in males |
| Acid secretion | Normal or low (H+ leaks into damaged mucosa) | High (increased parietal cell mass) |
| Gastrin level | Increased (due to reduced H+ feedback) | Baseline normal; meal-stimulated increased |
| H. pylori role | Direct mucosal barrier destruction | Indirect via excess H+ delivery to duodenum |
| Pain and food | Eating may worsen (or no relief) | Eating relieves pain (food buffers H+) |
| Night pain | Less characteristic | Characteristic (2-3 am - awakens patient) |
| Malignancy risk | YES - must biopsy to exclude (up to 10x biopsies) | NO - duodenal ulcers almost never malignant |
| Site | Lesser curvature, incisura angularis, antrum | Anterior wall of D1 (most common) |
| Blood group | Group A | Group O |
- Costanzo Physiology 7th Edition, p. 370; Bailey & Love Surgery 28th Ed.
Morphology (Pathology - Robbins)
Gross:
- Usually solitary (multiple suggest Zollinger-Ellison)
- Round to oval, sharply "punched out" defect
- Size: Usually <2 cm (rarely >4 cm); size does NOT differentiate benign from malignant
- Margins: flat, overhanging edges (benign); rolled-up edges suggest malignancy
- Base: Clean, smooth (benign) vs irregular hemorrhagic (malignant)
- Surrounding mucosa shows mucosal folds radiating to the ulcer edge (benign)
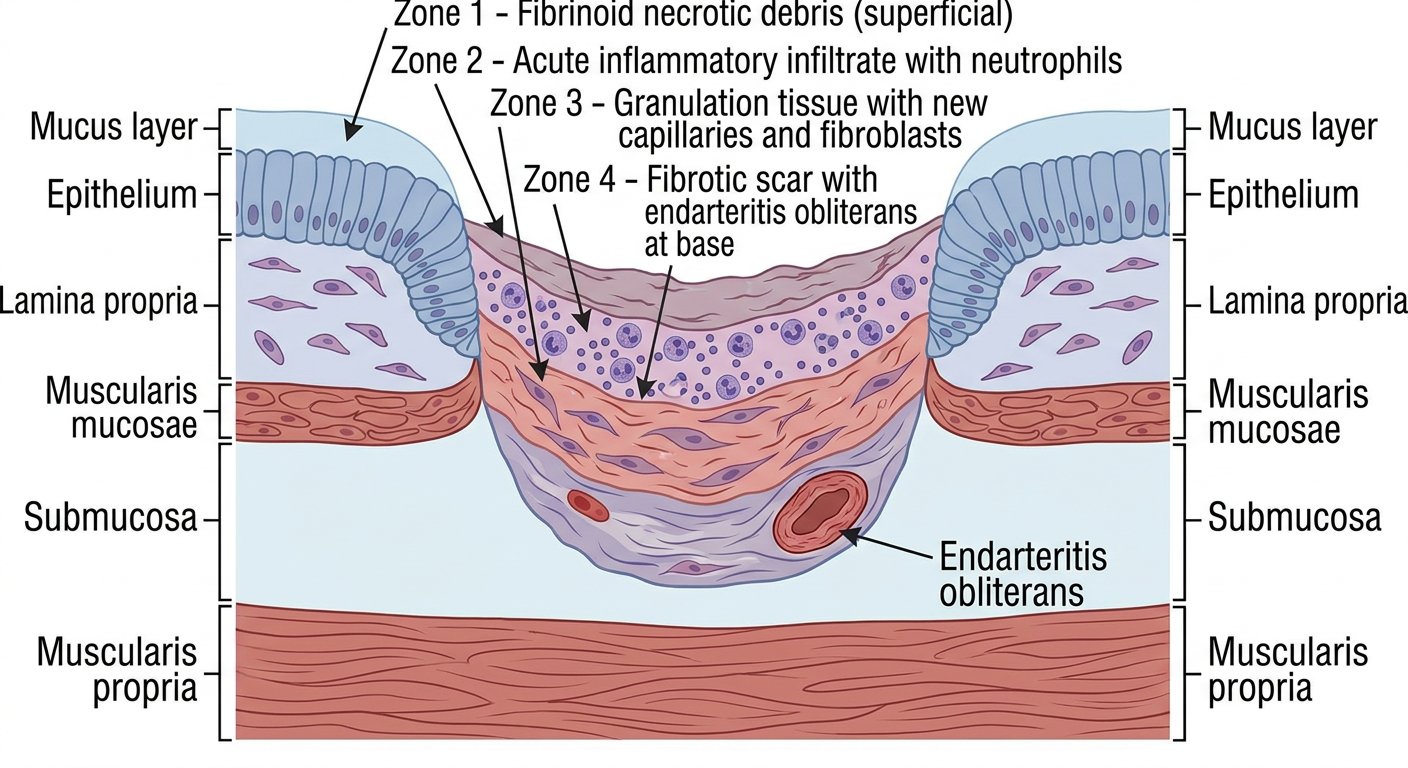
Microscopic:
- Zone of necrotic fibrinoid debris (superficial)
- Active inflammatory exudate (neutrophils)
- Granulation tissue with dilated capillaries and fibroblasts
- Fibrous/collagenous scar at the base - endarteritis obliterans (thickened vessel walls at the base)
Note: healing epithelium can mimic invasion - must not be mistaken for carcinoma
Clinical Features
Symptoms
- Epigastric pain - gnawing, burning, or aching
- May radiate to the back (especially if posterior penetration into pancreas)
- Periodicity - symptoms for weeks → remission for months → recurrence (due to spontaneous healing and relapse)
- Seasonality - worse in spring and autumn
- Vomiting - not prominent unless gastric outlet obstruction occurs
- Weight loss or gain possible; patients with gastric ulcers often underweight
Examination
- Epigastric tenderness is the main finding
- Otherwise examination may be unremarkable in uncomplicated PUD
Investigations
| Investigation | Findings |
|---|
| OGD (upper endoscopy) | Gold standard - directly visualizes ulcer; allows biopsy |
| Barium meal (Ba meal) | "Niche" = ulcer crater; gastric ulcer appears as barium pool projecting outside lumen |
| CLO test (Campylobacter-like organism) | Rapid urease test for H. pylori at endoscopy |
| Urea breath test (13C-UBT) | Patient drinks 13C-urea → H. pylori urease converts it → 13CO2 expired in breath; non-invasive |
| H. pylori serology | Detects IgG antibodies; cannot distinguish active from past infection |
| Stool antigen test | Active H. pylori infection |
| Serum gastrin | Elevated if Zollinger-Ellison syndrome suspected |
| Hemoglobin/FBC | Microcytic anemia if chronic blood loss |
Complications (Mnemonic: PBS-H)
1. Perforation
- Most commonly anterior DU perforates (duodenal ulcers more likely to perforate)
- Presents with: sudden severe epigastric pain → generalized peritonitis
- Board-like rigidity, shoulder tip pain (phrenic nerve irritation by subphrenic air)
- X-ray: Free air under diaphragm (pneumoperitoneum)
- Treatment: Emergency surgery (Graham's patch repair)
2. Bleeding (Most Common Complication)
- May be chronic (presenting as microcytic iron-deficiency anemia) or acute (hematemesis + melena)
- Posterior DU erodes into gastroduodenal artery (most dangerous)
- Treatment: Endoscopic hemostasis (adrenaline injection, clips, thermal coagulation), PPIs IV; surgery if endoscopy fails
3. Stenosis / Gastric Outlet Obstruction (GOO)
- Chronic DU → fibrosis and scarring → pyloric stenosis
- Features: projectile, non-bilious vomiting; visible peristalsis; succussion splash
- Metabolic consequence: Hypochloraemic, hypokalaemic metabolic alkalosis (from loss of HCl in vomit)
- Treatment: Endoscopic balloon dilatation; surgery (pyloroplasty)
4. Penetration
- Ulcer erodes through wall into adjacent structure without free perforation
- Posterior GU → pancreas (raised serum amylase)
- GU → splenic artery (rare but fatal hemorrhage)
- Change in pain character: becomes constant, no longer relieved by food/antacids
5. Malignant Transformation (Gastric Ulcers Only)
- Gastric ulcers can harbor carcinoma or undergo malignant change
- ALL gastric ulcers require biopsy (minimum 6-10 biopsies from margin and base)
- Duodenal ulcers do NOT become malignant
Treatment
Medical (Mainstay)
Step 1: Acid Suppression
| Drug | Class | Mechanism |
|---|
| Omeprazole, Pantoprazole, Rabeprazole | Proton Pump Inhibitors (PPIs) | Irreversibly block H+/K+ ATPase (proton pump) on parietal cells |
| Ranitidine, Famotidine | H2-receptor antagonists | Block histamine H2 receptors on parietal cells → 70-80% reduction in acid |
| Vonoprazan | Potassium-competitive acid blocker (PCAB) | Binds K+-binding region of proton pump; more rapid, sustained acid suppression |
Step 2: H. pylori Eradication
Standard Triple Therapy (7-14 days):
- PPI (twice daily) + Amoxicillin + Clarithromycin
Quadruple Therapy (if clarithromycin resistance):
- PPI + Bismuth + Metronidazole + Tetracycline
Confirm eradication with urea breath test 4 weeks after completing therapy.
Additional Measures
- Misoprostol (prostaglandin E1 analogue) - protects gastric mucosa; used for NSAID-induced ulcers
- Sucralfate - coats ulcer base; forms a protective barrier
- Antacids - neutralize HCl; symptomatic relief
- Lifestyle: Stop smoking, avoid NSAIDs and alcohol, stress reduction
Surgical (Rarely Indicated Now)
Performed only for complications (perforation, uncontrolled bleeding, obstruction) or refractory disease.
- Vagotomy (truncal or selective) - cuts vagal supply to parietal cells → reduces acid
- Partial gastrectomy (Billroth I or II) - removes ulcer-bearing mucosa
- Pyloroplasty - relieves GOO
Zollinger-Ellison Syndrome (ZES) - Special Topic
| Feature | Detail |
|---|
| Cause | Gastrinoma (most commonly in pancreatic head or duodenum) |
| Gastrin levels | Very high (>1000 pg/mL) |
| Ulcers | Multiple, unusual sites (jejunum), recurrent |
| Diarrhea + Steatorrhea | Excess H+ inactivates pancreatic lipase |
| Diagnosis | Secretin stimulation test (gastrin paradoxically rises in ZES); CT/MRI to locate tumor |
| Treatment | High-dose PPI + surgical resection of tumor; if metastatic, somatostatin analogues |
Key Exam Points to Remember
- "No acid, no ulcer" - Schwartz's Surgery principle
- H. pylori causes DU indirectly (inhibits somatostatin → excess gastrin) and GU directly (mucosal barrier destruction)
- Urease test principle: H. pylori urease + 13C-urea → 13CO2 (expired in breath)
- Gastric ulcers: biopsy is mandatory to exclude malignancy; duodenal ulcers do not require biopsy
- Metabolic complication of GOO: hypochloraemic hypokalaemic metabolic alkalosis
- The most common complication of PUD is bleeding; the most dangerous is perforation
- Posterior DU erodes into gastroduodenal artery → bleeding; posterior GU erodes into pancreas → penetration
- PPIs work better than H2 blockers because they act at the final common pathway of acid secretion
- NSAIDs cause ulcer by COX-1 inhibition → loss of prostaglandin → less mucus, less HCO3-, less blood flow
- Zollinger-Ellison: multiple ulcers + diarrhea + high gastrin; secretin test is diagnostic
Sources
- Guyton & Hall Textbook of Medical Physiology, Chapter 67 (Peptic Ulcer)
- Robbins & Kumar Basic Pathology, Chapter 13 (Peptic Ulcer Disease)
- Costanzo Physiology 7th Edition, Chapter 8 (Table 8.4)
- Bailey & Love's Short Practice of Surgery 28th Edition, Chapter 67