Loefflers pulmonary eosinophilia
Reading File
Finding Sources
Finding Sources
Searching PubMed
Loeffler syndrome pulmonary eosinophilia
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information to write a detailed answer. Let me compile it.
Loeffler's Pulmonary Eosinophilia (Loeffler Syndrome / Simple Pulmonary Eosinophilia)
Definition and Historical Context
Loeffler first described this syndrome in 1932 as a transient, self-limited clinical condition characterized by three core features:
- Mild respiratory symptoms
- Peripheral blood eosinophilia
- Migratory ("fleeting") pulmonary infiltrates
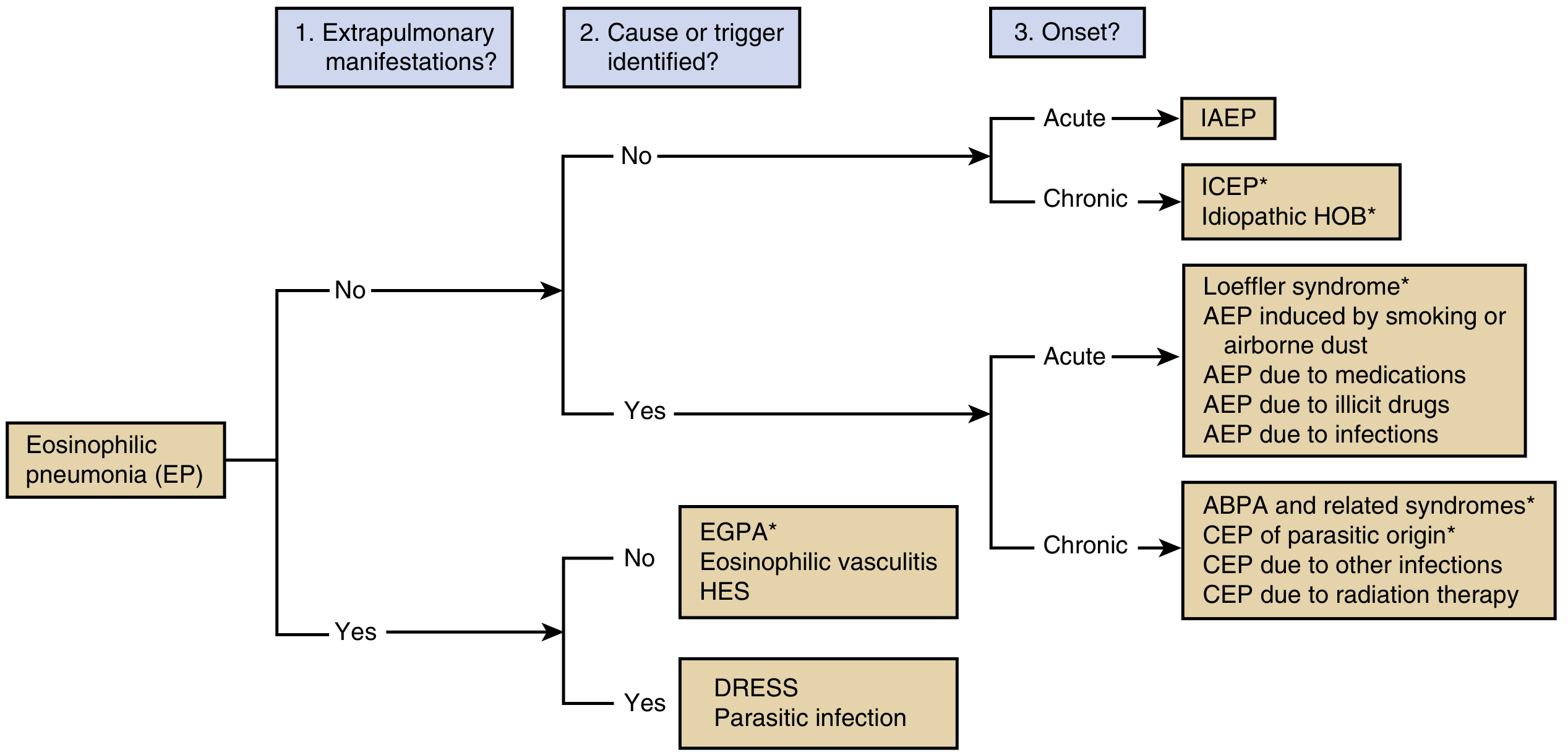
The term "simple pulmonary eosinophilia" is used interchangeably. A classification was formally proposed in 1952 by Crofton and colleagues after reviewing 450 cases in the literature. In the broader scheme of eosinophilic pneumonias, Loeffler syndrome sits in the category of known-cause, acute-onset eosinophilic pneumonia without extrapulmonary manifestations (see diagnostic algorithm below).
Etiology
The primary mechanism is transpulmonary larval migration of helminths. The most common causative agents include:
| Organism | Route of Infection | Geographic Notes |
|---|---|---|
| Ascaris lumbricoides (roundworm) | Ingestion of ova | Most common; now rare in Western countries |
| Ascaris suum | Ingestion | Zoonotic |
| Ancylostoma duodenale, Necator americanus (hookworms) | Skin penetration through feet | Southeastern USA, Mexico, Central/South America |
| Strongyloides stercoralis | Skin penetration | Widely endemic |
| Trichinella spiralis | Ingestion of undercooked meat | Rare |
| Toxocara canis (dog roundworm) | Soil ingestion (visceral larva migrans) | Children most affected |
The term has also been broadened to encompass drug-induced and toxin-induced pulmonary eosinophilia with a similar transient picture. A majority of Loeffler's original cases were likely due to Ascaris lumbricoides, though Ascaris causes Loeffler syndrome in only a small minority of infected individuals.
- Fishman's Pulmonary Diseases and Disorders, 2-Volume Set
Pathogenesis
Following ingestion of Ascaris ova, larvae hatch in the small intestine, cross the intestinal wall, enter the splanchnic and then pulmonary circulation, and migrate across pulmonary capillaries into alveoli. This transpulmonary passage triggers acute eosinophilic inflammation, which resolves once the larvae ascend the airways and descend into the alimentary tract to complete their life cycle. The entire larval lung transit is the mechanistic driver of symptoms.
Key cytokines mediating eosinophil recruitment to the lung:
-
IL-5 (primary) - drives eosinophil differentiation, maturation, tissue recruitment, and survival
-
GM-CSF, IL-3, IL-33 (secondary)
-
Chemokines: eotaxins (CCL11, CCL24, CCL26), LTB4
-
Fishman's Pulmonary Diseases and Disorders
Clinical Features
Loeffler syndrome affects all age groups. Symptoms are generally mild and self-limited, resolving within 1-2 weeks:
- Low-grade fever
- Nonproductive cough
- Mild to occasionally severe dyspnea
- Chest discomfort on coughing or deep breathing
- Wheezing
- Occasional hemoptysis
- Urticaria or skin lesions (especially with hookworm - "creeping eruption": raised, erythematous, serpiginous, tunnel-like, pruritic skin lesion)
Hookworm ("creeping eruption") causes Loeffler syndrome in up to 50% of cases.
Diagnostic Studies
Peripheral blood:
- Moderate to extreme eosinophilia (often peak at time of respiratory symptoms)
Stool examination:
- Negative for ova/parasites in early phase (larvae have not yet matured into egg-laying adults)
- Stool O&P becomes positive approximately 8 weeks after the onset of respiratory symptoms (in keeping with Ascaris life cycle)
Imaging (CXR / CT):
- Migratory, transient, bilateral pulmonary infiltrates - characteristically "fleeting" (appear and resolve in different areas)
- Infiltrates resolve spontaneously as larvae exit the lung
Respiratory secretions:
- Larvae may be recovered from sputum or BAL fluid during the pneumonic phase
- Gastric aspirate may also reveal larvae
Lung biopsy (not routinely required):
- Shows striking eosinophilic infiltration of interstitial and alveolar-capillary units
- Increased macrophages
- No tissue necrosis or vasculitis
- Larvae (Ascaris or hookworm) may be identified in specimens
Treatment and Prognosis
The condition is generally self-limited with an excellent prognosis.
| Treatment | Notes |
|---|---|
| Supportive care | Adequate in most cases |
| Bronchodilators | For symptomatic relief of wheeze/dyspnea |
| Corticosteroids | Rarely needed; for severe symptomatic cases |
| Mebendazole | 100 mg twice daily x 3 days, or single 500 mg dose (for Ascaris) |
| Alternatives | Pyrantel pamoate, albendazole, or ivermectin |
Why treat even if symptoms resolve? Because the late GI manifestations of Ascaris (which begin ~8 weeks after respiratory onset) include malnutrition, diarrhea, abdominal pain, and intestinal obstruction. Antihelminthic treatment prevents this.
Follow-up: Since stool specimens are negative early in illness, clinical follow-up over 2-3 months is indicated with repeat stool O&P.
Position Within the Eosinophilic Pneumonia Classification
Loeffler syndrome is classified as Simple Pulmonary Eosinophilia under "Pulmonary Eosinophilic Syndromes of Known Cause," alongside:
- Drug- or toxin-induced eosinophilic pneumonias
- Tropical pulmonary eosinophilia (Wuchereria bancrofti/Brugia - more severe, with marked eosinophilia >3000/mm³ and bronchospasm)
- Allergic bronchopulmonary mycosis (ABPA)
It contrasts with idiopathic forms (IAEP, ICEP) and systemic forms (EGPA/Churg-Strauss, hypereosinophilic syndrome) by having an identifiable parasitic cause and a benign, self-limited course.
- Fishman's Pulmonary Diseases and Disorders, 2-Volume Set
- Murray & Nadel's Textbook of Respiratory Medicine
- Harrison's Principles of Internal Medicine, 22nd Edition (2025)
This is a shared conversation. Sign in to Orris to start your own chat.