Hemiperasis
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have enough comprehensive textbook content to give a thorough answer on hemiparesis. Let me compile the full response.
Hemiparesis
Hemiparesis means unilateral weakness (partial loss of motor function) affecting the face, arm, and leg on the same side of the body. When complete, it is called hemiplegia. It is always a sign of an upper motor neuron (UMN) lesion - meaning the problem is in the brain or spinal cord, not the peripheral nerves or muscles.
Terminology for Weakness Patterns
| Term | Meaning |
|---|---|
| Monoparesis/monoplegia | One limb |
| Hemiparesis/hemiplegia | One side (face + arm + leg) |
| Paraparesis/paraplegia | Both legs |
| Quadriparesis/quadriplegia | All four limbs |
(Neuroanatomy through Clinical Cases, 3rd Ed.)
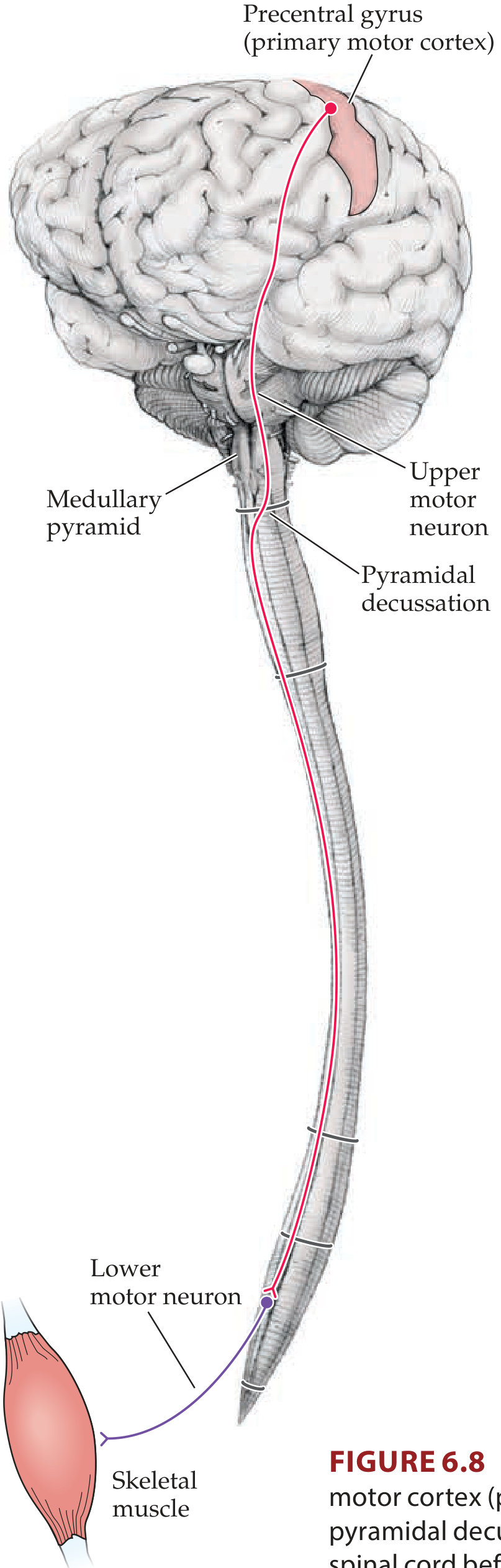
Anatomy of the Corticospinal Tract
The pathway responsible for voluntary motor control runs from:
- Primary motor cortex (precentral gyrus) - somatotopically organized (homunculus); face is lateral, leg is medial
- Corona radiata - white matter fan below cortex
- Internal capsule (posterior limb) - face fibers most anterior, then arm, then leg; very compact
- Cerebral peduncle (midbrain)
- Basis pontis (pons)
- Pyramidal decussation at the medullary-spinal junction - ~85% of fibers cross here
- Lateral corticospinal tract in the contralateral spinal cord
- Anterior horn lower motor neurons
Because the fibers cross at the pyramidal decussation, a lesion above the decussation causes contralateral hemiparesis, while a lesion below (spinal cord) causes ipsilateral weakness.
Types of Hemiparesis by Pattern
1. Pure Motor Hemiparesis (Face + Arm + Leg, No Sensory Loss)
- Rules out: Cortex (hard to involve the entire motor strip without some sensory loss); peripheral nerve/muscle (would require coincidental involvement of face, arm and leg on one side); spinal cord/medulla (face would be spared)
- Rules in: Corticospinal/corticobulbar tracts below the cortex and above the medulla: corona radiata, posterior limb of the internal capsule, basis pontis, or cerebral peduncle
- Side of lesion: Contralateral (above pyramidal decussation)
- Common causes: Lacunar infarct of the internal capsule (lenticulostriate or anterior choroidal artery) or pons (median perforating branches of the basilar artery); demyelination (MS); tumor; abscess
- Associated features: UMN signs (spasticity, hyperreflexia, Babinski); often dysarthria ("dysarthria - pure motor hemiparesis"); occasional ataxia of the affected side (ataxic hemiparesis) if cerebellar/pontine pathways are also involved
(Neuroanatomy through Clinical Cases, 3rd Ed., p. 266)
2. Hemiparesis Sparing the Face (Arm + Leg Only, No Face)
- Locations ruled in: Arm and leg areas of the motor cortex; corticospinal tract from lower medulla to C5 level
- Side of lesion: Contralateral (cortex or medulla above decussation); ipsilateral (cervical spinal cord, below decussation)
- Associated features: UMN signs; cortical lesions in watershed territory affect proximal more than distal muscles ("man in a barrel"); may have Brown-Sequard syndrome if spinal cord lesion; medial medullary lesion may add ipsilateral vibration/position loss and contralateral tongue weakness
- Common causes: Watershed infarct (ACA-MCA territory); medial medullary infarct; multiple sclerosis; cervical spinal cord compression/trauma
3. Face and Arm Weakness (No Leg) - Faciobrachial Paresis
- Location: Face and arm area of primary motor cortex (lateral frontal convexity)
- Side of lesion: Contralateral
- Associated features: Dysarthria, UMN signs; in dominant hemisphere - Broca's aphasia; in non-dominant hemisphere - hemineglect; sensory loss if extends to parietal lobe
- Classic cause: MCA superior division infarct
UMN vs. LMN Signs
Because hemiparesis is an UMN lesion, signs include:
| Feature | UMN (Hemiparesis) | LMN |
|---|---|---|
| Tone | Increased (spastic) | Decreased (flaccid) |
| Reflexes | Hyperreflexia | Hyporeflexia/absent |
| Babinski sign | Present (extensor plantar) | Absent |
| Muscle wasting | Minimal (late) | Prominent (early) |
| Fasciculations | Absent | May be present |
Note: In the acute phase of stroke, the affected limbs may be initially flaccid ("shock phase") before spasticity develops over days to weeks.
Localization Summary
| Location of Lesion | Pattern | Clues |
|---|---|---|
| Motor cortex (lateral) | Face + arm (leg spared) | Broca aphasia (dominant), hemineglect |
| Motor cortex (medial/parasagittal) | Leg >> arm (face spared) | ACA territory, "man in barrel" if bilateral |
| Internal capsule (posterior limb) | Pure motor hemiparesis | Lacunar infarct; compact bundle = full hemiplegia |
| Midbrain (cerebral peduncle) | Pure motor hemiparesis + CN III palsy (contralateral) | Weber syndrome |
| Pons (basis pontis) | Pure motor hemiparesis | Severe dysarthria, dysphagia; CN VI or VII palsy ipsilateral |
| Medulla (medial) | Arm + leg weakness + ipsilateral tongue, contralateral vibration loss | Medial medullary syndrome |
| Cervical spinal cord | Ipsilateral arm + leg | Brown-Sequard if hemisection |
Common Causes
- Ischemic stroke - most common overall (MCA territory, lacunar infarcts)
- Hemorrhagic stroke - putaminal, thalamic, pontine hemorrhage
- Brain tumor - primary or metastatic (progressive onset)
- Multiple sclerosis - young adults, relapsing-remitting, Uhthoff phenomenon (worsens with heat)
- Brain abscess - fever, raised ICP, ring-enhancing lesion
- Subdural/epidural hematoma - head trauma history
- Todd's paralysis - transient hemiparesis after a focal seizure
- Hemiplegic migraine - rare, reversible
Detecting Subtle Hemiparesis at the Bedside
- Pronator drift test: Outstretched arms, palms up, eyes closed - the weak side pronates and drifts downward
- Arm swing on walking: Reduced on the paretic side
- Facial asymmetry: Decreased nasolabial fold; lower facial droop (UMN lesions spare forehead because forehead has bilateral cortical representation)
- Finger tapping: Slower rhythm on weak side
- Babinski sign: Extensor plantar response on affected side
Key Clinical Pearls
- Pure motor hemiparesis without sensory, visual, or cortical signs strongly localizes to the internal capsule or basis pontis (lacunar territory) - not the cortex.
- A previous history of vertigo or gait unsteadiness before pure motor hemiparesis favors a pontine over a capsular lesion.
- Dysarthria + hemiparesis is classically a pontine or capsular syndrome.
- Ataxia + hemiparesis (ataxic hemiparesis) typically localizes to the basis pontis (junction of upper 1/3 and lower 2/3), with hemiparesis worse in the leg.
(Localization in Clinical Neurology, 8e; Neuroanatomy through Clinical Cases, 3rd Ed.)
This is a shared conversation. Sign in to Orris to start your own chat.