Sugery for olorectal carcinoma and main steps and which all structure removaed and different in table from and with diagram if possible
colorectal carcinoma surgery types steps structures removed comparison
Surgery for Colorectal Carcinoma (CRC)
Overview Comparison Table
| Feature | Right Hemicolectomy | Left Hemicolectomy | Sigmoid Colectomy | High Anterior Resection (HAR) | Low Anterior Resection (LAR) | Abdominoperineal Excision (APE) | Hartmann's Procedure | Pelvic Exenteration |
|---|---|---|---|---|---|---|---|---|
| Tumour location | Caecum, ascending, hepatic flexure, proximal transverse colon | Descending colon, splenic flexure | Sigmoid colon | Upper rectum (>12 cm from anal verge) | Middle/lower rectum (5-12 cm) | Low rectum/anus (distal 3rd, <5 cm from verge) | Sigmoid/upper rectum (unfit/frail patients) | Locally advanced rectum invading adjacent organs |
| Structures removed | Terminal ileum (10-15 cm), caecum, ascending colon, hepatic flexure, proximal transverse colon, associated mesocolon, ileocolic and right colic lymph nodes | Descending colon, splenic flexure, part of transverse colon, associated mesocolon, left colic LNs | Sigmoid colon, mesosigmoid, sigmoid vessels, LNs | Upper rectum (≥3 cm below tumour), mesorectum (partial TME), sigmoid colon, superior rectal vessels, LNs | Upper + middle + lower rectum (complete TME), mesorectum en bloc, sigmoid colon, pelvic LNs | Sigmoid colon, entire rectum, mesorectum, anus, anal sphincters, levator ani, ischiorectal fat, perineal skin, pelvic LNs | Sigmoid colon + rectum (stump closed), no anastomosis | All APE structures PLUS bladder ± prostate (male), or uterus ± posterior vaginal wall (female) |
| Anastomosis | Ileocolic (ileum to transverse colon) | Colorectal or colo-colic | Colorectal | Colorectal | Colorectal (stapled, low) | None - end colostomy | None - end colostomy (rectal stump closed) | Colostomy ± ileal conduit (if bladder removed) |
| Stoma | Usually none | Usually none | Usually none | Usually none | Defunctioning loop ileostomy often used | Permanent end-colostomy (left iliac fossa) | Permanent end-colostomy | Permanent colostomy ± urostomy |
| Anal sphincter preserved? | Yes | Yes | Yes | Yes | Yes | No | Yes | No (if APE component) |
| TME performed? | No | No | No | Partial (proximal TME) | Complete TME | Complete TME + extralevator excision | No | Complete |
| Key vessels ligated | Ileocolic artery, right colic artery, right branch of middle colic artery | Left colic artery, inferior mesenteric artery | Inferior mesenteric artery or sigmoid vessels | Superior rectal artery, IMA (high ligation) | IMA at origin or just distal (high ligation) | IMA, middle rectal vessels, pudendal branches | IMA | IMA + internal iliac vessels |
1. Right Hemicolectomy
Steps:
- Incision - Midline laparotomy or right-sided laparoscopic ports
- Exploration - Assess liver, peritoneum for metastases
- Mobilisation - Divide peritoneal reflection lateral to ascending colon (white line of Toldt), reflect medially
- Ureter and duodenum identification - Protected during dissection (right ureter, second part of duodenum)
- Vascular ligation - High ligation of ileocolic artery, right colic artery, and right branch of middle colic artery at their origins (CME principle)
- Mesocolon division - En bloc with draining lymph nodes (complete mesocolic excision, CME)
- Bowel transection - Terminal ileum (10-15 cm proximal) and mid-transverse colon
- Anastomosis - Ileocolic anastomosis (hand-sewn or stapled)
2. Left Hemicolectomy
Steps:
- Incision - Midline or laparoscopic approach
- Splenic flexure mobilisation - Divide gastrocolic and splenocolic ligaments
- Left ureter identification and protection
- Vascular ligation - Inferior mesenteric artery (IMA) or left colic artery ligation
- Mesocolon division (CME)
- Bowel transection - Proximal transverse colon to upper sigmoid/rectosigmoid junction
- Anastomosis - Colo-rectal or colo-colic
3. Sigmoid Colectomy
Steps:
- Mobilise sigmoid colon by dividing lateral peritoneal attachments
- Identify and protect left ureter (crosses iliac vessels)
- High ligation of IMA or sigmoid branches
- Divide sigmoid mesentery with lymph node clearance
- Bowel transection: proximal sigmoid to upper rectum
- Colorectal anastomosis (stapled or hand-sewn)
4. Anterior Resection (AR) - for Rectal Cancer
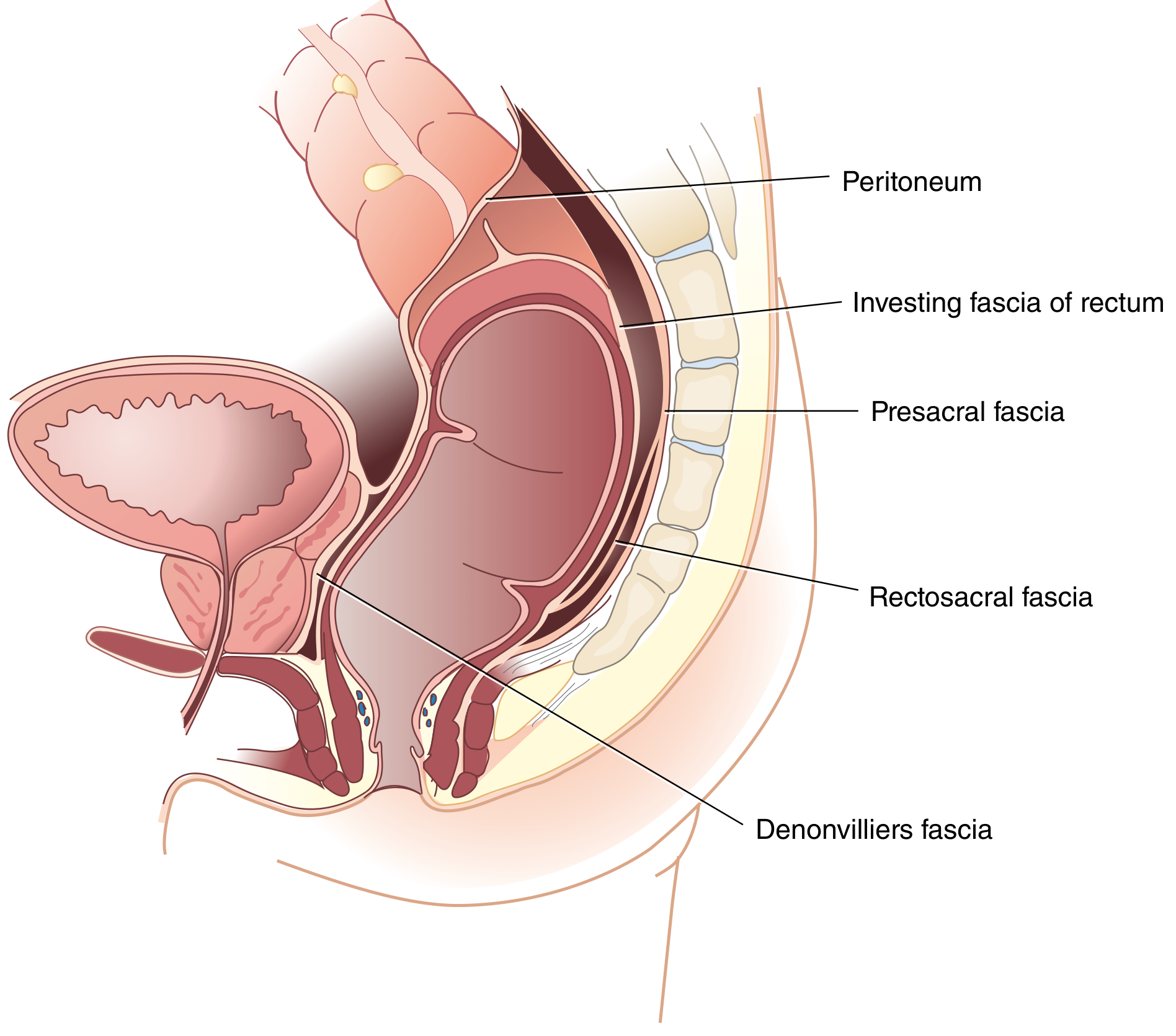
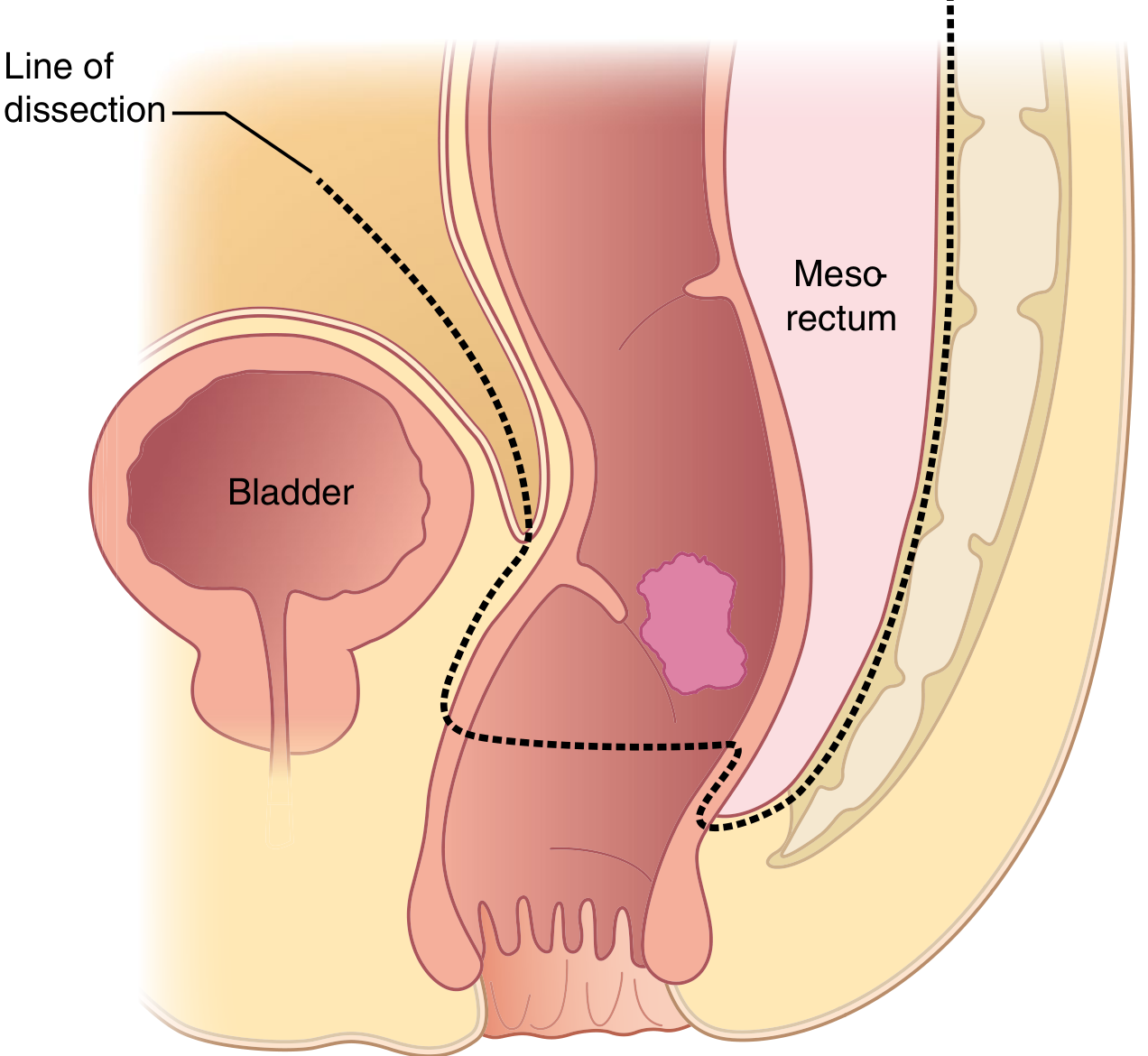
TME: Sharp dissection in the embryological plane between the investing fascia of the rectum (fascia propria) and the presacral/parietal pelvic fascia, removing the rectum en bloc with its intact mesorectum. This reduces local recurrence from ~25% to ~6% and improves 5-year survival from ~60% to ~73%.
Surgical Steps (Open / Laparoscopic / Robotic):
- Midline incision (or laparoscopic port placement)
- Full laparotomy - Assess for synchronous lesions, metastases
- Sigmoid and descending colon mobilisation - Divide left peritoneal reflection, mobilise to midline; protect left ureter and gonadal vessels
- Splenic flexure mobilisation - To achieve tension-free anastomosis
- IMA ligation - High ligation at or just below aorta (preserving superior hypogastric plexus where possible)
- Posterior rectal dissection - In the TME plane: anterior to presacral fascia, posterior to fascia propria; preserve hypogastric nerves over sacral promontory
- Lateral rectal dissection - Divide lateral ligaments; preserve pelvic plexuses (S2, S3, S4 parasympathetics)
- Anterior rectal dissection - Anterior to Denonvilliers' fascia (between rectum and prostate/seminal vesicles in male; rectum and vagina in female)
- Distal rectal transection - With linear stapler:
- High AR: at least 3 cm below the tumour (upper rectum)
- Low AR: at the anorectal junction (middle/lower rectum - complete TME)
- Proximal colonic transection - With adequate proximal margin
- Stapled colorectal anastomosis - Circular stapler per anum (end-to-end or end-to-side)
- Covering loop ileostomy - Often formed for low anastomoses to protect the join
Structures Removed:
- Sigmoid colon and upper rectum (with tumour)
- Complete mesorectum (in LAR) with all contained lymph nodes
- Superior rectal and inferior mesenteric vessels
5. Abdominoperineal Excision of the Rectum (APER / Miles' Operation)
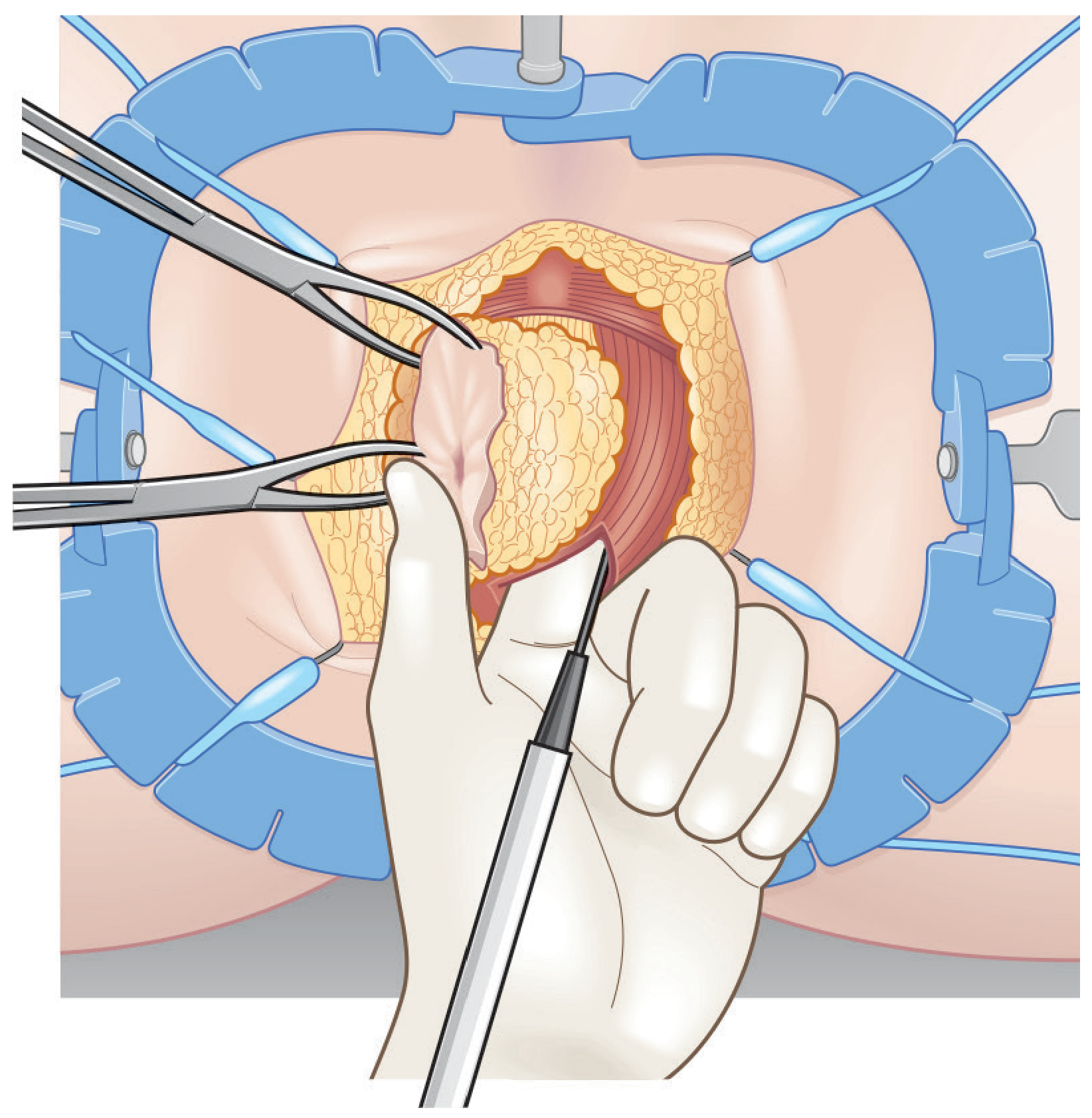
Surgical Steps:
- Midline laparotomy or laparoscopic access
- Identical dissection to anterior resection up to the level of the seminal vesicles (male) or cervix (female) - then stop, do NOT "cone down" onto the tumour
- IMA ligation, mobilisation of sigmoid colon
- Sigmoid divided proximally; proximal end brought out as end colostomy in left iliac fossa
- Dissection purposely stops before reaching pelvic floor (to avoid thin margins)
- Patient repositioned (prone jack-knife or Lloyd-Davies lithotomy)
- Circumanal incision - Elliptical incision around anus (anus sutured closed prior to incision)
- Deepened into ischiorectal fossae bilaterally, extending toward levator muscle attachment at pelvic side wall
- Posterior dissection - Waldeyer's (rectosacral) fascia is incised posteriorly; coccyx may be removed to improve access
- Anterior dissection - Plane between rectum and prostate/membranous urethra (male - catheter palpated to protect urethra) or between rectum and posterior vaginal wall (female)
- Levator ani division - Pubococcygeus and puborectalis divided from pelvic side wall
- Specimen retrieved through perineal wound en bloc
- Perineal wound closed with drains to pelvis
Structures Removed (APER):
- Sigmoid colon + entire rectum + mesorectum
- Anus + anal canal
- Internal AND external anal sphincters
- Levator ani muscles (pubococcygeus, puborectalis, iliococcygeus)
- Ischiorectal fat bilaterally
- Perineal skin (elliptical)
- All pelvic lymph nodes
- Optional: coccyx (if needed for access/margins)
- In females with anterior tumour: posterior vaginal wall
6. Hartmann's Procedure
Steps:
- Rectal stump is stapled closed (Hartmann's pouch)
- Proximal colon is brought out as a permanent end-colostomy
- No anastomosis is made
- Reversal is possible later, but often not undertaken
7. Pelvic Exenteration
| Type | Structures Removed |
|---|---|
| Posterior exenteration | Rectum + posterior vagina/uterus |
| Total exenteration | Rectum + bladder + prostate (male) OR rectum + uterus + bladder (female) |
| Extended | Above + sacrum, pelvic side wall muscles |
- Requires colostomy + ileal conduit (urinary diversion if bladder removed)
- Perineal defect reconstructed with rectus abdominis or gluteal flap
Key Structures Preserved (Nerves at Risk)
| Nerve | Origin | Function | At Risk During |
|---|---|---|---|
| Hypogastric plexus (sympathetic) | L1-L3 (preaortic) | Ejaculation, bladder neck closure | IMA high ligation, sacral promontory dissection |
| Pelvic plexus (parasympathetic) | S2, S3, S4 (nervi erigentes) | Erection, bladder voiding | Lateral rectal dissection |
| Pudendal nerve | S2-S4 | Anal sphincter tone, perineal sensation | Perineal phase of APER |
| Left ureter | Retroperitoneal | Urine drainage | Left colon / sigmoid mobilisation |
| Membranous urethra | - | Urinary continence | Anterior dissection in APER (male) |
Comparison: LAR vs. APER
| Feature | Low Anterior Resection (LAR) | Abdominoperineal Excision (APER) |
|---|---|---|
| Tumour level | Middle/upper rectum | Lower rectum / invades sphincter |
| Anal sphincters | Preserved | Excised |
| Stoma | Temporary covering ileostomy | Permanent end-colostomy |
| TME type | Complete | Complete + extralevator (cylindrical) |
| Approach | Abdominal only | Abdominal + perineal |
| Anastomosis | Yes (stapled) | No |
| Local recurrence risk | Low (with TME) | Low (with extralevator excision) |
| Positive CRM risk | Lower | Higher if standard (reduced with extralevator APER) |
Sources
- Bailey and Love's Short Practice of Surgery, 28th Edition, Chapter 79 (pp. 1434-1436)
- Sabiston Textbook of Surgery, 21st Edition, Chapter 96 (pp. 2137-2139)
- Fischer's Mastery of Surgery, 8th Edition, Chapter 145 (Mesorectal Anterior Excision)
- Yamada's Textbook of Gastroenterology, 7th Edition (Surgical treatment for rectal cancer)
Generate a detailed surgical atlas poster showing TME dissection planes
Detailed surgical atlas poster titled "Total Mesorectal Excision (TME) - Dissection Planes" for medical education. Scientific anatomical illustration style with clean white background. Main central illustration: Large sagittal cross-section of male pelvis showing: - Rectum in center with clearly labeled mesorectum (fatty envelope around rectum) - Tumor shown as pink nodule in mid-rectum - Labeled dissection planes with colored dotted/dashed lines: * POSTERIOR plane: between presacral fascia (Waldeyer's fascia) and fascia propria of rectum (mesorectal investing fascia) - shown in blue dotted line * ANTERIOR plane: anterior to Denonvilliers' fascia, between rectum and prostate/seminal vesicles - shown in red dotted line * LATERAL planes: along pelvic side walls - shown in green dotted line - Anatomical labels pointing to: Sacrum, Presacral fascia, Fascia propria of rectum, Mesorectum, Denonvilliers' fascia, Prostate, Seminal vesicles, Bladder, Peritoneum, Levator ani, Waldeyer's rectosacral fascia, Puborectalis, Anal canal, Anococcygeal ligament Top left inset diagram: Axial/cross-sectional view of rectum at mid-pelvis showing: - Concentric layers: rectal wall, mesorectum, investing fascia, parietal fascia - Circumferential resection margin (CRM) indicated - Label: "Holy Plane of TME" with arrow Top right inset: Posterior view showing hypogastric nerves and pelvic plexus with labels: - Superior hypogastric plexus - Left and right hypogastric nerves - Inferior hypogastric (pelvic) plexus - IMA (inferior mesenteric artery) stump - Sacral promontory - Nervi erigentes S2-S4 Bottom panel: Three-step sequential diagrams showing progression of TME dissection: Step 1 - "Posterior Dissection: Enter presacral space at sacral promontory" Step 2 - "Lateral Dissection: Divide lateral ligaments preserving pelvic nerves" Step 3 - "Anterior Dissection: Anterior to Denonvilliers' fascia" Bottom right inset: Completed TME specimen showing intact mesorectal envelope with label "Intact mesorectal fascia = oncologically correct TME" Color-coded legend box: - Blue = Posterior dissection plane - Red = Anterior dissection plane - Green = Lateral dissection planes - Yellow shading = Mesorectum - Orange = Nerves to preserve Title banner at top: "TOTAL MESORECTAL EXCISION (TME) - Surgical Dissection Planes" in bold dark blue Subtitle: "Anatomical Guide for Rectal Cancer Surgery" Footer: "Bailey & Love / Sabiston Surgical Atlas Reference" Professional medical atlas style, anatomically accurate, high detail, suitable for surgical training
mkdir -p /home/daytona/workspace/tme-poster && ls /home/daytona/workspace/tme-poster/
~/tme-poster/tme_atlas.py
"""
TME Surgical Atlas Poster - Total Mesorectal Excision Dissection Planes
"""
import matplotlib.pyplot as plt
import matplotlib.patches as mpatches
from matplotlib.patches import FancyArrowPatch, Arc, Ellipse, FancyBboxPatch, PathPatch
from matplotlib.path import Path
import matplotlib.patheffects as pe
import numpy as np
# ── Canvas ─────────────────────────────────────────────────────────────────
fig = plt.figure(figsize=(22, 28), facecolor='#F8F6F0')
fig.patch.set_linewidth(6)
fig.patch.set_edgecolor('#1a3a5c')
# Color palette
C = dict(
bg = '#F8F6F0',
title_bg = '#1a3a5c',
title_fg = '#FFFFFF',
bone = '#EDE0C4',
bone_dark = '#C8B89A',
rectum = '#C05050',
rectum_lm = '#8B2020',
mesrect = '#F4C4A0',
bladder = '#A0B8D8',
prostate = '#C4A0C8',
fascia = '#8B6914',
plane_p = '#1565C0', # posterior - blue
plane_a = '#C62828', # anterior - red
plane_l = '#2E7D32', # lateral - green
nerve = '#F57F17', # nerves - amber
lymph = '#4A148C', # lymphatics - purple
section_bg= '#E8F4FD',
heading = '#1a3a5c',
text = '#2C2C2C',
tumor = '#B71C1C',
levator = '#5D8A5E',
label_box = '#FFFFFFCC',
)
# ── Title Banner ────────────────────────────────────────────────────────────
title_ax = fig.add_axes([0, 0.945, 1, 0.055])
title_ax.set_facecolor(C['title_bg'])
title_ax.set_xlim(0,1); title_ax.set_ylim(0,1)
title_ax.axis('off')
title_ax.text(0.5, 0.70, 'TOTAL MESORECTAL EXCISION (TME)',
ha='center', va='center', fontsize=30, fontweight='bold',
color='white', fontfamily='DejaVu Sans')
title_ax.text(0.5, 0.20, 'Surgical Dissection Planes — Anatomical Atlas for Rectal Cancer Surgery',
ha='center', va='center', fontsize=15, color='#B0C4DE',
fontfamily='DejaVu Sans')
# ═══════════════════════════════════════════════════════════════════════════
# MAIN SAGITTAL DIAGRAM (left half, tall)
# ═══════════════════════════════════════════════════════════════════════════
main_ax = fig.add_axes([0.02, 0.32, 0.56, 0.60])
main_ax.set_facecolor(C['bg'])
main_ax.set_xlim(-1, 11); main_ax.set_ylim(-1, 14)
main_ax.axis('off')
main_ax.set_aspect('equal')
def filled_curve(ax, xs, ys, color, alpha=1.0, zorder=2, lw=1.5, ec=None):
ec = ec or color
ax.fill(xs, ys, color=color, alpha=alpha, zorder=zorder)
ax.plot(xs, ys, color=ec, lw=lw, zorder=zorder+1)
# ── Sacrum / Coccyx ─────────────────────────────────────────────────────────
sacrum_x = [6.5, 9.5, 9.8, 9.2, 9.4, 8.8, 9.0, 8.4, 8.2, 7.2, 6.5]
sacrum_y = [13.5, 13.5, 12.5, 11.5, 10.5, 9.5, 8.5, 7.5, 6.5, 5.5, 13.5]
filled_curve(main_ax, sacrum_x, sacrum_y, C['bone'], ec=C['bone_dark'], zorder=2)
# Coccyx
coccyx_x = [7.2, 8.2, 8.0, 7.6, 7.2]
coccyx_y = [5.5, 6.5, 5.0, 4.0, 5.5]
filled_curve(main_ax, coccyx_x, coccyx_y, C['bone'], ec=C['bone_dark'], zorder=2)
main_ax.text(8.8, 11.5, 'Sacrum', fontsize=10, color=C['text'], fontweight='bold', zorder=10)
main_ax.text(7.4, 4.5, 'Coccyx', fontsize=9, color=C['text'], zorder=10)
# ── Lumbar vertebra (top) ───────────────────────────────────────────────────
for yi, lbl in zip([13.0], ['L5']):
main_ax.add_patch(FancyBboxPatch((6.6, yi-0.4), 2.2, 0.8,
boxstyle="round,pad=0.05", fc=C['bone'], ec=C['bone_dark'], lw=1.5, zorder=3))
main_ax.text(7.7, yi, lbl, ha='center', va='center', fontsize=8, color=C['text'], zorder=10)
# ── Presacral fascia ────────────────────────────────────────────────────────
pf_x = [7.0, 8.8, 8.5, 8.0, 7.6, 7.2, 7.0]
pf_y = [13.0, 13.0, 11.2, 9.2, 7.2, 5.8, 13.0]
filled_curve(main_ax, pf_x, pf_y, '#D4B896', alpha=0.6, ec='#8B6914', lw=1.5, zorder=3)
main_ax.text(8.15, 9.8, 'Presacral\nfascia', fontsize=8.5, color=C['fascia'],
fontstyle='italic', zorder=10, ha='center')
# ── Waldeyer's fascia (rectosacral) ─────────────────────────────────────────
wald_x = np.array([4.8, 5.2, 5.8, 6.5, 7.0])
wald_y = np.array([5.8, 5.5, 5.2, 5.4, 5.8])
main_ax.plot(wald_x, wald_y, color='#5C4000', lw=2.5, ls='--', zorder=6)
main_ax.text(5.0, 5.0, "Waldeyer's fascia\n(rectosacral)", fontsize=8, color='#5C4000',
fontstyle='italic', zorder=10)
# ── Mesorectum (fatty envelope) ─────────────────────────────────────────────
meso_x = [3.5, 3.2, 3.0, 3.1, 3.4, 3.8, 4.2, 4.5, 4.8, 5.2, 5.8, 6.2,
6.8, 7.2, 7.5, 7.3, 6.8, 6.0, 5.0, 4.0, 3.5]
meso_y = [12.5, 11.5, 10.0, 8.5, 7.0, 6.0, 5.6, 5.5, 5.4, 5.2, 5.0, 5.2,
5.8, 6.5, 8.0, 10.0, 11.5, 12.5, 13.0, 12.8, 12.5]
filled_curve(main_ax, meso_x, meso_y, C['mesrect'], alpha=0.85, ec='#CC7733', lw=2, zorder=4)
main_ax.text(4.0, 9.0, 'Mesorectum\n(fatty envelope\nwith lymph nodes)', fontsize=9,
color='#884400', fontweight='bold', zorder=10, ha='center')
# ── Fascia propria of rectum (investing fascia) ──────────────────────────────
fp_x = [3.8, 3.6, 3.5, 3.6, 3.9, 4.2, 4.6, 4.8, 5.1, 5.5, 5.8, 6.2,
6.6, 6.9, 7.0, 6.8, 6.4, 5.8, 5.0, 4.2, 3.8]
fp_y = [12.2, 11.2, 9.8, 8.5, 7.2, 6.4, 6.0, 5.9, 5.8, 5.6, 5.5, 5.7,
6.2, 7.2, 8.5, 10.0, 11.2, 12.0, 12.5, 12.4, 12.2]
filled_curve(main_ax, fp_x, fp_y, '#F8D4B0', alpha=0.9, ec='#CC5500', lw=2.0, zorder=5)
# ── Rectum wall ──────────────────────────────────────────────────────────────
rect_x = [4.2, 4.0, 3.9, 4.0, 4.2, 4.5, 4.7, 5.0, 5.3, 5.6, 5.9, 6.1,
6.3, 6.5, 6.4, 6.2, 5.8, 5.3, 4.8, 4.2]
rect_y = [12.0, 11.0, 9.8, 8.5, 7.5, 6.8, 6.4, 6.2, 6.0, 5.9, 6.0, 6.2,
6.8, 7.5, 9.0, 10.5, 11.5, 12.2, 12.3, 12.0]
filled_curve(main_ax, rect_x, rect_y, '#D4706A', alpha=0.9, ec=C['rectum_lm'], lw=2, zorder=6)
main_ax.text(5.15, 9.2, 'RECTUM', fontsize=11, fontweight='bold',
color='white', ha='center', va='center', zorder=10)
# ── Tumor ────────────────────────────────────────────────────────────────────
tumor_patch = Ellipse((5.1, 7.5), 0.85, 0.65, fc=C['tumor'], ec='#800000', lw=2, zorder=8)
main_ax.add_patch(tumor_patch)
main_ax.text(5.1, 7.5, 'T', ha='center', va='center', fontsize=9, fontweight='bold',
color='white', zorder=9)
# ── Anal canal ───────────────────────────────────────────────────────────────
anal_x = [4.5, 4.3, 4.2, 4.3, 4.5, 5.0, 5.5, 5.7, 5.6, 5.4, 4.5]
anal_y = [5.5, 4.8, 4.0, 3.3, 2.8, 2.6, 2.8, 3.3, 4.0, 5.0, 5.5]
filled_curve(main_ax, anal_x, anal_y, '#A05050', ec='#703030', lw=1.5, zorder=7)
main_ax.text(5.0, 3.5, 'Anal\ncanal', fontsize=8.5, ha='center', color='white',
fontweight='bold', zorder=10)
# ── Levator ani ──────────────────────────────────────────────────────────────
lev_x = [3.0, 3.2, 3.6, 4.2, 4.5, 5.5, 6.0, 6.5, 7.0, 7.5, 7.5, 7.0,
6.5, 5.5, 4.5, 3.8, 3.2, 3.0]
lev_y = [4.5, 4.8, 5.0, 5.2, 5.3, 5.4, 5.3, 5.2, 5.0, 4.8, 4.2, 4.4,
4.5, 4.6, 4.5, 4.3, 4.0, 4.5]
filled_curve(main_ax, lev_x, lev_y, C['levator'], alpha=0.7, ec='#2E5E2E', lw=2, zorder=5)
main_ax.text(3.0, 4.6, 'Levator ani\n(puborectalis +\npubococcygeus)', fontsize=8,
color=C['levator'], fontstyle='italic', zorder=10)
# ── Bladder ──────────────────────────────────────────────────────────────────
bladder_patch = Ellipse((1.8, 9.5), 2.4, 3.2, fc=C['bladder'], ec='#1a5276', lw=2, alpha=0.85, zorder=5)
main_ax.add_patch(bladder_patch)
main_ax.text(1.8, 9.5, 'Bladder', ha='center', va='center', fontsize=9,
fontweight='bold', color='#1a5276', zorder=10)
# ── Prostate / Seminal vesicles ───────────────────────────────────────────────
prostate_patch = Ellipse((2.5, 7.0), 1.8, 1.2, fc=C['prostate'], ec='#6a0dad', lw=1.5, alpha=0.85, zorder=6)
main_ax.add_patch(prostate_patch)
main_ax.text(2.5, 7.0, 'Prostate', ha='center', va='center', fontsize=8.5,
fontweight='bold', color='white', zorder=10)
sv_patch = Ellipse((2.8, 8.1), 1.4, 0.7, fc='#D0B0E0', ec='#6a0dad', lw=1.5, alpha=0.85, zorder=6)
main_ax.add_patch(sv_patch)
main_ax.text(2.8, 8.1, 'Sem. vesicles', ha='center', va='center', fontsize=7.5,
color='#4a0078', zorder=10)
# ── Denonvilliers' fascia ─────────────────────────────────────────────────────
den_x = [3.5, 3.6, 3.8, 3.9, 4.0]
den_y = [8.8, 7.8, 7.0, 6.4, 6.0]
main_ax.plot(den_x, den_y, color='#8B0000', lw=3, ls='-.', zorder=8)
main_ax.text(1.5, 7.8, "Denonvilliers'\nfascia", fontsize=8.5, color='#8B0000',
fontstyle='italic', zorder=10, ha='center')
main_ax.annotate('', xy=(3.55, 8.3), xytext=(2.4, 8.0),
arrowprops=dict(arrowstyle='->', color='#8B0000', lw=1.5))
# ── Peritoneum reflection ─────────────────────────────────────────────────────
per_x = [0.5, 1.0, 1.5, 2.5, 3.2, 3.5, 3.6, 3.8, 4.0, 4.5, 5.0, 5.5, 5.8, 6.0,
6.2, 6.5, 7.0, 7.5, 8.0, 8.5, 9.0, 9.5, 10.5]
per_y = [13.8, 13.5, 13.0, 12.0, 11.5, 11.2, 10.8, 10.5, 10.4, 10.2, 10.0, 9.8, 9.7, 9.5,
9.2, 9.0, 9.2, 9.5, 10.0, 10.5, 11.0, 11.5, 12.0]
main_ax.plot(per_x, per_y, color='#2E8B57', lw=2.5, ls=':', zorder=7)
main_ax.text(1.2, 13.2, 'Peritoneum', fontsize=8.5, color='#2E8B57', fontstyle='italic', zorder=10)
# ═══════════════════════════════════════════════════════════════════════════════
# DISSECTION PLANE ARROWS & LABELS
# ═══════════════════════════════════════════════════════════════════════════════
# ── POSTERIOR plane (blue) ────────────────────────────────────────────────────
post_plane_x = np.linspace(6.0, 7.3, 30)
post_plane_y = np.linspace(12.0, 5.8, 30)
main_ax.plot(post_plane_x, post_plane_y, color=C['plane_p'], lw=4, ls='--',
dashes=(8,4), zorder=9, alpha=0.9)
# Arrow on the plane
main_ax.annotate('', xy=(6.8, 7.5), xytext=(6.5, 10.5),
arrowprops=dict(arrowstyle='->', color=C['plane_p'], lw=2.5))
# ── ANTERIOR plane (red) ──────────────────────────────────────────────────────
ant_plane_x = [3.8, 3.7, 3.6, 3.6, 3.7, 3.8, 3.9, 4.0]
ant_plane_y = [11.5, 10.5, 9.5, 8.5, 7.5, 6.8, 6.2, 5.8]
main_ax.plot(ant_plane_x, ant_plane_y, color=C['plane_a'], lw=4, ls='--',
dashes=(8,4), zorder=9, alpha=0.9)
main_ax.annotate('', xy=(3.7, 8.0), xytext=(3.9, 10.5),
arrowprops=dict(arrowstyle='->', color=C['plane_a'], lw=2.5))
# ── LATERAL planes (green) ────────────────────────────────────────────────────
main_ax.annotate('', xy=(4.0, 6.5), xytext=(2.5, 7.0),
arrowprops=dict(arrowstyle='->', color=C['plane_l'], lw=2.5,
connectionstyle='arc3,rad=0.2'))
main_ax.annotate('', xy=(6.5, 6.5), xytext=(8.0, 7.0),
arrowprops=dict(arrowstyle='->', color=C['plane_l'], lw=2.5,
connectionstyle='arc3,rad=-0.2'))
# ── Nerve paths (amber) ──────────────────────────────────────────────────────
# Hypogastric nerves along sacral promontory
nerve_x = [6.8, 6.5, 6.2, 5.9, 5.6]
nerve_y = [12.5, 12.0, 11.3, 10.5, 9.8]
main_ax.plot(nerve_x, nerve_y, color=C['nerve'], lw=3, zorder=9)
main_ax.plot([n+0.3 for n in nerve_x], nerve_y, color=C['nerve'], lw=3, zorder=9)
# Nervi erigentes
for sx, sy in [(7.5, 9.0), (7.5, 8.0), (7.5, 7.0)]:
ex, ey = sx - 2.8, sy - 1.0
main_ax.annotate('', xy=(ex, ey), xytext=(sx, sy),
arrowprops=dict(arrowstyle='->', color=C['nerve'], lw=1.8))
# ═══════════════════════════════════════════════════════════════════════════════
# CALLOUT LABELS (right side)
# ═══════════════════════════════════════════════════════════════════════════════
labels = [
(6.8, 11.0, 12.5, 11.5, 'Hypogastric\nnerves\n(sympathetic L1-L3)', C['nerve']),
(7.5, 8.5, 10.5, 8.5, 'Nervi erigentes\n(S2,S3,S4)', C['nerve']),
(7.5, 6.5, 10.5, 6.5, 'Pelvic (inferior\nhypogastric)\nplexus', C['nerve']),
(7.0, 5.6, 10.5, 5.6, "Waldeyer's\n(rectosacral)\nfascia", '#5C4000'),
]
for lx, ly, tx, ty, txt, col in labels:
main_ax.annotate(txt, xy=(lx, ly), xytext=(tx, ty),
fontsize=8.5, color=col,
arrowprops=dict(arrowstyle='-', color=col, lw=1.3),
bbox=dict(boxstyle='round,pad=0.3', fc='white', ec=col, alpha=0.9))
# Structures labels (left side)
struct_labels = [
(3.5, 11.0, -0.5, 11.5, 'Fascia propria\nof rectum\n(investing fascia)', C['plane_a']),
(3.0, 6.5, -0.5, 6.5, 'Mesorectal\ninvesting\nfascia', '#CC5500'),
]
for lx, ly, tx, ty, txt, col in struct_labels:
main_ax.annotate(txt, xy=(lx, ly), xytext=(tx, ty),
fontsize=8.5, color=col,
arrowprops=dict(arrowstyle='-', color=col, lw=1.3),
bbox=dict(boxstyle='round,pad=0.3', fc='white', ec=col, alpha=0.9))
# Tumor label
main_ax.annotate('TUMOUR', xy=(5.1, 7.5), xytext=(1.0, 7.3),
fontsize=9, color=C['tumor'], fontweight='bold',
arrowprops=dict(arrowstyle='->', color=C['tumor'], lw=1.8),
bbox=dict(boxstyle='round,pad=0.3', fc='#FFE0E0', ec=C['tumor']))
# Main ax title
main_ax.text(5.0, 13.8, 'SAGITTAL VIEW — Male Pelvis',
ha='center', fontsize=13, fontweight='bold', color=C['heading'], zorder=12)
# ═══════════════════════════════════════════════════════════════════════════
# TOP-RIGHT: AXIAL CROSS-SECTION
# ═══════════════════════════════════════════════════════════════════════════
ax_ax = fig.add_axes([0.60, 0.72, 0.38, 0.22])
ax_ax.set_facecolor(C['section_bg'])
ax_ax.set_xlim(-5, 5); ax_ax.set_ylim(-5, 5)
ax_ax.axis('off')
ax_ax.set_aspect('equal')
# Background circle (pelvis wall)
pelvis = plt.Circle((0,0), 4.5, fc='#E8D5B5', ec=C['bone_dark'], lw=2.5)
ax_ax.add_patch(pelvis)
# Parietal pelvic fascia
parietal = plt.Circle((0,0), 3.8, fc='#D4C4A0', ec='#9B7A30', lw=2.5)
ax_ax.add_patch(parietal)
# Mesorectum ring
meso_c = plt.Circle((0,0), 2.6, fc=C['mesrect'], ec='#CC7733', lw=3.0)
ax_ax.add_patch(meso_c)
# Fascia propria ring
fp_c = plt.Circle((0,0), 1.7, fc='#F0C0A0', ec='#CC5500', lw=2.0)
ax_ax.add_patch(fp_c)
# Rectum lumen
rect_c = plt.Circle((0,0), 1.1, fc=C['rectum'], ec=C['rectum_lm'], lw=2.0)
ax_ax.add_patch(rect_c)
# Tumor patch
t_c = plt.Circle((0.5, -0.6), 0.45, fc=C['tumor'], ec='#800000', lw=1.5)
ax_ax.add_patch(t_c)
ax_ax.text(0.5, -0.6, 'T', ha='center', va='center', fontsize=7, fontweight='bold', color='white')
# CRM dashed circle
crm = plt.Circle((0,0), 3.0, fc='none', ec='#CC0000', lw=2.5, ls='--')
ax_ax.add_patch(crm)
# Holy Plane arrow
ax_ax.annotate('', xy=(2.6*np.cos(np.radians(45)), 2.6*np.sin(np.radians(45))),
xytext=(3.5*np.cos(np.radians(45)), 3.5*np.sin(np.radians(45))),
arrowprops=dict(arrowstyle='<->', color=C['plane_p'], lw=2.5))
# Labels
ax_ax.text(0, 0, 'Rectum\nlumen', ha='center', va='center', fontsize=7,
color='white', fontweight='bold')
ax_ax.text(0, 1.35, 'Fascia\npropria', ha='center', va='center', fontsize=6.5, color='#883300')
ax_ax.text(0, 2.15, 'Mesorectum', ha='center', va='center', fontsize=7, color='#884400', fontweight='bold')
ax_ax.text(0, 3.0, 'CRM', ha='center', va='center', fontsize=7.5, color='#CC0000',
fontweight='bold',
bbox=dict(boxstyle='round,pad=0.2', fc='white', ec='#CC0000', alpha=0.9))
ax_ax.text(-4.2, 3.8, 'Pelvic\nwall', ha='center', fontsize=6.5, color=C['text'])
# Holy plane label
ax_ax.text(4.8, 4.5, '"Holy Plane"\nof TME', ha='right', fontsize=8,
color=C['plane_p'], fontweight='bold',
bbox=dict(boxstyle='round,pad=0.3', fc='#E8F0FF', ec=C['plane_p'], alpha=0.95))
ax_ax.annotate('', xy=(2.8, 2.8), xytext=(4.2, 4.0),
arrowprops=dict(arrowstyle='->', color=C['plane_p'], lw=1.8))
ax_ax.set_title('AXIAL VIEW — Mid-Rectum Cross-Section',
fontsize=11, fontweight='bold', color=C['heading'], pad=8)
# ═══════════════════════════════════════════════════════════════════════════
# MID-RIGHT: NERVE ANATOMY PANEL
# ═══════════════════════════════════════════════════════════════════════════
nerve_ax = fig.add_axes([0.60, 0.50, 0.38, 0.20])
nerve_ax.set_facecolor(C['section_bg'])
nerve_ax.set_xlim(0, 10); nerve_ax.set_ylim(0, 6)
nerve_ax.axis('off')
nerve_ax.set_title('AUTONOMIC NERVE ANATOMY (Posterior View)',
fontsize=11, fontweight='bold', color=C['heading'], pad=6)
# IMA and aorta
nerve_ax.plot([5, 5], [6.0, 4.8], color='#CC2222', lw=5, solid_capstyle='round', zorder=3)
nerve_ax.text(5.3, 5.5, 'Aorta / IMA', fontsize=8, color='#CC2222')
# Superior hypogastric plexus
shp = Ellipse((5, 4.3), 2.5, 0.6, fc='#FFE082', ec=C['nerve'], lw=2, zorder=4)
nerve_ax.add_patch(shp)
nerve_ax.text(5, 4.3, 'Superior hypogastric plexus', ha='center', va='center',
fontsize=7.5, fontweight='bold', color='#7B5E00')
# Left and right hypogastric nerves
nerve_ax.plot([4.0, 2.5], [4.0, 2.5], color=C['nerve'], lw=2.5, zorder=4)
nerve_ax.plot([6.0, 7.5], [4.0, 2.5], color=C['nerve'], lw=2.5, zorder=4)
nerve_ax.text(2.0, 2.3, 'L hypogastric\nnerve', fontsize=7.5, ha='center', color=C['nerve'])
nerve_ax.text(8.0, 2.3, 'R hypogastric\nnerve', fontsize=7.5, ha='center', color=C['nerve'])
# Nervi erigentes from sacrum
for sx, col_off in [(2.5, -0.3), (5.0, 0), (7.5, 0.3)]:
nerve_ax.plot([sx + col_off, sx + col_off - 0.5], [0.8, 2.0],
color='#1565C0', lw=2, ls='--', zorder=4)
nerve_ax.text(sx + col_off, 0.5, 'S2-S4', fontsize=7, ha='center', color='#1565C0')
# Inferior hypogastric plexus
ihp_l = Ellipse((2.5, 2.0), 1.8, 0.7, fc='#FFE082', ec=C['nerve'], lw=2, zorder=5)
ihp_r = Ellipse((7.5, 2.0), 1.8, 0.7, fc='#FFE082', ec=C['nerve'], lw=2, zorder=5)
nerve_ax.add_patch(ihp_l)
nerve_ax.add_patch(ihp_r)
nerve_ax.text(2.5, 2.0, 'Pelvic plexus\n(IHP)', ha='center', va='center', fontsize=7, color='#7B5E00')
nerve_ax.text(7.5, 2.0, 'Pelvic plexus\n(IHP)', ha='center', va='center', fontsize=7, color='#7B5E00')
# Rectum schematic
rect_nerve = FancyBboxPatch((3.8, 0.2), 2.4, 3.5, boxstyle="round,pad=0.2",
fc=C['rectum'], ec=C['rectum_lm'], lw=2, alpha=0.6, zorder=3)
nerve_ax.add_patch(rect_nerve)
nerve_ax.text(5.0, 2.0, 'RECTUM', ha='center', va='center', fontsize=8,
fontweight='bold', color='white', zorder=6)
# Legend
nerve_ax.plot([0.2, 0.8], [0.8, 0.8], color=C['nerve'], lw=2.5)
nerve_ax.text(0.9, 0.8, 'Sympathetic', fontsize=7, va='center', color=C['nerve'])
nerve_ax.plot([0.2, 0.8], [0.4, 0.4], color='#1565C0', lw=2.5, ls='--')
nerve_ax.text(0.9, 0.4, 'Parasympathetic', fontsize=7, va='center', color='#1565C0')
# ═══════════════════════════════════════════════════════════════════════════
# BOTTOM PANEL: 3-STEP SEQUENTIAL DISSECTION
# ═══════════════════════════════════════════════════════════════════════════
step_colors = [C['plane_p'], C['plane_a'], C['plane_l']]
step_titles = ['STEP 1: POSTERIOR DISSECTION',
'STEP 2: ANTERIOR DISSECTION',
'STEP 3: LATERAL DISSECTION']
step_texts = [
'Enter presacral space at\nsacral promontory (L5/S1).\nDissect anterior to presacral\nfascia, posterior to fascia\npropria of rectum.\nPreserve hypogastric nerves.\nIncise Waldeyer\'s fascia at\nanorectal junction.',
'Anterior to Denonvilliers\'\nfascia (between rectum and\nprostate / seminal vesicles\nin male; or posterior vaginal\nwall in female).\nProtect membranous urethra\n(palpate urinary catheter).',
'Divide lateral ligaments\n("lateral stalks") bilaterally.\nPreserve pelvic plexuses\n(inferior hypogastric plexus)\non pelvic side wall.\nNervi erigentes at greatest\nrisk here (S2, S3, S4).'
]
step_icons = ['⬇ Posterior', '⬆ Anterior', '↔ Lateral']
for i, (col, title, text, icon) in enumerate(zip(step_colors, step_titles, step_texts, step_icons)):
ax_s = fig.add_axes([0.03 + i*0.325, 0.10, 0.295, 0.20])
ax_s.set_facecolor('#FFFFFF')
for spine in ax_s.spines.values():
spine.set_edgecolor(col); spine.set_linewidth(3)
ax_s.axis('off')
# Header strip
ax_s.add_patch(FancyBboxPatch((0, 0.82), 1, 0.18,
boxstyle="square,pad=0", fc=col, ec=col, transform=ax_s.transAxes))
ax_s.text(0.5, 0.91, title, ha='center', va='center', fontsize=10, fontweight='bold',
color='white', transform=ax_s.transAxes)
# Schematic mini-diagram
ax_s.set_xlim(0, 10); ax_s.set_ylim(0, 10)
# Sacrum (right)
sac = FancyBboxPatch((6.5, 2), 2.5, 7, boxstyle="round,pad=0.2",
fc=C['bone'], ec=C['bone_dark'], lw=1.5)
ax_s.add_patch(sac)
# Rectum
rec = FancyBboxPatch((3.5, 2), 2.0, 7, boxstyle="round,pad=0.3",
fc=C['rectum'], ec=C['rectum_lm'], lw=1.5, alpha=0.85)
ax_s.add_patch(rec)
# Mesorectum
meso_mini = FancyBboxPatch((3.0, 2), 3.0, 7, boxstyle="round,pad=0.2",
fc=C['mesrect'], ec='#CC7733', lw=1.5, alpha=0.7, zorder=1)
ax_s.add_patch(meso_mini)
# Dissection arrow based on step
if i == 0: # posterior
ax_s.annotate('', xy=(6.3, 5.5), xytext=(5.2, 5.5),
arrowprops=dict(arrowstyle='->', color=col, lw=3))
ax_s.text(5.75, 6.2, 'PLANE', ha='center', fontsize=8, color=col, fontweight='bold')
elif i == 1: # anterior
ax_s.add_patch(FancyBboxPatch((1.0, 3), 2.0, 3.5, boxstyle="round,pad=0.2",
fc=C['prostate'], ec='#6a0dad', lw=1.5, alpha=0.8))
ax_s.text(2.0, 4.75, 'Prostate', ha='center', fontsize=7, color='white')
ax_s.annotate('', xy=(3.2, 5.5), xytext=(3.2, 5.5),
arrowprops=dict(arrowstyle='->', color=col, lw=3))
ax_s.plot([3.2, 3.2], [2.5, 8.5], color=col, lw=3, ls='--', dashes=(5,3))
ax_s.text(3.9, 8.8, 'PLANE', ha='center', fontsize=8, color=col, fontweight='bold')
else: # lateral
for xs, xe, ys in [(1.5, 2.9, 5.0), (8.5, 6.1, 5.0)]:
ax_s.annotate('', xy=(xe, ys), xytext=(xs, ys),
arrowprops=dict(arrowstyle='->', color=col, lw=3))
# Text description
ax_s.text(5.0, 1.5, text, ha='center', va='top', fontsize=7.5, color=C['text'],
transform=ax_s.transData,
bbox=dict(boxstyle='round,pad=0.4', fc='#F0F8FF', ec=col, alpha=0.9))
# ═══════════════════════════════════════════════════════════════════════════
# LEGEND BOX
# ═══════════════════════════════════════════════════════════════════════════
leg_ax = fig.add_axes([0.62, 0.10, 0.35, 0.19])
leg_ax.set_facecolor('#FAFAFA')
for spine in leg_ax.spines.values():
spine.set_edgecolor(C['heading']); spine.set_linewidth(2)
leg_ax.axis('off')
leg_ax.text(0.5, 0.95, 'LEGEND', ha='center', va='top', fontsize=11, fontweight='bold',
color=C['heading'], transform=leg_ax.transAxes)
legend_items = [
(C['plane_p'], '--', 'Posterior dissection plane (blue)'),
(C['plane_a'], '--', 'Anterior dissection plane (red)'),
(C['plane_l'], '--', 'Lateral dissection planes (green)'),
(C['nerve'], '-', 'Autonomic nerves (amber) — PRESERVE'),
('#CC7733', '-', 'Mesorectum / mesorectal envelope'),
(C['rectum'], '-', 'Rectum'),
(C['tumor'], '-', 'Tumour'),
('#CC0000', '--', 'Circumferential resection margin (CRM)'),
]
for j, (col, ls, lbl) in enumerate(legend_items):
y = 0.85 - j * 0.11
leg_ax.plot([0.03, 0.12], [y, y], color=col, lw=3 if ls == '-' else 2,
ls=ls, transform=leg_ax.transAxes)
leg_ax.text(0.15, y, lbl, va='center', fontsize=8, color=C['text'],
transform=leg_ax.transAxes)
# ═══════════════════════════════════════════════════════════════════════════
# FOOTER
# ═══════════════════════════════════════════════════════════════════════════
foot_ax = fig.add_axes([0, 0, 1, 0.04])
foot_ax.set_facecolor(C['title_bg'])
foot_ax.axis('off')
foot_ax.text(0.5, 0.55,
'Sources: Bailey & Love\'s Short Practice of Surgery (28e) · Sabiston Textbook of Surgery (21e) · Fischer\'s Mastery of Surgery (8e)',
ha='center', va='center', fontsize=9, color='#B0C4DE')
foot_ax.text(0.5, 0.15,
'TME reduces local recurrence from ~25% → ~6% | 5-year survival improves from ~60% → ~73%',
ha='center', va='center', fontsize=9.5, color='#FFD700', fontweight='bold')
# ═══════════════════════════════════════════════════════════════════════════
# SAVE
# ═══════════════════════════════════════════════════════════════════════════
out = '/home/daytona/workspace/tme-poster/TME_Surgical_Atlas.png'
plt.savefig(out, dpi=180, bbox_inches='tight', facecolor=C['bg'])
print(f"Saved: {out}")
plt.close()
cd /home/daytona/workspace/tme-poster && python tme_atlas.py 2>&1
ls -lh /home/daytona/workspace/tme-poster/TME_Surgical_Atlas.png
TME Surgical Atlas
Image · PNG
- Full male pelvis cross-section showing: sacrum/coccyx, bladder, prostate, seminal vesicles, rectum, mesorectum, anal canal, levator ani
- Color-coded dissection planes drawn in-situ:
- Blue dashed line = posterior plane (between presacral fascia and fascia propria)
- Red dashed line = anterior plane (anterior to Denonvilliers' fascia)
- Green arrows = lateral dissection directions
- Fascial layers labeled: presacral fascia, fascia propria of rectum, Waldeyer's (rectosacral) fascia, Denonvilliers' fascia, peritoneum
- Nerve pathways: hypogastric nerves, nervi erigentes (S2-S4), pelvic plexus
- Concentric ring diagram showing: rectal lumen, fascia propria, mesorectum, CRM (circumferential resection margin in red dashes)
- The "Holy Plane of TME" labeled with arrow
- Posterior view showing the full autonomic nerve map: superior hypogastric plexus → hypogastric nerves → inferior hypogastric (pelvic) plexus + nervi erigentes from S2-S4
- Step 1: Posterior - enter presacral space, incise Waldeyer's fascia
- Step 2: Anterior - Denonvilliers' fascia plane, protect urethra
- Step 3: Lateral - divide lateral stalks, preserve pelvic plexus
- Full color coding guide
- Footer stat: TME reduces local recurrence 25% → 6%, improves 5-year survival 60% → 73%