Liver chirossis in detail
Reading File
Finding Sources
Finding Sources
Searching PubMed
"liver cirrhosis"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
I now have comprehensive, well-illustrated information from multiple major textbooks. Let me compose the full detailed answer.
Liver Cirrhosis - Comprehensive Overview
Definition
Cirrhosis is the diffuse transformation of the liver into regenerative parenchymal nodules surrounded by fibrous bands, representing the final common pathway for a wide variety of chronic liver diseases. It is not a single specific diagnosis - the morphology, pathophysiology, and prognosis can differ depending on the underlying cause. Importantly, not all chronic liver disease terminates in cirrhosis, and not all cirrhosis leads to end-stage liver disease.
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease, p. 1163
- Robbins & Kumar Basic Pathology, p. 598
Gross and Histological Appearance

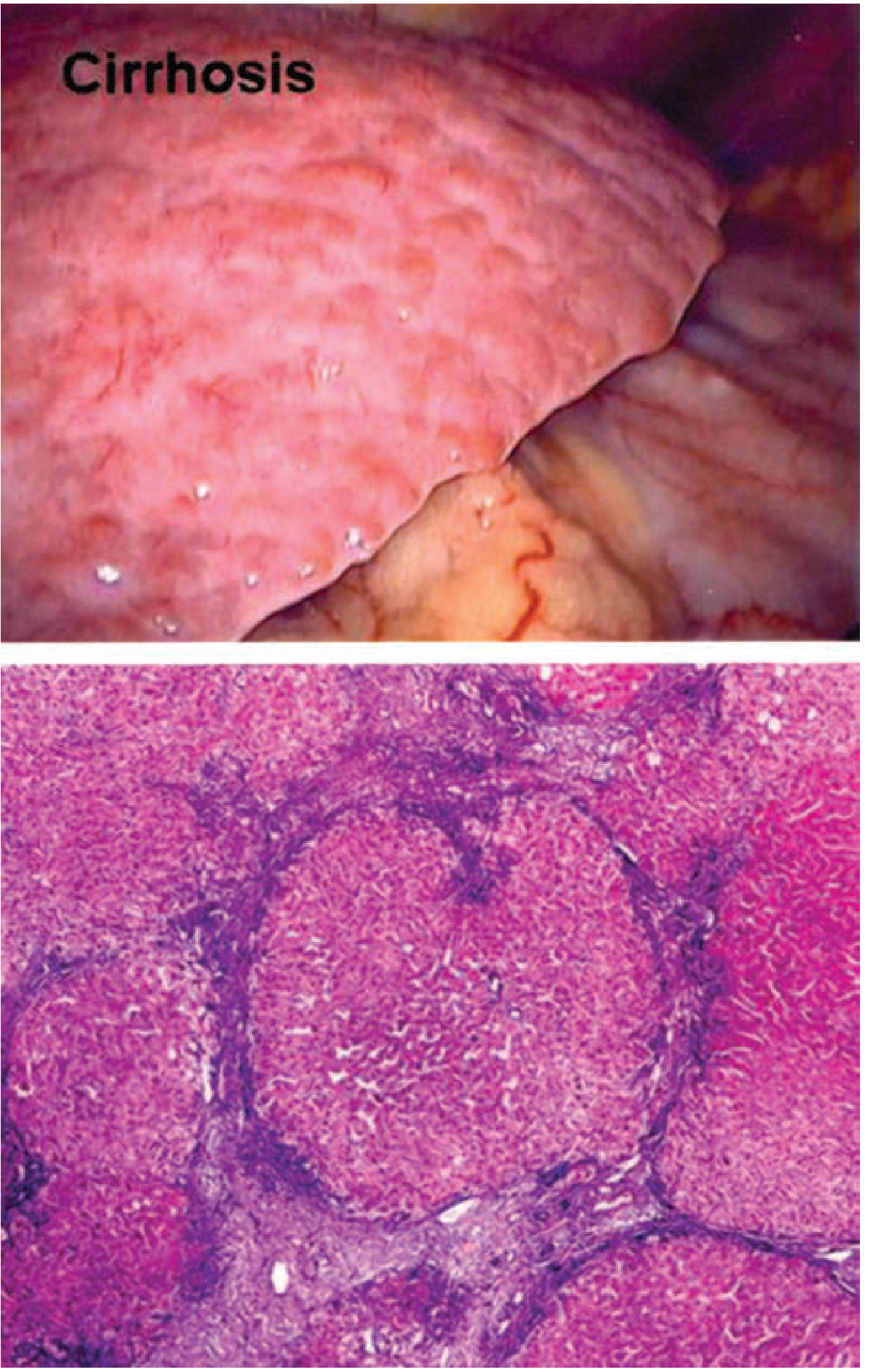
Gross: The liver surface shows a nodular texture, can be small or enlarged depending on etiology and stage, with varying patterns of nodularity:
- Micronodular (<3 mm): typical of alcohol-related cirrhosis
- Macronodular (>3 mm): typical of post-viral cirrhosis
- Mixed pattern can occur with alcohol cessation
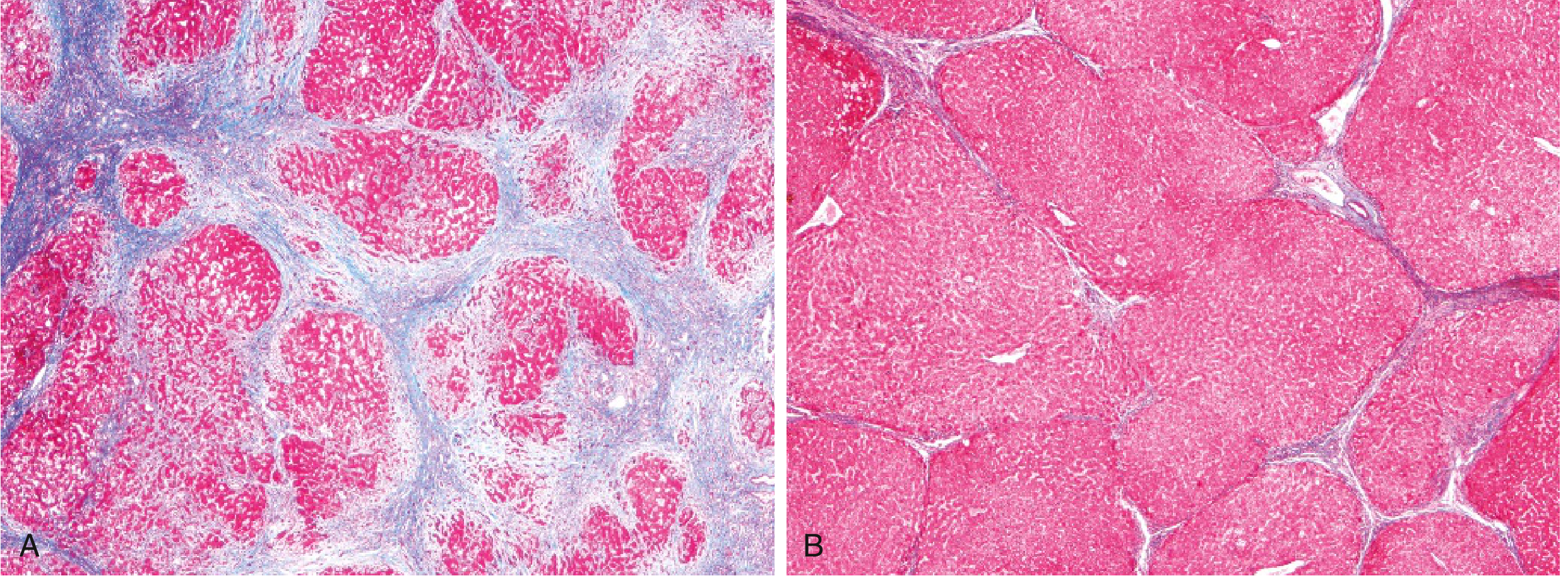
Microscopic: Regenerative parenchymal nodules surrounded by fibrous bands (portal-to-portal or portal-to-central bridging fibrosis). Ductular reactions (stem cell-derived duct-like structures) increase with disease progression and are most prominent in cirrhosis.
- Robbins & Kumar Basic Pathology, p. 598
Etiology
Common Causes
| Category | Examples |
|---|---|
| Alcohol | Alcohol-associated liver disease (most common in USA/Europe) |
| Viral hepatitis | Chronic Hepatitis B, Chronic Hepatitis C |
| Metabolic | Metabolic dysfunction-associated steatotic liver disease (MASLD/MASH) |
| Biliary | Primary biliary cholangitis (PBC), Primary sclerosing cholangitis (PSC), Autoimmune cholangiopathy |
| Autoimmune | Autoimmune hepatitis |
| Inherited metabolic | Hemochromatosis, Wilson's disease, Alpha-1 antitrypsin deficiency, Cystic fibrosis |
| Cardiac | Cardiac cirrhosis (chronic right heart failure) |
| Drug-induced | High-dose vitamin A, methotrexate |
| Cryptogenic | No identifiable cause |
- Harrison's Principles of Internal Medicine 22E, p. (Table 355-1)
Alcohol accounts for the most common etiology in Western countries. Over 14 million adults in the US meet criteria for alcohol use disorder. Chronic alcohol use can produce fibrosis even without inflammation, and the pattern may be centrilobular, pericellular, or periportal.
Pathogenesis
The Central Role of Hepatic Stellate Cells
The key cellular player in liver fibrosis is the hepatic stellate cell (HSC). In the normal liver, HSCs are pericytes residing in the space of Disse, abluminal to sinusoidal endothelial cells. Upon activation (by injury, inflammation, or paracrine signaling), HSCs transform into myofibroblasts, characterized by:
- Upregulation of smooth muscle actin
- Increased motility and contractility
- Production of extracellular matrix (initially fibronectin, then collagen type 1)
The matrix deposition causes further HSC activation and disrupts the normal hepatic angioarchitecture, creating a self-amplifying cycle.
Key signaling pathways driving HSC activation:
- Platelet-derived growth factor (PDGF) - kinase pathway
- Transforming growth factor-beta (TGF-β)
- Integrin signaling pathways
Other cells involved:
- Portal fibroblasts - implicated in biliary/cholestatic forms of fibrosis (PBC, PSC)
- Macrophages (Kupffer cells) - release inflammatory cytokines that transactivate HSCs; some subsets promote fibrosis, others aid resolution
- Sinusoidal endothelial cells - paracrine role in stellate cell activation
- Epithelial cells - injury (apoptosis, sterile necrosis, inflammation) is the initiating step
Fibrosis regression is possible: with disease remission/cure, myofibroblasts can undergo deactivation, apoptosis, or senescence. Matrix proteases break down fibrous septa and nodules coalesce. Even established cirrhosis can regress - shown dramatically in alcohol-related cirrhosis after abstinence (see histology above).
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease, p. 1164
Clinical Features
Compensated vs. Decompensated Cirrhosis
About 40% of patients are asymptomatic until advanced disease. Clinicians must distinguish:
| Stage | Description |
|---|---|
| Stage 1 (Compensated) | No ascites, no varices |
| Stage 2 (Compensated) | Varices present, no bleeding, no ascites |
| Stage 3 (Decompensated) | Ascites ± esophageal varices |
| Stage 4 (Decompensated) | Variceal bleeding ± ascites |
Development of ascites, hepatic encephalopathy, or variceal bleeding = decompensated cirrhosis → consider liver transplant evaluation.
Symptoms and Signs
General:
- Anorexia, weight loss, weakness, fatigue
- Jaundice (chronic severe jaundice → pruritus, sometimes severe)
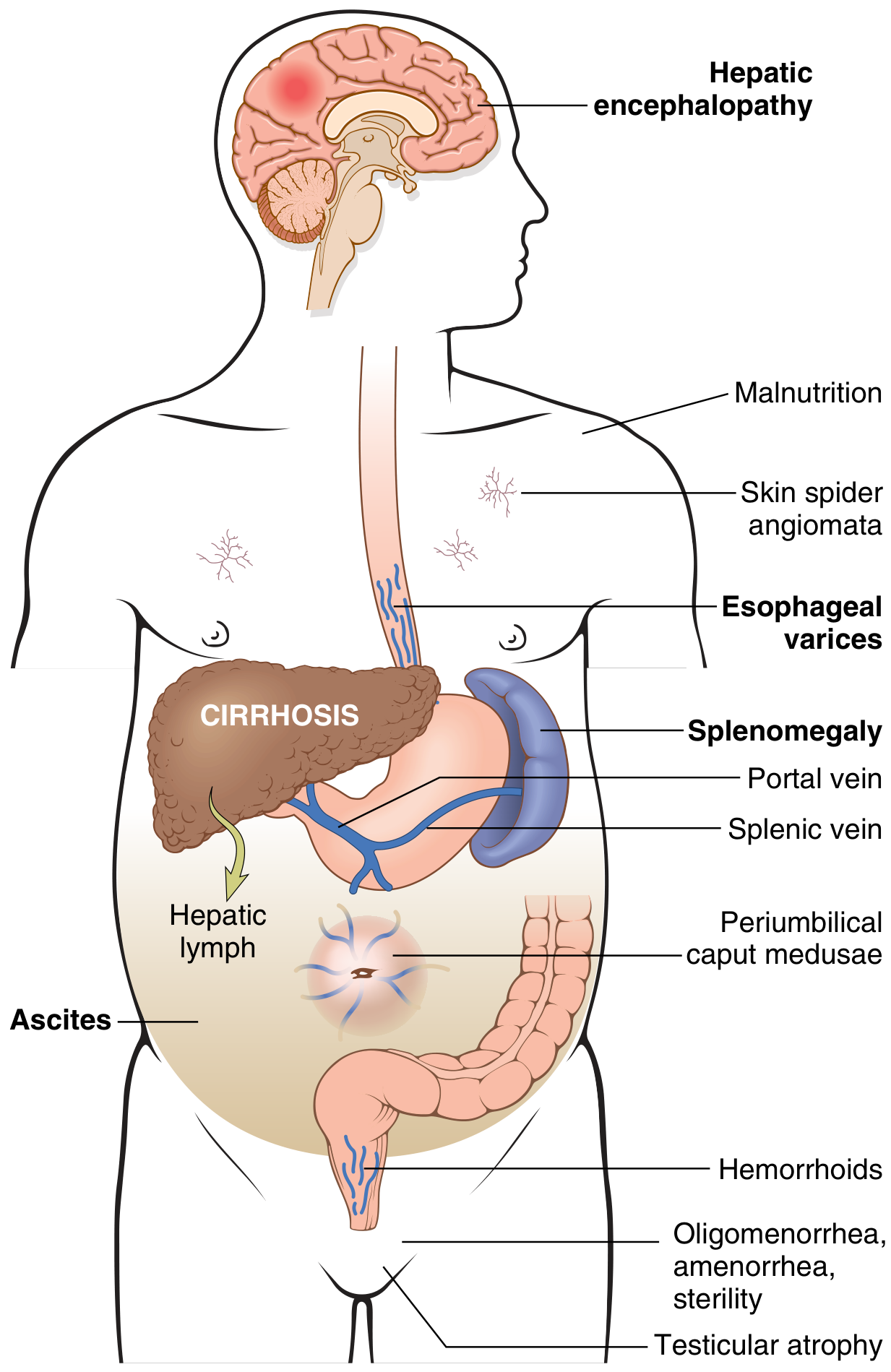
Signs of portal hypertension:
- Ascites (85% of ascites is caused by portal hypertension from cirrhosis)
- Esophageal/gastric varices (~40% of advanced cases, risk of fatal hematemesis)
- Caput medusae (dilated periumbilical veins)
- Hemorrhoids
- Splenomegaly → hypersplenism (thrombocytopenia, pancytopenia)
Signs of impaired synthetic function:
- Hypoalbuminemia → edema
- Coagulopathy (prolonged PT/INR)
- Jaundice
Signs of hyperestrogenemia (male patients - impaired estrogen metabolism):
- Palmar erythema
- Spider angiomas (on trunk and upper limbs)
- Gynecomastia
- Hypogonadism, testicular atrophy
Female patients: Oligomenorrhea, amenorrhea, sterility
- Robbins & Kumar Basic Pathology, p. 598-599
Complications
Portal Hypertension-Related
- Ascites - transudate (protein <3 g/dL), serum-to-ascites albumin gradient (SAAG) ≥1.1 g/dL
- Variceal hemorrhage - esophagogastric varices in ~40% of advanced liver disease; potentially fatal
- Hepatic hydrothorax
- Spontaneous bacterial peritonitis (SBP)
Hepatic Dysfunction
- Hepatic encephalopathy - portosystemic shunting of ammonia and other toxins
- Coagulopathy - impaired clotting factor synthesis
- Hepatorenal syndrome (HRS) - functional renal failure in decompensated cirrhosis
Cardiopulmonary
- Hepatopulmonary syndrome - intrapulmonary vascular dilation → hypoxemia
- Portopulmonary hypertension
- Cirrhotic cardiomyopathy
Metabolic and Endocrine
- Adrenal insufficiency
- Hypogonadism
- Malnutrition / sarcopenia
- Osteoporosis
Hematologic
- Thrombocytopenia (hypersplenism)
- Anemia
- Venous thrombosis (paradoxically increased due to impaired anticoagulant synthesis)
Oncologic
-
Hepatocellular carcinoma (HCC) - most chronic liver diseases predispose; cirrhosis is the strongest risk factor for HCC worldwide
-
Cholangiocarcinoma
-
Sleisenger and Fordtran's Gastrointestinal and Liver Disease, pp. 1164-1167
Diagnosis
Laboratory Tests
- Liver enzymes: AST, ALT elevated (AST:ALT >2:1 in alcohol-related disease)
- Synthetic function: Low albumin, prolonged PT/INR
- Bilirubin: Elevated in decompensated disease
- CBC: Thrombocytopenia (platelet <160,000/mm³ supports diagnosis; ≥160,000 argues against)
- APRI score (AST/platelet ratio index): >2 suggests cirrhosis
Non-Invasive Fibrosis Assessment
- Serum-based scores: FIB-4, APRI, Bonacini score, Lok index
- Transient elastography (Fibroscan):
-
14 kPa → suggests cirrhosis
-
19.5 kPa → esophageal varices unlikely if below this
-
21 kPa → portal hypertension with complications
-
- ARFI elastography: >2.6 m/sec → cirrhosis
- MR elastography (MRE): >5.9 kPa → cirrhosis (liver biopsy usually not needed to confirm)
- Increasing spleen stiffness on elastography is associated with portal hypertension onset
Imaging
- Ultrasound: Small nodular liver + splenomegaly + collaterals + ascites
- CT/MRI: Cross-sectional imaging for detailed assessment and HCC screening
Liver Biopsy
The gold standard for staging (F0-F4 on Metavir or equivalent):
- Stage 3 = bridging fibrosis with nodularity
- Stage 4 = cirrhosis
Biopsy is typically not required if non-invasive tests confirm cirrhosis.
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease, pp. 1164-1167
Prognosis Scoring
Child-Pugh Score
Assesses 5 parameters (encephalopathy, ascites, bilirubin, albumin, PT):
- Class A (5-6 points): Well-compensated, 1-year survival ~100%
- Class B (7-9 points): Significant impairment
- Class C (10-15 points): Decompensated, 1-year survival ~45%
MELD Score (Model for End-Stage Liver Disease)
MELD = 3.78 × ln(bilirubin) + 11.2 × ln(INR) + 9.57 × ln(creatinine) + 6.43
- MELD ≥15 → consider liver transplant listing
- Higher MELD = higher 90-day mortality
- Used for organ allocation priority by UNOS
Key prognostic points:
-
Compensated cirrhosis: 5x increased risk of death vs. general population
-
Decompensated cirrhosis: 10x increased risk
-
Chronic liver disease is the 12th leading disease cause of death in the USA; in ages 45-64, it is the 3rd leading cause of death
-
In compensated stages, the most common cause of death is cardiovascular disease, not liver failure
-
In decompensated cirrhosis, death is usually due to complications of portal hypertension, HCC, or sepsis
-
Sleisenger and Fordtran's Gastrointestinal and Liver Disease, pp. 1167-1169
Management
General Measures
- Treat the underlying cause (most important):
- Abstinence from alcohol
- Antiviral therapy for HBV (tenofovir, entecavir) and HCV (direct-acting antivirals - >95% cure rate)
- Ursodeoxycholic acid for PBC
- Immunosuppression for autoimmune hepatitis
- Phlebotomy/chelation for hemochromatosis
- Avoid hepatotoxins: NSAIDs, nephrotoxic agents, sedatives
- Vaccinate: Hepatitis A, Hepatitis B, pneumococcal, influenza
- Nutrition: High-calorie, protein-adequate diet (1.2-1.5 g/kg/day protein); treat sarcopenia
Management of Specific Complications
Ascites:
- Sodium restriction (<2 g/day)
- Diuretics: spironolactone (first-line) ± furosemide
- Large-volume paracentesis + albumin infusion for refractory ascites
- TIPS (transjugular intrahepatic portosystemic shunt) for refractory cases
Esophageal Varices:
- Primary prophylaxis: non-selective beta-blockers (propranolol, nadolol, carvedilol)
- Endoscopic variceal band ligation (EVL)
- Active bleed: octreotide/terlipressin + EVL ± TIPS
Hepatic Encephalopathy:
- Lactulose (reduces ammonia absorption)
- Rifaximin (non-absorbable antibiotic, reduces gut ammonia-producing bacteria)
- Identify and treat precipitants (infection, GI bleed, constipation, medications)
Spontaneous Bacterial Peritonitis (SBP):
- Third-generation cephalosporins (cefotaxime)
- Long-term norfloxacin prophylaxis in high-risk patients
Hepatorenal Syndrome:
- Discontinue diuretics, nephrotoxins
- IV albumin + vasoconstrictors (terlipressin or norepinephrine + albumin)
- TIPS as bridge to transplantation
HCC Surveillance:
- Ultrasound ± AFP every 6 months in all cirrhotic patients
Reversal of Fibrosis
Regression of fibrosis - and even of fully established cirrhosis - can occur after disease remission. Scars become thinner, fragment, and adjacent nodules coalesce. This is best demonstrated in:
- Hepatitis C: fibrosis regression after sustained virologic response (SVR)
- Alcohol: significant regression after prolonged abstinence
- Autoimmune hepatitis: regression with immunosuppression
Liver Transplantation
- Definitive treatment for end-stage cirrhosis
- Indications: MELD ≥15, decompensated cirrhosis refractory to treatment, HCC within Milan criteria
- 5-year survival post-transplant: ~70-80%
- Patients with ACLF listed for transplant have high risk of delisting or death (~50% within 6 months if not transplanted)
Acute-on-Chronic Liver Failure (ACLF)
A distinct, severe syndrome occurring in patients with underlying chronic liver disease:
- Definition: Chronic liver disease ± cirrhosis + acute decompensation + hepatic and extrahepatic organ failure + high short-term mortality (within 3 months without specific treatment)
- Precipitants (West): Bacterial infection (most common), alcohol-associated hepatitis
- Precipitants (East): HBV reactivation, HEV superinfection, alcohol
- Pathophysiology: Gut microbiome dysbiosis → bacterial translocation → systemic inflammation → multiorgan failure
- Mortality: ~50% in-hospital; higher than acute liver failure after 1 week
ACLF types:
-
Type A: Underlying chronic liver disease without cirrhosis
-
Type B: Underlying compensated cirrhosis
-
Type C: Underlying decompensated cirrhosis
-
Sleisenger and Fordtran's Gastrointestinal and Liver Disease, pp. 1170-1171
Summary Table
| Feature | Compensated | Decompensated |
|---|---|---|
| Ascites | Absent | Present |
| Varices | May be present, no bleed | Bleeding varices |
| Encephalopathy | Absent | Present |
| Jaundice | Mild or absent | Prominent |
| 1-yr mortality | Low | High (~10-fold increased) |
| Main cause of death | Cardiovascular disease | Portal hypertension complications, HCC, sepsis |
Sources:
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease (Chapter 74)
- Robbins & Kumar Basic Pathology (Chapter 14)
- Harrison's Principles of Internal Medicine, 22nd Ed. (Chapter 355)
Recent evidence note: A 2025 systematic review (PMID 40588713) addresses the hepatic fibrosis-to-HCC axis with emerging therapeutic targets. Research in sarcopenia and MASLD-related cirrhosis is also active (PMID 39214253). No major shifts in core cirrhosis management guidelines have been identified in recent meta-analyses.
Classification
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
Reading File
I now have everything needed for a thorough classification answer. Here it is:
Classification of Liver Cirrhosis
Cirrhosis is classified under four main frameworks: morphological, etiological, clinical/functional (compensated vs. decompensated), and prognostic scoring systems.
1. Morphological Classification (WHO, 1977)
Based on the size of regenerative nodules on gross and histological examination:
| Type | Nodule Size | Characteristics | Typical Etiology |
|---|---|---|---|
| Micronodular | <3 mm | Thick regular septa; small uniform nodules; involves virtually every lobule | Alcohol, biliary obstruction, hemochromatosis |
| Macronodular | >3 mm | Septa and nodules of varying sizes; hepatocytes with large nuclei; cell plates of varying thickness | Viral hepatitis (HBV, HCV), autoimmune hepatitis |
| Mixed | Both | Micronodular liver with foci of macronodular regeneration; a transitional state | Alcohol with cessation (micro → macro conversion) |
Important caveat: The WHO morphological classification has low specificity - the same pattern can result from different diseases, and a single disease can show several patterns. Nodule size changes over time (dynamic process). This system is therefore considered to have little utility in defining etiology and has largely been replaced by etiological classification.
- Schwartz's Principles of Surgery, 11th Ed., p. 1390
- Mulholland and Greenfield's Surgery, 7th Ed., p. 2858
2. Etiological Classification
The most clinically useful classification. Identifying the cause drives treatment decisions.
A. Alcohol-Related
- Most common cause in Western countries (accounts for ~30% of liver transplants in USA)
- Classically produces micronodular cirrhosis
- Minimum threshold: >30 g/day (women), >50 g/day (men) for ≥5 years
- Histology: steatosis → alcoholic steatohepatitis → fibrosis → cirrhosis; Mallory-Denk bodies; megamitochondria
B. Viral Hepatitis
- Chronic Hepatitis B - can cause cirrhosis with or without prior hepatitis
- Chronic Hepatitis C - one of the leading causes worldwide; SVR with direct-acting antivirals can halt and reverse fibrosis
- Hepatitis D - superinfection on HBV accelerates cirrhosis
- Typically produces macronodular pattern
C. Metabolic / Steatotic Liver Disease
- MASLD/MASH (formerly NAFLD/NASH) - now the most common chronic liver disease worldwide; ~1 in 10 NASH patients progress to cirrhosis
- Hemochromatosis - iron overload → hepatocyte injury
- Wilson's disease - copper accumulation
- Alpha-1 antitrypsin deficiency - misfolded protein accumulation in hepatocytes
- Cystic fibrosis - biliary involvement
- Glycogen storage diseases (types IA, III, IV), Tyrosinemia, Galactosemia
D. Biliary / Cholestatic
- Primary Biliary Cholangitis (PBC) - autoimmune destruction of small intrahepatic bile ducts; antimitochondrial antibodies in 95%; progresses from non-suppurative cholangitis → bridging fibrosis → cirrhosis
- Primary Sclerosing Cholangitis (PSC) - inflammation and fibrosis of intra- and extrahepatic ducts; associated with IBD
- Autoimmune cholangiopathy
- Biliary obstruction (secondary biliary cirrhosis)
E. Autoimmune
- Autoimmune hepatitis - responds to immunosuppression; cirrhosis may regress with treatment
F. Vascular / Cardiac
- Cardiac cirrhosis - chronic right heart failure → centrilobular congestion → "nutmeg liver" → fibrosis
- Budd-Chiari syndrome - hepatic vein outflow obstruction
G. Drugs and Toxins
- High-dose vitamin A (chronic)
- Methotrexate (cumulative dose)
- Amiodarone, isoniazid, and others
H. Cryptogenic
-
No identifiable cause after full workup; may represent unrecognized MASLD or burnt-out autoimmune hepatitis
-
Schwartz's Principles of Surgery, p. 1390 (Table 31-3)
-
Harrison's Principles of Internal Medicine, 22nd Ed.
3. Clinical / Functional Classification
Compensated vs. Decompensated
The most important clinical distinction, as it directly governs prognosis and management:
| Feature | Compensated | Decompensated |
|---|---|---|
| Ascites | Absent | Present |
| Variceal bleeding | Absent | Present |
| Hepatic encephalopathy | Absent | Present |
| Jaundice | Minimal/absent | Significant |
| 5-year survival | ~80% | ~35% |
Four-Stage Model (Baveno / D'Amico Staging)
| Stage | Description | Median survival |
|---|---|---|
| Stage 1 | Compensated; no varices, no ascites | >12 years |
| Stage 2 | Compensated; varices present, no bleeding, no ascites | >12 years (but higher risk) |
| Stage 3 | Decompensated; ascites ± varices | ~2 years |
| Stage 4 | Decompensated; variceal bleeding ± ascites | ~1 year |
Stages 1-2 = compensated; stages 3-4 = decompensated.
Portal Hypertension Sub-staging (Current Guidelines)
Current guidelines further sub-stage compensated cirrhosis by the Hepatic Vein Pressure Gradient (HVPG):
| Sub-stage | HVPG | Definition | Significance |
|---|---|---|---|
| Mild portal hypertension | 6-9 mmHg | Below threshold for CSPH | Lower risk of varices |
| Clinically Significant Portal Hypertension (CSPH) | ≥10 mmHg | Predicts variceal formation and decompensation | Mandates variceal screening |
| Severe portal hypertension | ≥12 mmHg | Threshold for variceal bleeding | Active intervention required |
If HVPG is unavailable, CSPH is inferred from: liver stiffness >20-25 kPa plus low platelets, splenomegaly, or portosystemic collaterals on imaging.
- Mulholland and Greenfield's Surgery, 7th Ed., p. 2894
4. Prognostic Scoring Classification
A. Child-Pugh Score
Developed to stratify operative risk for portal decompressive surgery. Scores 5 clinical/lab parameters (1-3 points each):
| Parameter | 1 Point | 2 Points | 3 Points |
|---|---|---|---|
| Encephalopathy | None | Grade 1-2 | Grade 3-4 |
| Ascites | None | Slight | Moderate-severe |
| Albumin (g/dL) | >3.5 | 2.8-3.5 | <2.8 |
| Bilirubin (mg/dL) | <2.0 | 2.0-3.0 | >3.0 |
| PT prolonged (sec) / INR | <4 / <1.7 | 4-6 / 1.7-2.3 | >6 / >2.3 |
Total score → Class:
| Class | Score | Interpretation | 1-year survival |
|---|---|---|---|
| A | 5-6 | Well-compensated | ~100% |
| B | 7-9 | Significant impairment | ~80% |
| C | 10-15 | Decompensated / end-stage | ~45% |
- Class B (score ≥7) = accepted minimum for liver transplant listing (historical criterion)
- Limitations: subjective parameters (ascites, encephalopathy grading), ceiling effect, less center-to-center consistency
B. MELD Score (Model for End-Stage Liver Disease)
Fully objective; now used globally for transplant waitlist prioritization. Uses 3 lab values:
$$\text{MELD} = 3.78 \times \ln[\text{bilirubin (mg/dL)}] + 11.2 \times \ln[\text{INR}] + 9.57 \times \ln[\text{creatinine (mg/dL)}] + 6.43$$
(If hemodialysis × 2 within 1 week, creatinine is set to 4.0 mg/dL)
| MELD Score | 3-month Mortality Risk | Action |
|---|---|---|
| <10 | Low | Monitor |
| 10-20 | Intermediate | Close follow-up |
| >20 | High | Transplant evaluation urgent |
| ≥15 | - | Standard threshold for listing |
MELD-Na: Adds serum sodium to improve accuracy (hyponatremia is an independent predictor of mortality in cirrhosis).
PELD (Pediatric End-Stage Liver Disease): Used for children <12 years old.
Advantages over Child-Pugh:
-
All objective variables
-
Wider scoring range
-
Better predicts short-term survival
-
Superior for predicting post-TIPS outcomes
-
Harrison's Principles of Internal Medicine, 22nd Ed., p. (Table 347-6)
-
Tietz Textbook of Laboratory Medicine, 7th Ed., p. (Table 51.9)
Summary Diagram
LIVER CIRRHOSIS CLASSIFICATION
│
├── 1. MORPHOLOGICAL (WHO 1977 - limited utility)
│ ├── Micronodular (<3mm) → Alcohol, hemochromatosis
│ ├── Macronodular (>3mm) → Viral hepatitis, autoimmune
│ └── Mixed → Transitional state
│
├── 2. ETIOLOGICAL (most clinically useful)
│ ├── Alcohol-related
│ ├── Viral (HBV, HCV, HDV)
│ ├── Metabolic (MASLD, hemochromatosis, Wilson's, A1AT)
│ ├── Biliary (PBC, PSC)
│ ├── Autoimmune hepatitis
│ ├── Vascular (cardiac, Budd-Chiari)
│ ├── Drug/toxin-induced
│ └── Cryptogenic
│
├── 3. CLINICAL (prognostic staging)
│ ├── Compensated (Stage 1-2)
│ │ ├── Without CSPH (HVPG <10)
│ │ └── With CSPH (HVPG ≥10)
│ └── Decompensated (Stage 3-4)
│ ├── Ascites
│ ├── Variceal hemorrhage
│ └── Encephalopathy
│
└── 4. PROGNOSTIC SCORES
├── Child-Pugh (Class A/B/C) → surgical risk, historical transplant criterion
├── MELD (0-40+) → transplant listing, short-term mortality
├── MELD-Na → adds sodium for accuracy
└── PELD → pediatric patients (<12 yrs)
This is a shared conversation. Sign in to Orris to start your own chat.