Scabies
Reading File
Finding Sources
Searching PubMed
scabies treatment management
Reading File
Reading File
Searching Images
scabies mite burrow skin rash
Reading File
Reading File
Reading File
Now I have comprehensive information. Let me compile the full response.
Scabies
Overview
Scabies is an infestation of the epidermis by the mite Sarcoptes scabiei var. hominis (class Arachnida, family Sarcoptidae). It affects over 100 million persons annually worldwide, crossing all ages, races, and socioeconomic levels. Prevalence in some underdeveloped regions reaches 4–100% of the population.
The Mite
- Pearl-like, translucent, white, oval, eyeless; 4 pairs of short stubby legs
- Adult female: ~0.4 × 0.3 mm (just below naked-eye visibility); male slightly smaller
- Cannot fly or jump
- Survives 3 days off-host in air; up to 7 days in mineral oil
- Entire life cycle completed on human skin
Life cycle: The female excavates a burrow of 0.5–5 mm/day in the stratum corneum (up to 1 cm long), laying 0–4 eggs/day (~50 total over her 30-day lifespan). Eggs hatch in 10–12 days → larvae → nymphs (on skin surface) → adults.
A normal host harbors 3–50 mites. Crusted (Norwegian) scabies hosts may harbor millions.
Transmission
- Primary route: Close, prolonged skin-to-skin contact (sexual and non-sexual)
- Fomites: Bedding, clothing, upholstered furniture — especially relevant in crusted scabies (6,000 mites/g of debris documented)
- Occurs more commonly in winter months
Clinical Features
Incubation: 4–6 weeks after primary infestation (symptoms can be delayed up to 3 months). On reinfection, symptoms develop within 2–3 days.
Cardinal symptom: Intense nocturnal pruritus
Distribution (adults):
- Interdigital web spaces (hands)
- Sides of fingers, volar wrists, lateral palms
- Elbows, axillae
- Scrotum, penis, labia, areolae
- Periumbilical skin, buttocks
- Head and neck spared in healthy adults
In infants/young children: Face, scalp, palms, soles involved; lesions are often papules and vesicopustules; nodular lesions in intertriginous areas
Pathognomonic lesion: The burrow — a thin, thread-like, linear or J-shaped tunnel, 1–10 mm long, in the stratum corneum. Best seen in interdigital webs and wrists.
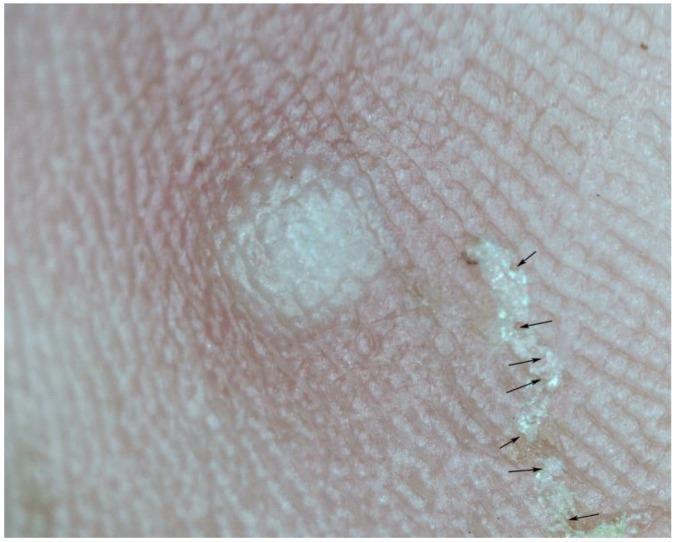
Scabies burrow at 15× magnification showing the serpentine tunnel in the stratum corneum with the "delta sign" mite at the leading edge.
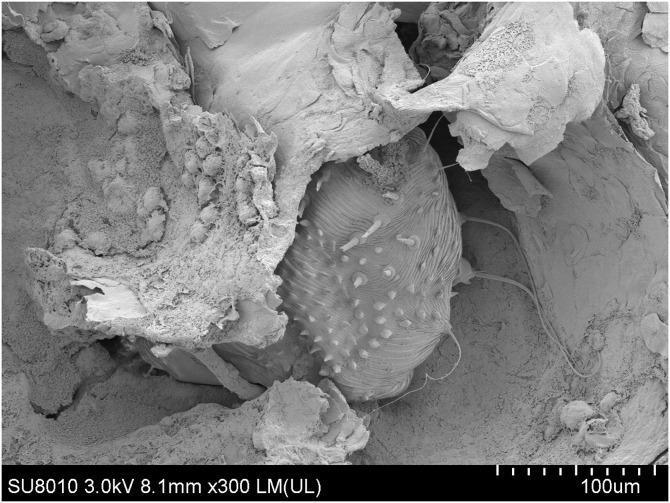
SEM (×300) of an adult female S. scabiei within a cutaneous burrow. Fecal pellets (scybala) are visible alongside the mite.
Crusted (Norwegian) Scabies
- Occurs in immunosuppressed patients (HIV with CD4 <200/mm³), elderly, those with neuropathy or dementia, leprosy, paraplegia
- Hyperkeratotic, grayish-white plaques — palmar/plantar predominance; nail thickening and dystrophy
- Paradoxically minimal or absent pruritus despite millions of mites
- Highly contagious — nosocomial outbreaks documented
- Head and neck commonly affected (unlike classic scabies)
- Can mimic seborrheic dermatitis, psoriasis, drug eruptions, eczema
Diagnosis
Clinical: Based on characteristic pruritus, distribution, and exposure history.
Definitive (laboratory):
- Mineral oil preparation of skin scrapings from a burrow → microscopic identification of mites, eggs, or fecal pellets (scybala)
- Dermoscopy: "Delta sign" / "jet sign" — triangular dark structure at the leading end of the burrow
- KOH preparation of skin scrapings
- PCR for S. scabiei DNA (emerging technique)
Burrow identification tip: Ink test (apply ink over suspected burrow, wipe off — ink tracks into the burrow channel).
Differential Diagnosis
| Most Likely | Also Consider |
|---|---|
| Atopic dermatitis | Dermatitis herpetiformis |
| Dyshidrotic eczema | Psoriasis |
| Contact dermatitis | Bullous pemphigoid |
| Insect bite reactions | Linear IgA bullous dermatosis |
| Pyoderma / Id reaction | Drug eruption |
| Varicella, miliaria | Delusions of parasitosis |
| Pityriasis rosea | Secondary syphilis |
Treatment
All household members and close contacts must be treated simultaneously, regardless of symptoms (asymptomatic carriers are common).
| Drug | Dose | Notes |
|---|---|---|
| Permethrin 5% cream (first-line) | Apply neck-down, 8–14 h, wash off; repeat in 7 days. Crusted: daily × 7 days then twice weekly until cured | Pregnancy category B; most effective topical agent; tolerance emerging |
| Ivermectin 200 µg/kg oral | Days 1 and 8; crusted: days 1, 2, 8, 9, 15 | Highly effective; avoid in <15 kg children, pregnancy, lactation |
| Crotamiton 10% cream | Apply days 1, 2, 3, and 8 | Also antipruritic; marginal efficacy |
| Precipitated sulfur 5–10% | Apply days 1, 2, and 3 | Safe in neonates and pregnancy; limited data |
| Benzyl benzoate 10% | Apply 24 h | Not available in USA |
| (avoid) | FDA black-box warning (neurotoxicity, seizures); banned in California; resistance documented |
Crusted scabies: Combination of topical permethrin + repeated oral ivermectin is recommended. Add keratolytic agents to facilitate scale removal.
HIV-associated crusted scabies: Treat with combined permethrin + multi-dose ivermectin; watch for bacterial superinfection and septicemia.
Adjunct measures
- Oral antihistamines and emollients for pruritus (avoid harsh soaps)
- Environmental decontamination: Wash sheets and clothing at ≥60°C (140°F) and tumble-dry on high heat
- Items that cannot be washed: seal in a plastic bag for 2 weeks
Post-treatment note
Pruritus may persist for 2–4 weeks after successful eradication due to ongoing hypersensitivity reaction — this does not indicate treatment failure.
Complications
- Secondary bacterial infection (impetigo, cellulitis) — especially in children
- Post-streptococcal glomerulonephritis (in endemic areas)
- Fatal septicemia in immunocompromised hosts with crusted scabies
Sources: Fitzpatrick's Dermatology (8e), Rosen's Emergency Medicine (10e), Dermatology 2-Volume Set (5e) — Goldman-Cecil Medicine (2e)
This is a shared conversation. Sign in to Orris to start your own chat.