Shoulder joint ligament
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive overview of the shoulder joint ligaments, drawn from multiple authoritative orthopaedic and anatomy textbooks.
Shoulder Joint Ligaments
The shoulder (glenohumeral) joint is the most mobile joint in the body, gaining that mobility at the cost of bony stability. Ligamentous support is therefore critical for maintaining static stability.
Diagrams
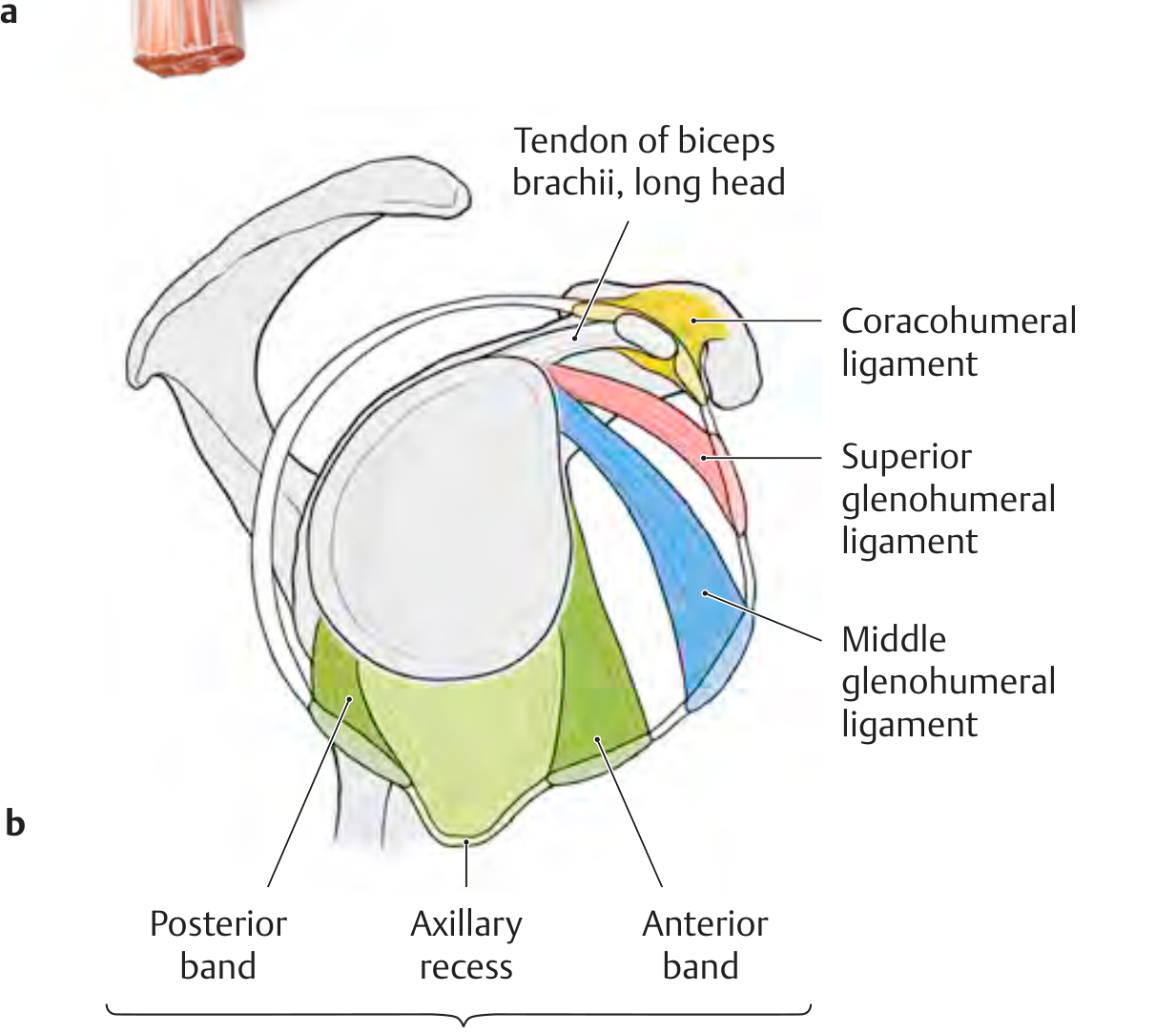
Left: Coracohumeral ligament and rotator interval, superior view. Right: All three glenohumeral ligaments with the IGHL's three components (anterior band, axillary recess, posterior band).
1. Glenohumeral Ligaments (GHLs)
These are fibrous thickenings of the anterior joint capsule - the primary passive stabilizers of the shoulder. They are usually only clearly visible arthroscopically or when viewed from inside the joint. Three ligaments are recognized:
A. Superior Glenohumeral Ligament (SGHL)
- Attachment: Anterosuperior glenoid rim (near apex of labrum, conjoined with long head of biceps) → intertubercular groove and lesser tubercle of humerus
- Function: Limits inferior translation and external rotation of the adducted shoulder. Together with the coracohumeral ligament, it forms the rotator interval
- Taut position: 0° abduction (arm at side)
B. Middle Glenohumeral Ligament (MGHL)
- Attachment: Upper margin of glenoid cavity → anatomic neck of humerus (passes almost at a right angle to the subscapularis tendon)
- Function: Secondary restraint to anterior translation; limits external rotation at ~45° abduction
- Clinical note: Highly variable in size - may be absent (e.g., Buford complex: cord-like MGHL + absent anterosuperior labrum, found in ~1.5-2% of individuals)
C. Inferior Glenohumeral Ligament (IGHL)
- The most important glenohumeral ligament
- Attachment: Inferior glenoid margin → distal lesser tuberosity / proximal humeral shaft
- Three components:
- Anterior band (ABIGHL) - primary restraint to anterior dislocation; most important restraint in abduction + external rotation
- Posterior band (PBIGHL) - resists posterior instability in flexion + internal rotation
- Axillary pouch (recess) - lies between the two bands; forms a "hammock" during abduction
- Function: Primary restraint to anterior, posterior, and inferior glenohumeral translation. The major restraint to external rotation in neutral and abducted positions
- Taut position: Arm in abduction and external rotation
2. Coracohumeral Ligament (CHL)
- Attachment: Base of coracoid process → greater and lesser tubercles of humerus (two parts/bands)
- Function:
- Limits inferior translation and external rotation of the adducted shoulder (in conjunction with SGHL)
- Stabilizes the tendon of the long head of biceps brachii as it passes through the intertubercular groove
- Forms the roof of the rotator interval (together with SGHL and part of the joint capsule)
- Clinical note: Contracture of the CHL is implicated in adhesive capsulitis (frozen shoulder)
3. Coracoacromial Ligament (CAL)
- Attachment: Undersurface of the medial acromion → superolateral border of coracoid process
- Function:
- Forms the coracoacromial arch (with acromion and coracoid) - provides a roof over the humeral head, prevents superior dislocation
- Acts as a tension band between acromion and coracoid, transmitting forces from surrounding muscles
- The subacromial bursa lies between the CAL and the rotator cuff tendons
- Clinical note: The CAL limits upward movement of the humerus. Thickening or osteophytes under it cause subacromial impingement
4. Transverse Humeral Ligament
- Attachment: Greater tubercle → lesser tubercle of humerus
- Function: Bridges the intertubercular (bicipital) groove, holding the long head of the biceps tendon in place within the groove
- Clinical note: Disruption can allow the biceps tendon to sublux or dislocate out of the groove
5. Rotator Interval
A region (not a single ligament) between the supraspinatus and subscapularis tendons, composed of:
- SGHL
- Coracohumeral ligament
- Part of the joint capsule
The long head of biceps passes through this interval. Rotator interval closure decreases external rotation in shoulder adduction and reduces posteroinferior translation.
Positional Function Summary
| Arm Position | Primary Stabilizing Ligament |
|---|---|
| 0° (adduction) | SGHL + CHL |
| ~45° abduction | MGHL |
| 90° abduction + ER | IGHL (anterior band) |
| Flexion + IR | IGHL (posterior band) |
Key Clinical Points
- The capsule is broad and thin posteriorly - not reinforced by ligaments, hence posterior dislocations can occur with fewer restraints
- The axillary recess (inferior capsular fold) provides reserve capacity for abduction; with prolonged disuse it can become atrophic - contributing to adhesive capsulitis
- The joint cavity communicates with the subtendinous bursa of subscapularis and the biceps tendon sheath within the intertubercular groove
- The IGHL anterior band is the single most important restraint to anterior dislocations
Sources: General Anatomy and Musculoskeletal System - THIEME Atlas of Anatomy, p. 284-285; Rheumatology 2-Volume Set (2022, Elsevier), p. 79; Imaging Anatomy Text and Atlas Vol. 3, p. 481
Simplify
Shoulder Joint Ligaments - Simplified
The shoulder is the most mobile joint in the body, so it needs strong ligaments to stay stable.
The Main Ligaments
1. Glenohumeral Ligaments (3 bands on the front of the joint)
These thicken the front of the joint capsule. Think of them as three straps running from the glenoid (socket) to the humerus (arm bone).
| Ligament | Job |
|---|---|
| Superior (SGHL) | Stabilizes arm hanging at the side |
| Middle (MGHL) | Stabilizes at ~45° arm raise |
| Inferior (IGHL) | Most important - prevents dislocation when arm is raised and rotated out |
The IGHL has 3 parts: anterior band, posterior band, and axillary pouch (like a hammock under the joint).
2. Coracohumeral Ligament
- Runs from the coracoid process → humerus
- Stops the arm from dropping downward when at rest
- Keeps the biceps tendon in its groove
3. Coracoacromial Ligament
- Runs from coracoid process → acromion
- Forms a roof over the shoulder (coracoacromial arch)
- Prevents the humeral head from popping upward
- When this arch is too tight → impingement syndrome
4. Transverse Humeral Ligament
- A small strap across the bicipital groove
- Holds the biceps tendon in place
Simple Memory Aid
"3 GH bands front, 1 roof above, 1 strap on top, 1 strap across the groove"
This is a shared conversation. Sign in to Orris to start your own chat.