Respiratory disease which causes less ciliary function
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a complete overview of Primary Ciliary Dyskinesia (PCD) - the respiratory disease caused by reduced/absent ciliary function - drawn from authoritative textbooks.
Primary Ciliary Dyskinesia (PCD)
Also known as: Immotile Cilia Syndrome | Kartagener Syndrome (when combined with situs inversus)
Definition & Genetics
PCD is a group of autosomal recessive hereditary disorders affecting approximately 1 in 10,000-20,000 live-born children. It is caused by mutations in genes encoding dynein proteins (components of cilia) or cytoplasmic proteins responsible for cilia assembly. Because many different genes can be affected, PCD is genetically heterogeneous - over 40 causative genes have been identified.
- Histology: A Text and Atlas, p. 350
- Murray & Nadel's Textbook of Respiratory Medicine
The Ciliary Defect
Normal cilia have a 9+2 microtubule arrangement with inner and outer dynein arms that power movement. In PCD, structural defects prevent normal ciliary beating:
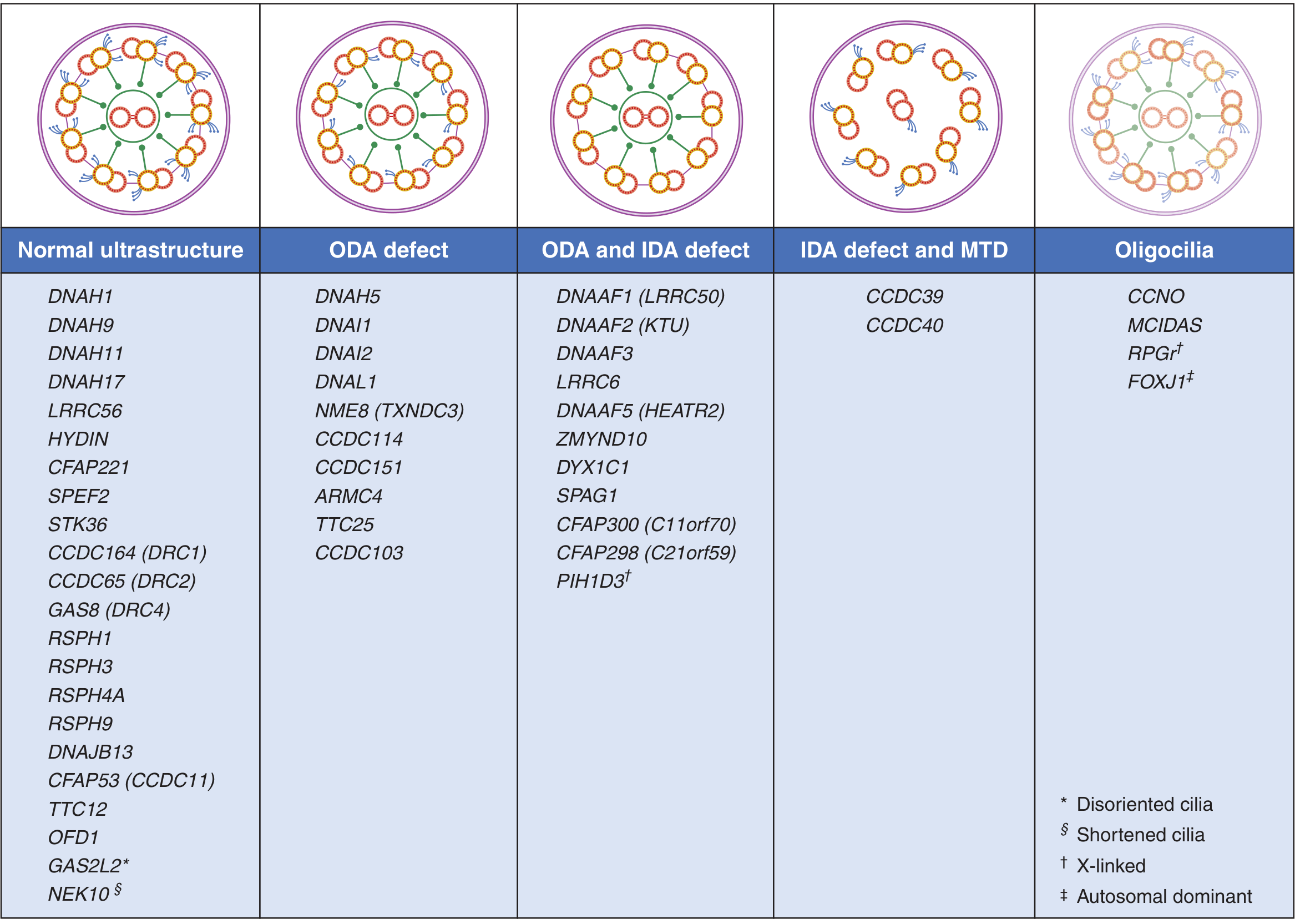
Four main ultrastructural defect patterns:
| Pattern | Example Genes |
|---|---|
| Outer dynein arm (ODA) defect only | DNAH5, DNAI1, DNAI2 |
| ODA + Inner dynein arm (IDA) defect | DNAAF1, DNAAF2, LRRC6 |
| IDA defect + microtubule transposition (MTD) | CCDC39, CCDC40 |
| Oligocilia (few cilia) | CCNO, MCIDAS |
| Normal ultrastructure (functional defect) | DNAH11, HYDIN, RSPH genes |
The diagram below shows these patterns and their associated genes:
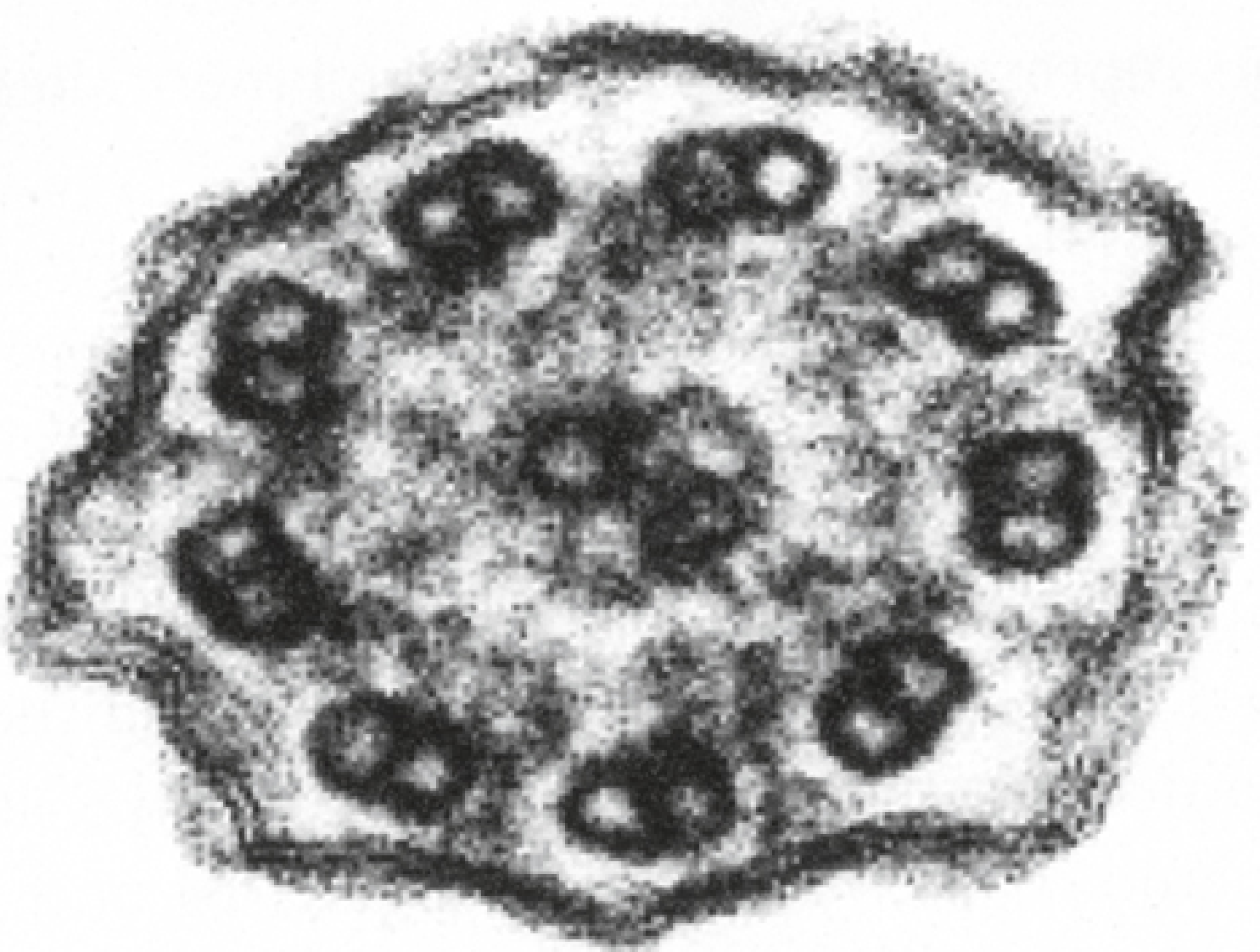
The electron micrograph below shows a cross-section of a cilium from a PCD patient - note the absence of dynein arms on the microtubule doublets:
Pathophysiology
When cilia cannot beat normally, mucociliary clearance fails. The respiratory epithelium normally moves mucus (and trapped bacteria/particles) upward and out. In PCD, this system is severely impaired, leading to:
- Mucus stasis and bacterial overgrowth
- Recurrent infections of the entire respiratory tract (ear, nose, sinuses, lungs)
- Progressive bronchiectasis
Clinical Features
Respiratory (most prominent):
- Daily year-round wet/productive cough from childhood
- Chronic sinusitis and rhinitis - begins under 6 months of age with watery nasal discharge
- Recurrent otitis media with effusion - nearly universal; leads to conductive and sensorineural hearing loss
- Bronchiectasis - right middle lobe and lingula predilection; lower lobe predominant (unlike cystic fibrosis)
- Neonatal respiratory distress at term birth (due to inability to clear lung fluid)
Common pathogens: H. influenzae, S. aureus, smooth strains of P. aeruginosa in childhood; mucoid P. aeruginosa emerges in adulthood
Extra-respiratory:
- Situs inversus in ~50% of patients (all organs mirrored) - when present, the triad of sinusitis + bronchiectasis + situs inversus is called Kartagener Syndrome
- Male infertility - immobile sperm flagella (same 9+2 structure as cilia)
- Female subfertility - impaired fallopian tube ciliary transport; increased risk of ectopic pregnancy
- Hydrocephalus (rare) - ependymal cilia line brain ventricles and help circulate CSF
- Pectus excavatum, scoliosis
Diagnosis
| Test | Notes |
|---|---|
| Nasal nitric oxide (nNO) | Excellent screening test; markedly reduced in PCD. Not diagnostic alone (also low in CF) |
| PICADAR score | Clinical scoring tool (max 14 pts); score ≥5 = sensitivity 90%, specificity 75% |
| Transmission electron microscopy (TEM) | Identifies ultrastructural defects; no longer considered gold standard as some PCD has normal axoneme |
| High-speed video microscopy | Directly visualizes ciliary beat pattern and frequency |
| Genetic panel testing | Identifies causative mutations; confirmatory |
Summary Comparison: PCD vs Cystic Fibrosis
| Feature | PCD | CF |
|---|---|---|
| Cough clearance | Relatively preserved | Severely impaired |
| Bronchiectasis distribution | Lower lobe predominant | Upper lobe predominant |
| Situs inversus | ~50% | Not associated |
| Genetics | Many genes (autosomal recessive) | CFTR gene only |
| nNO | Low | Can be low |
Sources:
- Fishman's Pulmonary Diseases and Disorders (Primary Ciliary Dyskinesia and Other Motile Ciliopathies)
- Murray & Nadel's Textbook of Respiratory Medicine (Chapter 69)
- Histology: A Text and Atlas With Correlated Cell and Molecular Biology (p. 350)
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery
This is a shared conversation. Sign in to Orris to start your own chat.