Difference between acute liver failure, DCLD and ACLF
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
I now have comprehensive information from the textbooks. Let me compile the full comparison.
Acute Liver Failure (ALF) vs. DCLD vs. ACLF
These three syndromes are distinct but often confused because they all involve severe hepatic dysfunction. The key differentiator is whether underlying chronic liver disease exists and to what degree.
1. Acute Liver Failure (ALF)
Definition: Sudden loss of hepatic function in a person without pre-existing liver disease (or with known but previously stable diseases like Wilson's disease, autoimmune hepatitis, or hepatitis B). Encephalopathy is an essential component of the definition.
- Fulminant hepatic failure: Encephalopathy develops within 8 weeks of symptom onset (e.g., jaundice)
- Subfulminant hepatic failure: Liver disease present for up to 26 weeks before encephalopathy develops
Common Causes (US/Western Europe):
- Acetaminophen toxicity - most common (40%)
- Idiosyncratic drug-induced liver injury (13%)
- Hepatitis B (6%), ischemic hepatitis (6%), autoimmune hepatitis (4%), HAV (4%)
- Wilson's disease (3%), pregnancy-related (2%), Budd-Chiari (2%)
- Indeterminate (17%)
Key Features:
- No prior liver disease (de novo)
- Coagulopathy (elevated INR)
- Hepatic encephalopathy with cerebral edema - this is the hallmark that distinguishes ALF from CLD encephalopathy; cerebral edema does NOT develop in chronic liver disease
- Cerebral edema develops in ~80% with grade 4 encephalopathy; herniation is the most common cause of death (>50% of ALF mortality)
- Multiorgan failure: cerebral edema, hemodynamic instability, coagulopathy, renal failure, sepsis, pulmonary dysfunction, acid-base disturbances
- Rapid progression - must transfer immediately to a liver transplant center
Key Difference from CLD encephalopathy: Lactulose is NOT shown to improve survival in ALF (unlike cirrhotic encephalopathy). Management focuses on reducing intracranial pressure (head elevation, sedation/paralysis, mannitol, hypertonic saline).
- Current Surgical Therapy 14e, p. 460; Harrison's Principles 22E
2. Decompensated Chronic Liver Disease (DCLD) / Decompensated Cirrhosis
Definition: Cirrhosis that has progressed from a compensated to a decompensated state, defined by the appearance of clinical complications of portal hypertension and hepatic dysfunction.
Staging (Sleisenger & Fordtran):
| Stage | Features |
|---|---|
| 1 (Compensated) | No ascites, no varices |
| 2 (Compensated) | Varices present, no bleeding, no ascites |
| 3 (Decompensated) | Ascites ± esophageal varices |
| 4 (Decompensated) | Variceal bleeding ± ascites |
Decompensation is defined by the presence of:
- Ascites
- Variceal hemorrhage
- Hepatic encephalopathy (WITHOUT cerebral edema - key contrast to ALF)
- Jaundice
- Hepatocellular carcinoma (HCC)
Prognosis:
- Compensated cirrhosis: median survival 9-12 years, 5x increased mortality vs. general population
- Decompensated cirrhosis: median survival ~2 years, 10x increased mortality
- Annual rate of decompensation: 4% (HCV), 6-10% (alcohol), 10% (HBV); 58% cumulative probability over 10 years
- Most common causes of death: HCC, sepsis, complications of portal hypertension
Key Features:
- Chronic, slow deterioration over years
- Encephalopathy triggered by precipitants (GI bleeding, infection, hyponatremia, dehydration, constipation)
- No cerebral edema
- Management with lactulose, rifaximin, diuretics, beta-blockers for varices, SBP prophylaxis
- MELD score guides transplant listing
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease; Harrison's Principles 22E
3. Acute-on-Chronic Liver Failure (ACLF)
Definition: A condition in patients with underlying chronic liver disease (with or without cirrhosis) in which a precipitating event triggers hepatic and extrahepatic multiorgan failure with high short-term mortality.
Working definition: "A condition associated with mortality within 3 months in the absence of treatment of the underlying liver disease, liver support, or liver transplantation."
Three Types (based on underlying disease):
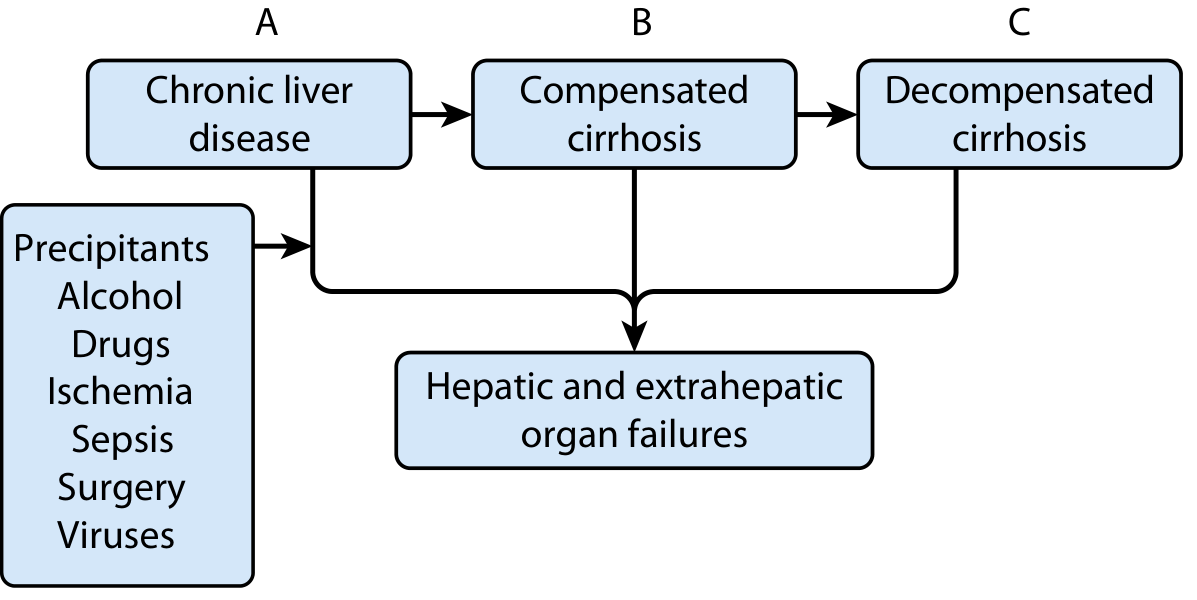
| Type | Underlying Disease |
|---|---|
| A | Chronic liver disease without cirrhosis |
| B | Compensated cirrhosis |
| C | Decompensated cirrhosis |
Precipitating Events:
- Eastern countries: HBV reactivation, HEV superinfection, alcohol-associated hepatitis
- Western countries: Alcohol-associated hepatitis, bacterial infections
- Others: drugs, ischemia, sepsis, surgery, viruses
Organ Failures in ACLF (TABLE 74.2):
| Organ | Manifestation |
|---|---|
| Brain | Hepatic encephalopathy grade 3-4 |
| Kidneys | Type 1 HRS or need for renal replacement therapy |
| Circulatory | Need for vasopressor support |
| Lungs | ARDS requiring ventilatory support |
| Liver | Hypoglycemia, lactic acidosis, hyperammonemia, coagulopathy |
| Adrenal | Hypotension |
| Bone marrow | Suppression |
Prognosis by number of organ failures:
- 2 organ failures: 27% in-hospital mortality
- 3 organ failures: 65% mortality
- 4 organ failures: 97% mortality
Clinical features: Systemic inflammatory response syndrome - fever, tachycardia, tachypnea, leukocytosis.
Management:
- Treat precipitating event (glucocorticoids for alcohol-associated hepatitis, antivirals for HBV)
- Aggressive organ support
- Liver transplantation (often the only definitive therapy)
- Multidisciplinary critical care team
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease; Tietz Textbook of Laboratory Medicine 7E; Harrison's Principles 22E
Summary Comparison Table
| Feature | ALF | DCLD | ACLF |
|---|---|---|---|
| Prior liver disease | Absent (or previously stable) | Yes - long-standing cirrhosis | Yes - chronic liver disease ± cirrhosis |
| Onset | Acute (days to weeks) | Chronic, gradual | Acute deterioration on chronic background |
| Encephalopathy | Present (required for diagnosis) | May be present (precipitant-driven) | Present (grade 3-4 = organ failure) |
| Cerebral edema | Yes - characteristic | No | Rare |
| Multiorgan failure | Yes | No (single-organ complications) | Yes - defining feature |
| Systemic inflammation | Variable | Mild/absent | Prominent (SIRS) |
| Mortality | High (without transplant) | 50% at 2 years | Very high short-term (27-97% by organ failure count) |
| Main cause of death | Cerebral herniation | HCC, sepsis, portal HTN complications | Multiorgan failure |
| Reversibility | Yes if etiology treated early | Partial (treat underlying disease) | Low once 3+ organ failures |
| Liver transplant | Often needed | Listed by MELD | Urgent indication |
| Lactulose | NOT effective | Effective | Supportive only |
| Key biomarker/score | INR, factor V | MELD, Child-Pugh | CLIF-C ACLF score, NACSELD-ACLF |
Practical Mnemonic:
- ALF = Liver failure appearing from nowhere (no prior disease) - acute, explosive
- DCLD = Liver failing slowly under the weight of chronic disease - gradual, progressive
- ACLF = Chronic disease pushed over the edge by an acute insult - acute-on-chronic, multiorgan, systemic inflammation
This is a shared conversation. Sign in to Orris to start your own chat.