I have pain in testes 2 days ago..pain relives..now..irritation while passing urine...and color is almost normal..what should bhi diagnosis and treatment
epididymo-orchitis STI chlamydia treatment
Your Symptoms - What They Suggest
| Symptom | Significance |
|---|---|
| Testicular pain 2 days ago, now relieved | Likely early epididymo-orchitis or STI-related epididymitis |
| Irritation/burning while urinating | Urethritis - strong indicator of STI (chlamydia or gonorrhea) |
| Normal urine color | Rules out gross hematuria or severe infection |
Most Likely Diagnoses
1. Urethritis from STI (Most Likely - Primary Diagnosis)
"Urethritis from STI presents with dysuria, penile discharge, pain with intercourse, and testicular pain."
"C. trachomatis and N. gonorrhoeae are the most common causes of epididymitis in male patients younger than 35 years of age. Epididymitis presents as unilateral testicular pain and swelling accompanied by dysuria."
2. Acute Epididymo-Orchitis (Secondary/Related)
"In young men [epididymo-orchitis] usually arises secondary to a sexually transmitted genital infection."
3. Acute Prostatitis (Possible)
⚠️ Must Rule Out
- Testicular Torsion - if pain returns suddenly and severely, this is a surgical emergency. The fact that pain has partially resolved is slightly reassuring, but if pain returns suddenly and acutely, go to the emergency department immediately.
- Testicular Tumor - rarely presents with pain, but must be considered if there is any mass or hardness.
Investigations to Get
- Urine NAAT/PCR for Chlamydia and Gonorrhea (most important)
- Urinalysis (midstream urine) - look for WBCs, nitrites
- Urine culture - if bacterial urinary infection suspected
- Scrotal ultrasound - to assess epididymis and testes, and rule out torsion or abscess
- Urethral swab (if discharge present)
- STI screen - HIV, syphilis, hepatitis
Treatment
If STI (Chlamydia/Gonorrhea) Most Likely:
| Drug | Dose | Duration |
|---|---|---|
| Ceftriaxone (for gonorrhea) | 250-500 mg IM, single dose | Once |
| Doxycycline (for chlamydia) | 100 mg orally, twice daily | 10 days |
Supportive Treatment:
- NSAIDs (e.g., ibuprofen 400 mg three times daily with food) for pain and inflammation
- Scrotal support/elevation - helps reduce pain
- Rest, avoid strenuous activity
Additional (if enteric organisms or anal sex history):
- Levofloxacin 500 mg orally once daily for 10 days, OR
- Ofloxacin 300 mg orally twice daily for 10 days
Key Advice
- See a doctor today - do not delay. Even though the testicular pain has reduced, you need proper testing and treatment to prevent complications like infertility or spread of infection.
- Inform and treat sexual partner(s) - STIs require partner notification and simultaneous treatment.
- Abstain from unprotected sex until both you and your partner have completed treatment.
- Do NOT take antibiotics without prescription - wrong antibiotic or incomplete course can cause antibiotic resistance and complications.
- If testicular pain returns suddenly, or you develop fever/chills/vomiting - go to emergency immediately (rule out torsion or abscess).
Disclaimer: This is educational information only, not a substitute for a doctor's consultation. Please visit a urologist, general practitioner, or sexual health clinic for proper examination, testing, and treatment.
- Bailey & Love's Short Practice of Surgery, 28th Ed.
- Tintinalli's Emergency Medicine, Comprehensive Study Guide
- Symptom to Diagnosis: An Evidence-Based Guide, 4th Ed.
- Fitzpatrick's Dermatology, Vol. 1-2
Is it UTI?
Is It a UTI? - Probably Not the Primary Cause
UTI in Males is Uncommon
How to Tell the Difference
| Feature | UTI (Cystitis) | STI / Urethritis |
|---|---|---|
| Burning on urination | Yes | Yes |
| Testicular pain | Rare | Common |
| Urethral irritation/itch | No | Yes |
| Penile discharge | No | Sometimes |
| Urine color change | Often cloudy/dark | Usually normal |
| Fever, chills | Sometimes | Sometimes |
| Age group (men) | Older men, or structural abnormality | Young, sexually active men |
What About Both?
Bottom Line
| Diagnosis | Likelihood |
|---|---|
| STI-related urethritis / epididymo-orchitis | Most likely |
| UTI (complicated cystitis) | Possible but less likely |
| Prostatitis | Worth ruling out |
- Symptom to Diagnosis: An Evidence-Based Guide, 4th Ed.
- Tintinalli's Emergency Medicine
There is no discharge
No Discharge - What Does It Mean?
"The absence of visible discharge does not exclude the diagnosis of urethritis."
"Urethritis can be associated with dysuria or mucopurulent discharge or can be completely asymptomatic."
The Likely Culprit: NGU (Non-Gonococcal Urethritis)
- Mild burning/irritation during urination
- Little or no visible discharge (or only slight clear fluid in the morning)
- Urethral itching or discomfort
Revised Probability With No Discharge
| Diagnosis | Likelihood |
|---|---|
| NGU (Chlamydia) - urethritis | Most likely |
| UTI (cystitis) | Now more likely to consider |
| Gonococcal urethritis | Less likely (usually causes obvious discharge) |
| Prostatitis | Still possible |
How to Diagnose Without Discharge
- Urine PCR/NAAT for Chlamydia and Gonorrhea (most reliable test - done on first-void urine)
- Urinalysis - 10 or more white blood cells (WBCs) per high-power field
- Positive leukocyte esterase on first-void urine dipstick
Key Takeaway
- Rosen's Emergency Medicine
- Swanson's Family Medicine Review
Now treatment in Pakistan brand ..how to to dose it
azithromycin doxycycline brand names Pakistan pharmacy chlamydia urethritis
doxycycline azithromycin ceftriaxone brand names available Pakistan 2024
Treatment Plan for NGU / Chlamydia Urethritis (Pakistan)
Option 1 - Doxycycline (FIRST CHOICE - current guideline preference)
| Details | |
|---|---|
| Generic name | Doxycycline |
| Pakistan brands | Doxin (Pfizer Pakistan), Doxitab, Vibramycin, Doxylin |
| Dose | 100 mg, twice daily (morning + evening) |
| Duration | 7 days |
| Take with | Food and a full glass of water (reduces stomach upset) |
| Do NOT | Lie down for 30 min after taking - causes esophagitis |
| Avoid | Milk/antacids within 2 hours of dose |
| Price | Very affordable - PKR 30-60 per strip widely available |
Option 2 - Azithromycin (If you cannot complete 7 days or prefer single dose)
| Details | |
|---|---|
| Generic name | Azithromycin |
| Pakistan brands | Zithromax (Pfizer), Azithral, Azomax, Orzid, Azibact |
| Dose | 1 gram (1000 mg) as a SINGLE dose (usually 2 x 500 mg tablets together) |
| Duration | Just 1 day - single dose |
| Take with | Can take with or without food |
| Note | Easier to take but slightly less effective than doxycycline for urethral chlamydia |
Option 3 - If Gonorrhea Also Suspected (cover both organisms)
| Details | |
|---|---|
| Generic name | Ceftriaxone |
| Pakistan brands | Rocephin (Roche), Ceftriax, Triaxone, Biotriax |
| Dose | 500 mg IM (injection) - single dose |
| Where | A doctor or clinic gives this injection |
Option 4 - For Pain/Inflammation (Supportive)
| Drug | Pakistan Brand | Dose |
|---|---|---|
| Ibuprofen | Brufen, Neurofen | 400 mg, 3x daily with food |
| Diclofenac | Voltaren, Dyclo | 50 mg, 2x daily with food |
Practical Steps in Pakistan
- Go to a pharmacy - Doxin (Doxycycline) and Azomax/Zithromax (Azithromycin) are available over the counter at most pharmacies in Pakistan without prescription.
- Get Doxin 100mg - ask for a full strip (10 tablets) - take 1 tablet morning, 1 at night for 7 days.
- Add Brufen 400mg for pain relief as needed.
- See a doctor if symptoms do not improve in 3-4 days, pain returns in testis, or you develop fever - you may need the ceftriaxone injection.
- Tell your partner - they must be treated at the same time, otherwise you will re-infect each other.
⚠️ Important Warnings
- Do not stop after 2-3 days just because you feel better - complete the full 7 days
- Do not take doxycycline if you are under 12 years old or pregnant
- Avoid sun exposure while on doxycycline (causes photosensitivity)
- No alcohol with metronidazole if prescribed
Disclaimer: This is for educational guidance. A doctor's consultation and proper testing (urine PCR) is strongly recommended for accurate diagnosis and treatment.
White white fluid is also coming..now best treatment according to Pakistani brand.. complete prescription
🇵🇰 Complete Prescription - Pakistan Brand Names
DRUG 1 - Ceftriaxone Injection (for Gonorrhea)
| Pakistan Brand | Rocephin (Roche) / Ceftriax / Biotriax / Triaxone |
| Dose | 500 mg IM injection - ONE TIME ONLY |
| When | Day 1 only (single dose) |
| Where | Go to any clinic, dispensary, or pharmacy - ask them to give the injection |
| Note | Mixed with lidocaine (lignocaine) to reduce injection pain - ask pharmacist for Rocephin 500mg + lidocaine 1% |
DRUG 2 - Doxycycline Tablets (for Chlamydia + epididymitis)
| Pakistan Brand | Doxin 100mg (Pfizer) / Vibramycin 100mg / Doxitab 100mg |
| Dose | 1 tablet (100mg) TWICE daily - morning + evening |
| Duration | 10 days (important - full 10 days because of testicular involvement) |
| Take with | Food + full glass of water |
| Do NOT | Lie down for 30 min after taking |
DRUG 3 - Ibuprofen (for pain + swelling)
| Pakistan Brand | Brufen 400mg / Neurofen 400mg |
| Dose | 1 tablet (400mg) THREE times daily |
| Duration | 5-7 days |
| Take with | Must take with food - never on empty stomach |
| For | Pain relief + reduces inflammation in testis/epididymis |
DRUG 4 - Scrotal Support
- Wear tight, supportive underwear (not loose boxers) for the next 10 days - this reduces testicular pain and swelling significantly.
Complete 10-Day Prescription Summary
Rx:
1. Inj. Rocephin (Ceftriaxone) 500mg IM
→ STAT (once only, Day 1)
2. Tab. Doxin (Doxycycline) 100mg
→ 1 tablet TWICE daily (morning + night) × 10 days
→ Take with food and water
3. Tab. Brufen (Ibuprofen) 400mg
→ 1 tablet THREE times daily × 5-7 days
→ Take with food only
⚠️ Critical Instructions
| Do | Don't |
|---|---|
| Complete full 10 days of Doxin | Stop early when symptoms improve |
| Tell your sexual partner to get treated | Have unprotected sex during treatment |
| Take Brufen with food | Take Doxin on empty stomach |
| Elevate scrotum with supportive underwear | Ignore if pain returns severely |
| Return to doctor if no improvement in 3 days | Self-adjust the dose |
🚨 Go to Hospital Immediately If:
- Testicular pain returns suddenly and severely (could be torsion)
- You develop fever above 38.5°C
- Testis becomes very swollen or red
- No improvement after 3-4 days of treatment
Disclaimer: This is educational guidance based on standard medical guidelines. A proper doctor's examination, urethral swab, and urine PCR test are strongly recommended before starting antibiotics. Please consult a doctor or urologist for confirmation.
- Harrison's Principles of Internal Medicine, 22nd Ed. (2025)
- Tintinalli's Emergency Medicine
how is it STI .I have not done this
Not All Cases Are STIs - Other Causes Are Very Real
"Epididymitis is typically caused by sexually transmitted pathogens OR by organisms known to cause urinary tract infection."
Non-STI Causes That Fit Your Symptoms Perfectly
1. Acute Bacterial Prostatitis (Very Likely)
- The prostate gland gets infected by normal gut bacteria (E. coli, Klebsiella)
- Causes: burning urination, white/cloudy discharge, pelvic discomfort, sometimes testicular pain
- No sexual contact needed - bacteria from your own bowel travel to the prostate
- Common in young and middle-aged men
- Triggered by: dehydration, holding urine too long, constipation, sitting for long hours, cycling
2. UTI with Prostatitis (Complicated UTI in Males)
- Urinary bacteria spread from bladder to prostate/epididymis
- Same bacteria that cause UTI in women (E. coli) can infect the male urinary tract
- Causes white cells and mild discharge from urethra
3. Epididymo-Orchitis from UTI Bacteria
- Gram-negative enteric bacteria (E. coli, Proteus) travel from urethra upward to the epididymis and testis
- Does not require sexual contact at all
- More common with: urinary tract structural problems, dehydration, kidney stones
4. Non-Specific Urethritis
- Inflammation of the urethra from irritants - tight clothing, chemical irritation, spicy food, concentrated urine from not drinking enough water
What Changes in Your Treatment?
For Non-STI Bacterial Infection (Prostatitis / UTI-origin):
Rx (Pakistan Brands):
1. Tab. Ciprofloxacin (Cipro / Cifran / Ciprowin) 500mg
→ 1 tablet TWICE daily × 14 days
(fluoroquinolones penetrate the prostate very well)
OR
Tab. Levofloxacin (Levaquin / Levotas / Lovomax) 500mg
→ 1 tablet ONCE daily × 10-14 days
2. Tab. Brufen (Ibuprofen) 400mg
→ 1 tablet THREE times daily × 5 days
→ Take with food
3. Drink at least 2.5-3 litres of water daily
Which Doctor to See
- Urologist - best specialist for this
- OR any general doctor / family physician
What Tests to Ask For
| Test | Why |
|---|---|
| Urine complete examination (UCE) | Checks for pus cells, bacteria |
| Urine culture & sensitivity | Identifies exact bacteria + which antibiotic works |
| Scrotal ultrasound | Rules out abscess, torsion, or tumor |
Bottom Line
| You said | What it means |
|---|---|
| No sexual contact | Non-STI cause is very likely |
| White discharge + burning | Prostatitis or UTI-origin urethritis |
| Prior testicular pain | Epididymo-orchitis from UTI bacteria |
Disclaimer: Please see a doctor for proper examination. This is educational guidance only.
- Smith & Tanagho's General Urology, 19th Ed.
- Textbook of Family Medicine, 9th Ed.
Why this happens
How This Happens - Step by Step
The Basic Problem: Bacteria Enter and Travel Up
Bacteria enter urethra
↓
Urethra gets inflamed → burning urine, white discharge
↓
Travel up to PROSTATE → testicular/pelvic pain
↓
Travel further to EPIDIDYMIS/TESTIS → testicular pain and swelling
What Triggers This in Young Men?
Common Everyday Triggers:
| Trigger | How it causes infection |
|---|---|
| Not drinking enough water | Concentrated urine irritates and inflames the urethra. Less urine flow means bacteria are not flushed out |
| Holding urine for long hours | Urine stagnates, bacteria multiply. Pressure forces bacteria into prostate ducts |
| Sitting for long periods (office, driving, studying) | Pressure on the perineum (area between anus and scrotum) compresses prostate and reduces blood flow |
| Constipation | The rectum sits right next to the prostate. Pressure from hard stool pushes bacteria toward the prostate |
| Spicy food / excessive tea or coffee | Irritates the urethral lining, reduces its natural defence barrier |
| Tight clothing / underwear | Increases local heat and pressure in the groin area - bacteria thrive in warm, moist conditions |
| Cold weather / getting chilled | Reduces local blood circulation, weakening immune defences in the pelvic area |
| Reduced immunity (stress, poor sleep, exam pressure) | Body's defences weaken, bacteria that were harmless now cause infection |
| Physical strain / heavy lifting | Can cause urine to reflux (flow backward) into the prostate ducts, carrying bacteria with it |
Why Did Your Testis Hurt First?
Prostate infection → inflammation travels backward through vas deferens → epididymis pain → testis pain
Why the White Discharge?
In Short - Most Likely Reason in Your Case
Bacteria from your own body (like E. coli) found a way into your urethra - possibly due to dehydration, prolonged sitting, constipation, or reduced immunity - and traveled upward infecting the urethra, prostate and temporarily irritating the testicular area.
How to Prevent It Coming Back
- Drink 8-10 glasses of water every day - most important step
- Never hold urine for more than 3-4 hours
- Eat more fruits, vegetables, fibre - prevent constipation
- Avoid excessive tea, coffee, and spicy food during and after treatment
- Take warm baths - reduces pelvic muscle tension
- Do not sit for more than 1-2 hours without a short walk break
Campbell-Walsh-Wein Urology | Textbook of Family Medicine, 9th Ed.
Cranmax and ciprofloxacin is taken before or after food
ciprofloxacin before or after food administration cranberry supplement Cranmax food interaction
Ciprofloxacin (Cifran / Cipro) - Food Timing
✅ Can be taken WITH or WITHOUT food
- Food does not significantly affect its absorption
- However, taking it with a light meal is better to reduce stomach upset (nausea, acidity)
- Do NOT take with milk, yogurt, or dairy alone - calcium blocks absorption
- Do NOT take with antacids (like Gaviscon, Maalox, Mylanta) - they reduce absorption severely. Keep a 2-hour gap between ciprofloxacin and any antacid
Best Practice:
Take Ciprofloxacin after a light meal (not dairy), with a full glass of water
Cranmax (Cranberry Extract) - Food Timing
✅ Take WITH food or after a meal
- Cranberry supplements can cause stomach upset, nausea, or acidity if taken on empty stomach
- Taking after food reduces this irritation
- No major interaction with ciprofloxacin - they are safe to take together
Best Practice:
Take Cranmax after a meal
Important: Cranberry + Ciprofloxacin Interaction
Simple Daily Schedule
| Time | What to take |
|---|---|
| Morning - after breakfast | Ciprofloxacin 500mg + Cranmax |
| Evening - after dinner | Ciprofloxacin 500mg |
| With lunch or any meal | Brufen 400mg (if taking for pain) |
⚠️ Avoid with Ciprofloxacin:
- Milk, yogurt, cheese (within 2 hours)
- Antacids / Gaviscon / calcium tablets (2-hour gap)
- Tea / coffee immediately after (reduces absorption slightly)
- Alcohol
Appendicitis complete.details with history and examination
ACUTE APPENDICITIS - Complete Clinical Guide
1. Definition & Epidemiology
- Accounts for 17% of all emergency abdominal pain presentations
- Lifetime risk: 8.6% in males, 6.7% in females
- Peak age: teens and early twenties
- More common in males (M:F = 3:2 at age 25)
- Rare under 2 years of age and after middle age
2. Aetiology (Causes)
| Cause | Details |
|---|---|
| Faecalith (most common) | Hardened stool/debris blocking the lumen |
| Lymphoid hyperplasia | Viral infection causing lymph tissue to swell and narrow lumen |
| Intestinal parasites | e.g. Enterobius vermicularis (pinworm) |
| Tumour | Caecal carcinoma occluding the appendix orifice (elderly) |
| Fibrotic stricture | From previous appendicitis that resolved |
| Low-fibre diet | Associated with higher incidence |
3. Pathophysiology (How It Progresses)
Luminal obstruction
↓
↑ Intraluminal pressure + mucus secretion
↓
Oedema + mucosal ulceration → Bacterial translocation to submucosa
↓
Venous obstruction → Ischaemia of appendix wall
↓
Bacterial invasion through wall → ACUTE APPENDICITIS
↓
Ischaemic necrosis → GANGRENOUS APPENDICITIS
↓
Perforation → PERITONITIS or APPENDIX ABSCESS

4. History (Symptoms)
Classic Symptom Sequence (present in ~50% of cases):
- Vague, colicky, periumbilical pain (around the navel)
- Poorly localised, intermittent
- Similar to mild small bowel colic but less intense
- Due to appendiceal distension stimulating visceral nerve fibres
- Anorexia (loss of appetite) - very constant feature, especially in children
- Nausea and 1-2 episodes of vomiting (vomiting follows pain onset - Murphy's rule: "pain before vomiting")
- Low-grade fever (37.2-37.7°C)
- Pain migrates to the Right Iliac Fossa (RIF) - lower right abdomen
- Becomes constant, sharp, well-localised
- Worsened by coughing, movement, or deep breathing
- Patient prefers to lie still
Key History Points to Ask:
| Question | Significance |
|---|---|
| Where did the pain start? | Periumbilical → RIF migration is classic |
| Did pain come before vomiting? | Yes = appendicitis. Vomiting first = gastroenteritis |
| Any loss of appetite? | Almost always present in appendicitis |
| Bowel habit changes? | Constipation common; diarrhoea suggests pelvic appendix |
| Urinary symptoms? | Frequency if appendix contacts bladder |
| Last menstrual period (women)? | Rule out ectopic pregnancy, ovarian cyst |
| Any vaginal discharge? | Rule out PID |
| Family history of appendicitis? | Up to 1/3 of children have a first-degree relative affected |
5. Examination (Signs)
General Inspection:
- Patient looks unwell, flushed
- Lies still - movement worsens pain
- May walk bent forward holding right side
- Low-grade pyrexia (37.2-37.7°C); pulse 80-90 bpm
- In 20% of cases, NO fever in early stages
Abdominal Examination:
- Limited respiratory movement in the lower abdomen
- No visible distension (unless perforated)
- Ask patient to point to where pain began, then where it moved (Pointing Sign)
| Sign | How to Elicit | Significance |
|---|---|---|
| McBurney's Point Tenderness | Press on point 1/3 of the way from ASIS to umbilicus | Classic - point of maximum tenderness |
| Guarding (muscle rigidity) | Involuntary tensing of muscles over RIF on palpation | Peritoneal irritation |
| Rebound Tenderness | Press slowly, release quickly - pain on release | Peritoneal inflammation (Blumberg's sign) |
| Rovsing's Sign | Press deep in LEFT iliac fossa → pain felt in RIGHT | Positive = peritoneal irritation, supports appendicitis |
| Psoas Sign | Extend right hip while patient lies on left side → RIF pain | Retrocaecal appendix irritating psoas muscle |
| Obturator Sign | Flex + internally rotate right hip → hypogastric pain | Pelvic appendix irritating obturator internus |
- Tenderness over McBurney's point on gentle percussion
- Elicits rebound tenderness without forceful release
- Tenderness in right side of rectovesical pouch
- Mandatory in every patient with acute lower abdominal pain
- Especially important when appendix is pelvic in position
6. Special Positions of the Appendix & Their Presentation
| Position | % | Special Features |
|---|---|---|
| Retrocaecal (most common, ~65%) | 65% | Loin/back pain, psoas sign positive, abdominal signs may be minimal |
| Pelvic (~30%) | 30% | Suprapubic pain, diarrhoea, urinary frequency, tenderness only on rectal exam |
| Subcaecal | Rare | Pain in RIF |
| Postileal | Rare | Pain does NOT shift, marked nausea/retching, diarrhoea |
| Pre-ileal | Rare | Intestinal obstruction features |
7. Investigations
Routine (all patients):
| Test | Expected Finding |
|---|---|
| Full Blood Count (FBC) | Leukocytosis (WBC >10,000) with neutrophilia; "shift to left" |
| Urinalysis | Usually normal; few pus cells may be present (from adjacent inflammation) |
| C-Reactive Protein (CRP) | Elevated |
| Pregnancy Test (women) | Must exclude ectopic pregnancy |
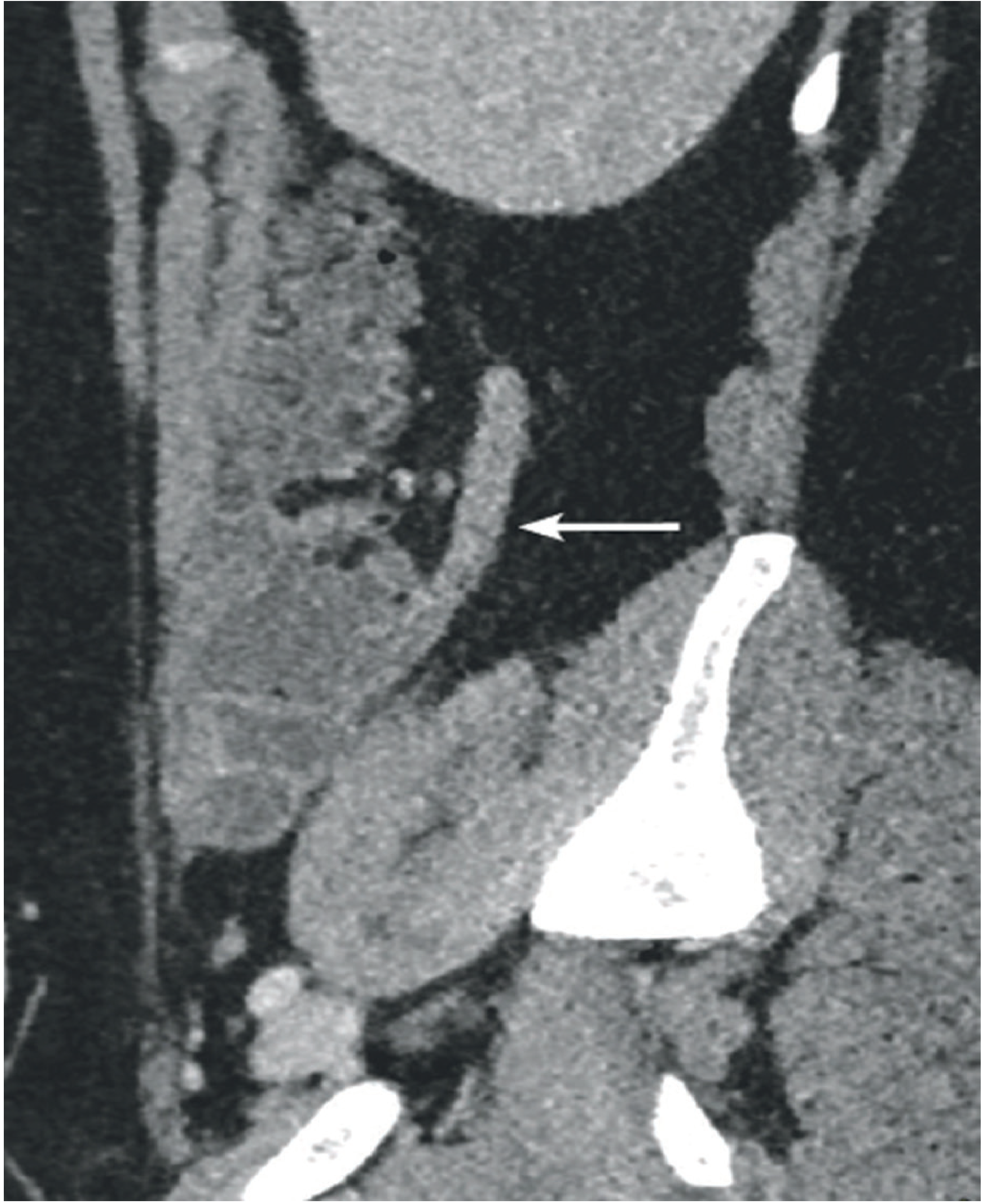
Imaging:
| Investigation | Use | Accuracy |
|---|---|---|
| Ultrasound abdomen | First line - children, thin adults, women (rule out gynaecological cause) | ~90% if visualised |
| CT abdomen/pelvis | Best for equivocal cases, elderly, obese; appendix >10mm diameter diagnostic | ~95% sensitivity and specificity |
| MRI | Pregnant patients (avoids radiation) | Approaching CT accuracy |
| Plain X-ray | Not diagnostic; rarely shows faecalith | Not routinely used |
8. Alvarado Score (MANTRELS) - Clinical Decision Tool
| Feature | Points |
|---|---|
| M - Migratory RIF pain | 1 |
| A - Anorexia | 1 |
| N - Nausea/Vomiting | 1 |
| T - Tenderness RIF | 2 |
| R - Rebound tenderness | 1 |
| E - Elevated temperature | 1 |
| L - Leukocytosis | 2 |
| S - Shift to left (WBC) | 1 |
| Total | 10 |
| Score | Interpretation |
|---|---|
| 1-4 | Appendicitis unlikely - observe/discharge |
| 5-6 | Possible appendicitis - imaging required |
| 7-8 | Probable appendicitis - surgical consult |
| 9-10 | Almost certain appendicitis - operate |
9. Differential Diagnosis
| In Children | In Adults | In Women | In Elderly |
|---|---|---|---|
| Gastroenteritis | Ureteric colic | Ectopic pregnancy | Diverticulitis |
| Mesenteric adenitis | Perforated peptic ulcer | Ovarian cyst torsion/rupture | Colon carcinoma |
| Meckel's diverticulitis | Testicular torsion | PID / Salpingitis | Intestinal obstruction |
| Intussusception | Pancreatitis | Mittelschmerz | Mesenteric infarction |
| Lobar pneumonia | Crohn's disease / terminal ileitis | Endometriosis | Leaking aortic aneurysm |
10. Complications
| Complication | Features |
|---|---|
| Perforation | High fever, diffuse peritonitis, rigid abdomen, very high WBC |
| Appendix abscess (mass) | Palpable RIF mass, swinging fever |
| Generalised peritonitis | Board-like rigidity, sepsis, shock |
| Pylephlebitis | Septic thrombosis of portal vein - rare, very serious |
11. Treatment
Surgical (Standard):
- Appendicectomy (appendix removal) - definitive treatment
- Laparoscopic approach - preferred (faster recovery, less wound infection)
- Open (McBurney's incision) - used when laparoscopy unavailable or perforated
Pre-operative:
- IV fluids, NBM (nil by mouth)
- IV antibiotics: Metronidazole + 3rd generation cephalosporin (e.g. Cefotaxime)
- Analgesia (do NOT withhold - does NOT mask signs)
Non-operative (selected uncomplicated cases):
- IV antibiotics only (Metronidazole + Cephalosporin)
- Successful in ~85% initially
- 25-33% will need surgery within 1 year
Appendix Mass (Ochsner-Sherren Regime):
- Conservative - IV antibiotics, bowel rest, observe
- Mark mass limits on skin with pen
- Measure pulse + temperature 4-hourly
- Operate if: rising pulse, spreading pain, enlarging mass, peritonitis signs
12. Summary - Classic Presentation at a Glance
Young patient (teens-30s)
↓
Sudden periumbilical colicky pain
↓
Anorexia + nausea + 1-2 vomits (pain comes FIRST)
↓
Pain shifts to RIF after 6-8 hours - becomes constant
↓
Low grade fever (37.2-37.7°C)
↓
Examination: RIF tenderness, guarding, rebound, Rovsing's +ve
↓
WBC elevated with neutrophilia
↓
Alvarado score ≥7 → Surgical referral → Appendicectomy
Bailey & Love's Short Practice of Surgery, 28th Ed. | Sleisenger & Fordtran's Gastrointestinal and Liver Disease | Rosen's Emergency Medicine
Hydrocele , verecocele inguinal hernia, testicular torsion.....best brief explanation ..differentiating points....tx
Scrotal Swellings - Complete Guide
1. HYDROCELE
Definition
Types
| Type | Description |
|---|---|
| Communicating | Connected to peritoneal cavity via patent processus vaginalis - size varies with position |
| Non-communicating | Fluid trapped locally - fixed size |
| Primary (idiopathic) | No underlying cause |
| Secondary (reactive) | Due to epididymitis, orchitis, torsion, or tumor |
History
- Painless scrotal swelling
- Gradual onset
- May increase in size during the day (communicating type)
- No fever, no nausea
Examination
| Finding | Details |
|---|---|
| Transillumination | ✅ Positive - light passes through (pathognomonic) |
| Consistency | Soft, fluctuant, smooth |
| Can you get above it? | Yes - confined to scrotum |
| Testis palpable? | Cannot separately palpate testis (surrounded by fluid) |
| Reducible? | No (unlike hernia) |
| Cough impulse | Negative |
| Cremasteric reflex | Normal |
⚠️ Key Warning
Treatment
| Condition | Treatment |
|---|---|
| Infants (<1 year) | Watch and wait - resolves spontaneously by age 1 |
| Adults (symptomatic) | Jaboulay's operation (eversion of tunica) or Lord's procedure (plication) |
| Aspiration | Temporary relief only - high recurrence rate; not recommended |
| Secondary hydrocele | Treat the underlying cause first |
2. VARICOCELE
Definition
Key Facts
- Occurs in 15% of all males; found in 35-40% of infertile males
- 90% left-sided - because left spermatic vein drains at a 90° angle into the left renal vein (higher resistance)
- Right-sided varicocele = rare = suspect retroperitoneal mass / IVC obstruction
History
- Usually asymptomatic
- Dull, dragging ache or heaviness in scrotum, worse after standing/exercise
- May cause subfertility/infertility
- No acute severe pain
Examination
| Finding | Details |
|---|---|
| Classic sign | "Bag of worms" - soft, compressible mass above the testis |
| Position | Superior and posterior to testis |
| Increases with Valsalva | Yes - ask patient to cough or strain |
| Decreases when lying down | Yes - veins empty on supine position |
| Transillumination | ❌ Negative |
| Testis | May be smaller on affected side (testicular atrophy from venous hypertension) |
Grading (Clinical)
| Grade | Description |
|---|---|
| Grade I | Palpable only with Valsalva |
| Grade II | Palpable at rest without Valsalva |
| Grade III | Visible through scrotal skin ("bag of worms" visible) |
Treatment
| Indication | Treatment |
|---|---|
| Asymptomatic, fertile | Observation only |
| Pain or infertility | Surgical ligation (Palomo or inguinal approach) |
| Minimally invasive | Percutaneous venous embolization (equally effective as surgery) |
| Monitor | Scrotal ultrasound + semen analysis |
3. INGUINAL HERNIA
Definition
Types
| Type | Mechanism | Age |
|---|---|---|
| Indirect (most common) | Through deep inguinal ring, along the inguinal canal | Young males, children |
| Direct | Through Hesselbach's triangle (posterior wall weakness) | Older males |
History
- Intermittent bulge in groin or scrotum, appears on straining/coughing/standing
- Usually painless when reducible
- Painful if incarcerated (stuck) or strangulated (blood cut off) - EMERGENCY
- Associated vomiting and abdominal pain if bowel obstructed
Examination
| Finding | Details |
|---|---|
| Cough impulse | ✅ Positive - swelling increases with cough |
| Can get above it? | ❌ No - can NOT get fingers above the swelling (comes from above) |
| Reducible? | Yes (unless incarcerated) - bowel goes back into abdomen |
| Transillumination | ❌ Negative (unless bowel has gas, may rarely glow faintly) |
| Testis | Separately palpable below the hernia |
| Bowel sounds | May be heard over the swelling with stethoscope |
Complications
- Incarceration - hernia stuck, cannot reduce - tender, firm swelling
- Strangulation - blood supply cut off → bowel gangrene - surgical emergency
Treatment
| Type | Treatment |
|---|---|
| Reducible | Elective surgical repair (Herniotomy in children, Herniorrhaphy/Hernioplasty in adults) |
| Laparoscopic | TEP or TAPP procedure - less pain, faster recovery |
| Incarcerated (acute) | Attempt manual reduction (Trendelenburg + gentle pressure), then surgery |
| Strangulated | Emergency surgery immediately |
4. TESTICULAR TORSION
Definition
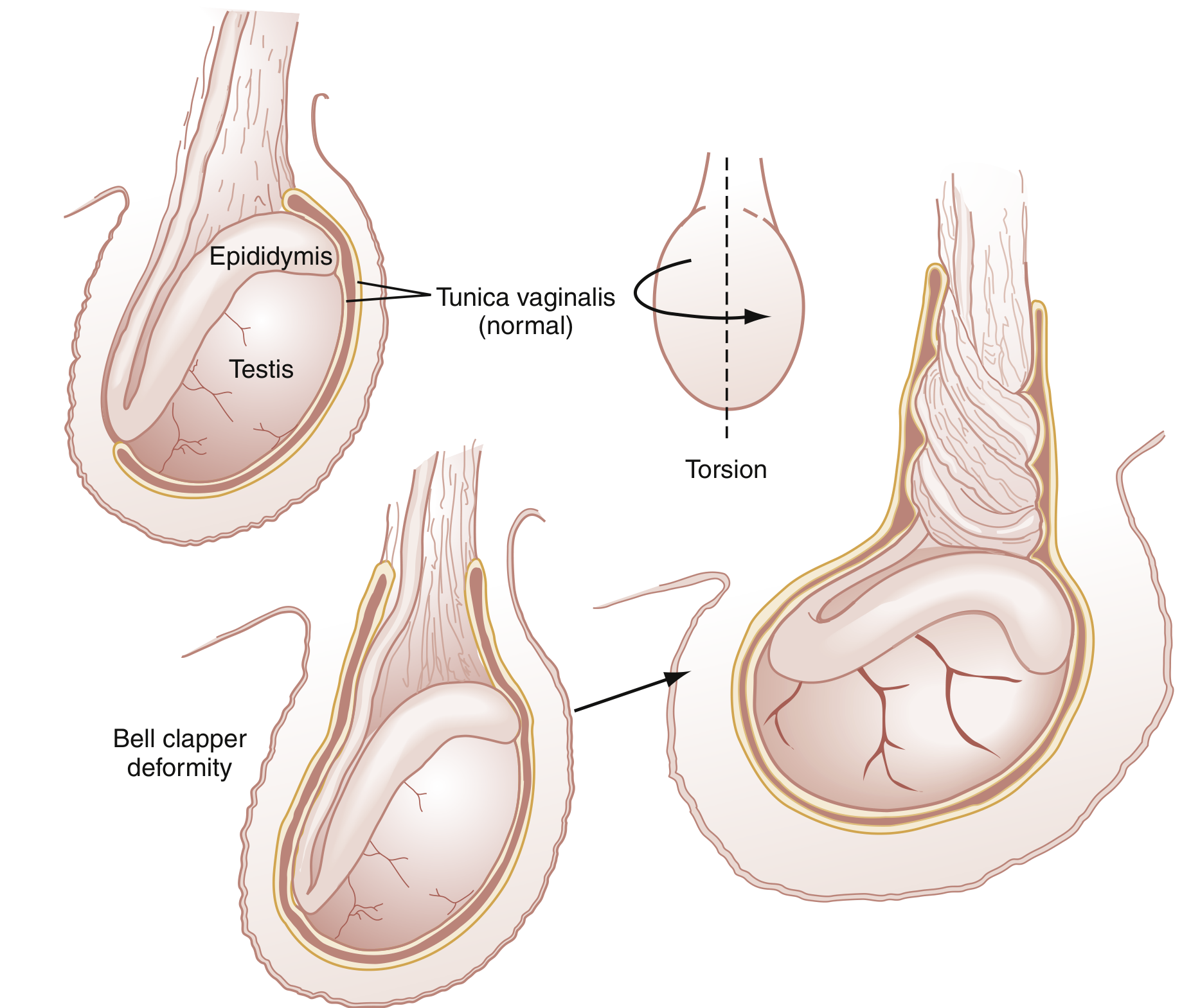
Pathophysiology
- Bell-clapper deformity - testis hangs freely inside the tunica like a clapper in a bell → rotates freely → twists → venous obstruction → arterial ischemia → infarction if not reversed within 6 hours
History
- Sudden, severe, unilateral testicular pain - often wakes patient from sleep
- Onset: within hours (most acute presentation of all scrotal conditions)
- Nausea and vomiting almost always present
- May radiate to abdomen (can be mistaken for appendicitis!)
- Age: bimodal - neonates AND puberty (12-18 years)
- No fever, no dysuria (unlike epididymitis)
Examination
| Finding | Details |
|---|---|
| High-riding testis | ✅ Testis pulled up toward inguinal canal |
| Transverse/horizontal lie | ✅ Testis lies horizontally instead of vertically |
| Cremasteric reflex | ❌ Absent - most reliable sign |
| Prehn's sign | Negative - lifting testis does NOT relieve pain (unlike epididymitis where it relieves pain) |
| Tenderness | Diffuse over entire testis |
| Skin | Scrotal erythema/edema develops later |
| Fever | Absent or mild early on |
Time and Salvage Rate
| Time from onset | Testicular salvage rate |
|---|---|
| < 6 hours | > 90% |
| 6-12 hours | ~50% |
| 12-24 hours | ~10% |
| > 24 hours | ~0% |
Treatment
| Step | Action |
|---|---|
| IMMEDIATE | Emergency urology consult - do NOT delay for tests if clinically obvious |
| Imaging | Doppler ultrasound (decreased/absent blood flow) - only if does NOT delay surgery |
| Temporary (if surgical delay) | Manual detorsion - rotate testis "open book" (lateral direction, like opening a book) |
| Surgery | Orchidopexy (fix testis to prevent recurrence) if viable |
| Non-viable testis | Orchiectomy (remove) + fix contralateral testis |
| Bilateral fixation | Always fix the other side too (bell-clapper is bilateral in 40%) |
MASTER DIFFERENTIATION TABLE
| Feature | Hydrocele | Varicocele | Inguinal Hernia | Testicular Torsion |
|---|---|---|---|---|
| Pain | None | Dull ache | None (unless strangulated) | Severe, sudden |
| Onset | Gradual | Gradual | Intermittent | Acute (hours) |
| Age | Any (common in infants) | Adolescent/adult | Any | Puberty / neonates |
| Transillumination | ✅ Positive | ❌ Negative | ❌ Negative | ❌ Negative |
| Reducible | ❌ No | ❌ No | ✅ Yes | ❌ No |
| Cough impulse | ❌ No | ❌ No | ✅ Yes | ❌ No |
| Can get above it | ✅ Yes | ✅ Yes | ❌ No | ✅ Yes |
| Texture | Smooth, fluctuant | "Bag of worms" | Soft/firm bowel | Swollen, tender testis |
| Cremasteric reflex | Normal | Normal | Normal | ❌ Absent |
| Testis palpable? | Cannot separate | Testis below it | Testis below it | Testis is the mass |
| Valsalva | Increases if communicating | ✅ Increases | Increases | No change |
| Lying down | No change | ✅ Decreases | Reduces | No change |
| Fever | No | No | Only if strangulated | Absent early |
| Nausea/vomiting | No | No | If obstructed | ✅ Yes |
| Urgency | Elective | Elective | Urgent if incarcerated | ⚠️ EMERGENCY |
| Treatment | Jaboulay's operation | Surgery/embolization | Hernia repair | Orchidopexy/orchiectomy |
Quick Memory Trick
| Condition | Remember |
|---|---|
| Hydrocele | "Lights up like a lantern" - transilluminates |
| Varicocele | "Bag of worms" + disappears lying down + left side |
| Inguinal Hernia | "Cannot get above it" + cough impulse + reducible |
| Testicular Torsion | "High, horizontal, no cremasteric, EMERGENCY" |
Rosen's Emergency Medicine | Textbook of Family Medicine, 9th Ed. | Campbell-Walsh-Wein Urology