Temperomandibular joint
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive information to write a thorough response. Let me compile the full answer.
Temporomandibular Joint (TMJ)
Overview
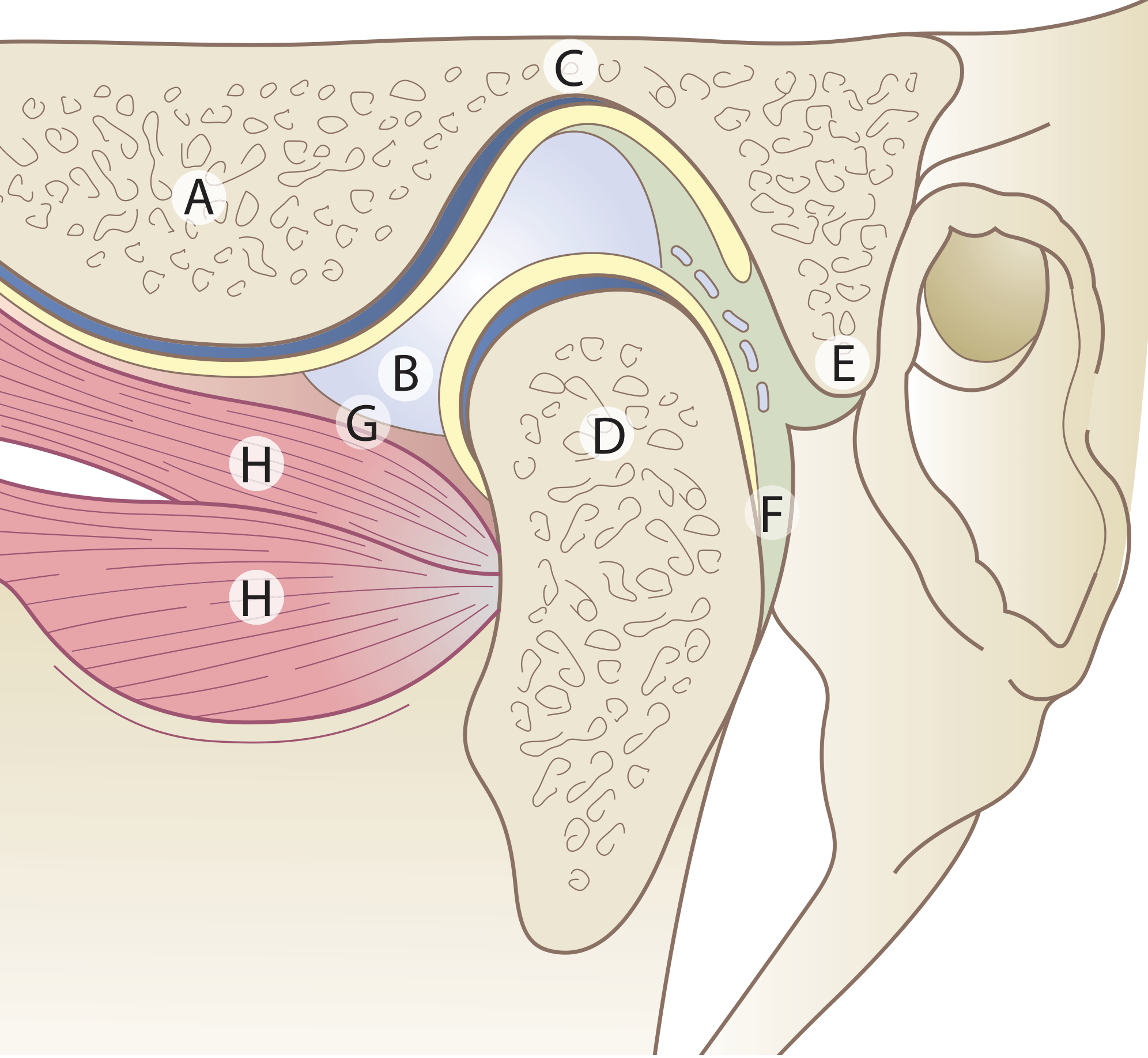
The temporomandibular joint is a synovial joint formed by the articulation of the mandibular condyle with the mandibular (glenoid) fossa of the temporal bone, situated just anterior to the external auditory canal. It is unique among synovial joints in several important respects.
Unique Features
- Divided joint space - An intra-articular fibrocartilaginous disc divides the joint into upper and lower compartments.
- Fibrous articular surfaces - Unlike most synovial joints, the articular surfaces are covered by fibrous tissue, not hyaline cartilage, reflecting the joint's intramembranous developmental origin.
- Secondary condylar cartilage - Present in the head of the condyle until puberty (~16 years), after which it disappears.
- Tooth-influenced movements - Joint biomechanics are directly influenced by dental occlusion.
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, p. 693
Bony Components
- Mandibular condyle: The articular surfaces are the anterior and superior surfaces. The condyle connects to the ramus via the neck of the condyle - a common fracture site. A small pterygoid fovea on the anterior surface of the neck marks the partial attachment of the lateral pterygoid muscle.
- Mandibular (glenoid) fossa of the temporal bone: The fossa does not conform exactly to the condyle shape - partly why the disc is needed to fill the incongruent space.
Joint Capsule
The capsule attaches above to the mandibular fossa (extending anteriorly to just in front of the articular eminence crest, posteriorly to the squamotympanic and petrotympanic fissures) and below to the neck of the condyle. The capsule is relatively slack and weak - it does not significantly limit jaw movements. The inner surface is lined by synovial membrane, which secretes synovial fluid containing proteoglycans. Intra-articular fluid pressure is subatmospheric at rest but rises considerably during mastication.
Articular Disc (Meniscus)
- Dense fibrous consistency, moulded to the bony joint surfaces
- Avascular centrally; blood vessels only at the periphery
- Sagittal section: upper surface is concavo-convex anteroposteriorly; lower surface is concave
- Superior view: rectangular or oval outline
- The self-centring mechanism of the disc maintains its relationship to the condyle during movement
- The central (intermediate) zone is the thinnest region; crimped collagen fibres reflect combined tensional and compressional forces
Disc Attachments
- Anteriorly: fibrous bands to the anterior margin of the articular eminence (above) and the anterior margin of the condyle (below)
- Medially and laterally: attached to the joint capsule and to connective tissue zones at the condylar poles
- Posteriorly: the retrodiscal (bilaminar) tissue - the superior lamina is loose with elastin fibres and vessels (attaches to the squamotympanic fissure); the inferior lamina is relatively avascular and less extensible (attaches to the posterior condyle margin). During jaw opening, venous engorgement increases the retrodiscal tissue volume 4-5 times. Elastic recoil of the superior lamella helps return the disc to its original position.
Movements
The two-compartment arrangement allows two types of movement:
| Compartment | Movement Type |
|---|---|
| Upper (disc-temporal) | Gliding (translation / protrusion) |
| Lower (disc-condyle) | Hinge (rotation) |
During normal mouth opening, the condyle undergoes rotation then translation anteriorly. The joint between the meniscus and condyle is essentially a hinged joint; the joint between the meniscus and temporal bone is a sliding joint. The anteromedial capsule is loose synovial tissue to allow translation.
Normal maximal mouth opening: 3 to 6 cm measured between upper and lower incisor teeth. Lateral movement is assessed using incisor teeth as landmarks.
Muscles of the TMJ
The principal muscle related to disc position is the lateral pterygoid:
- The superior head attaches (in ~60% of individuals) to the joint capsule and medial aspect of the anterior disc border (as well as to the condyle)
- The inferior head is the primary jaw-opening muscle
- Both heads act together with functional heterogeneity; the superior head is also active during opening
Other muscles of mastication (masseter, temporalis, medial pterygoid) act on the mandible and indirectly affect TMJ loading.
Ligaments
| Ligament | Origin | Insertion | Function |
|---|---|---|---|
| Lateral (temporomandibular) ligament | Articular tubercle of articular eminence | Lateral surface and posterior border of condylar neck | Main ligament; limits lateral movement and posterior condyle displacement |
| Sphenomandibular ligament | Spine of sphenoid | Lingula of mandible | Remnant of first branchial arch perichondrium; becomes taut during jaw opening |
| Stylomandibular ligament | Tip of styloid process | Angle of mandible | Reinforced deep cervical fascia; relatively minor role |
| Pterygomandibular raphe | Pterygoid hamulus | Posterior mandible | Accessory; minor function |
| Retinacular ligament (recently described) | Articular eminence | Fascia over masseter at mandibular angle | May maintain blood circulation during mastication |
Innervation and Vasculature
- Innervation: Auriculotemporal, masseteric, and deep temporal branches of the mandibular nerve (V3). Proprioceptive endings are especially important for reflex control of mastication.
- Blood supply: Superficial temporal artery and maxillary artery (anterior tympanic and deep auricular branches), with contributions from deep temporal and transverse facial arteries.
Clinical Conditions
TMJ Disorders (Temporomandibular Disorders - TMD)
TMJ disorders are multifactorial and common. The hallmark features are:
- Pain in the jaw joint or face
- Clicking or popping sounds
- Limited mouth opening (trismus)
Pathophysiology: Like other synovial joints, the TMJ is prone to inflammatory and degenerative arthritis (RA, osteoarthritis). Disc damage increases friction, leading to:
- Disc displacement (usually anteromedial)
- Abnormal loading of the posterior disc
- Vascular invasion, disc perforation
- Bone exposure at articular surfaces
Inflammatory mediators (pro-inflammatory cytokines) accumulate in the synovial fluid. TMJ syndrome is associated with bruxism (teeth grinding) and is considered a form of myofascial pain, akin to fibromyalgia.
Examination: Palpate just anterior to the external auditory canal while the patient opens/closes the mouth and moves laterally. Unilateral or asymmetric synovitis is easier to detect by comparison with the opposite side. Crepitus or clicking can be found in patients with and without severe arthritis.
Disc Internal Derangement
Trauma can tear the meniscus or injure collateral ligaments - causing:
- Clicking/popping as the meniscus fails to translate normally
- Closed lock: inability to open the mouth fully because the disc fails to translate completely
Management: soft diet, avoid wide opening, refer to oral surgeon. Pediatric patients with post-traumatic internal derangements are prone to asymmetric facial growth and retrognathia.
TMJ Dislocation
Anterior dislocation occurs with spontaneous wide mouth opening. Muscle spasm prevents spontaneous reduction.
Clinical features:
- Inability to close the mouth
- Unilateral: jaw rotated away from the affected side
- Bilateral: significant jaw protrusion with drooling and garbled speech
- Depression in the area of the affected TMJ on inspection
Reduction technique: Patient seated upright, operator standing in front. Thumbs/index fingers in the buccal sulcus on either side, press the angle of the jaw downward while rotating the chin upward and backward. Wrap fingers with gauze to protect from bite injury during muscle snap-back. Adequate analgesia and sedation are required.
Arthritis-related
Multiple arthritides affect the TMJ, including juvenile and adult rheumatoid arthritis. In children, arrested mandibular growth leads to micrognathia. - Firestein & Kelley's Textbook of Rheumatology, p. 4608
Imaging
- MRI: Gold standard for soft tissue assessment (disc position, displacement, perforation)
- CT: Best for bony changes, fractures, and surgical planning
- Plain radiograph / Panorex: Used before reduction attempts when fracture-dislocation is suspected
Relation to the Ear
The TMJ is closely related anatomically to the external acoustic meatus. TMJ conditions commonly produce pain that must be distinguished from direct ear pathology - an important clinical consideration in ENT practice.
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, p. 693-694
- Firestein & Kelley's Textbook of Rheumatology, p. 4608-4621
- ROSEN's Emergency Medicine, p. 3522-3524
This is a shared conversation. Sign in to Orris to start your own chat.