describe the below embryology topics in detail
Asking for Preferences
It looks like your original message may have had a list of topics that didn't come through - could you please type them out? For example:
- "Gametogenesis, fertilization, cleavage, gastrulation"
- Or paste the list of topics from your textbook/notes
Once I have the specific topics, I'll look them up in the medical library and give you detailed, textbook-quality explanations.
pharyngeal arches and its derivatives
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have all the information needed for a thorough, well-illustrated answer. Here is the full detailed write-up.
Pharyngeal Arches and Their Derivatives
Overview
The pharyngeal (branchial) arches are paired, bar-like thickenings of mesenchyme that develop in the lateral walls of the primordial pharynx during weeks 4-5 of embryonic development. In a 4-week embryo, 4-5 arches are visible on the surface, separated externally by pharyngeal clefts (grooves) and internally by pharyngeal pouches. The 5th arch is rudimentary and the 6th is present but not externally visible.
- The Developing Human: Clinically Oriented Embryology
Structure of a Typical Pharyngeal Arch
Each arch has a core of mesenchyme covered externally by ectoderm and internally by endoderm. The mesenchyme has two origins:
- Neural crest cells - migrate into the arches during week 4 and form skeletal structures (cartilage, bone), dermis, and smooth muscle of the head/neck
- Paraxial and lateral plate mesoderm - form the muscular core of each arch
Each arch also contains:
- An aortic arch artery (arising from the truncus arteriosus)
- A cartilaginous skeletal element
- A cranial nerve (special visceral efferent fibers)
- A muscle primordium
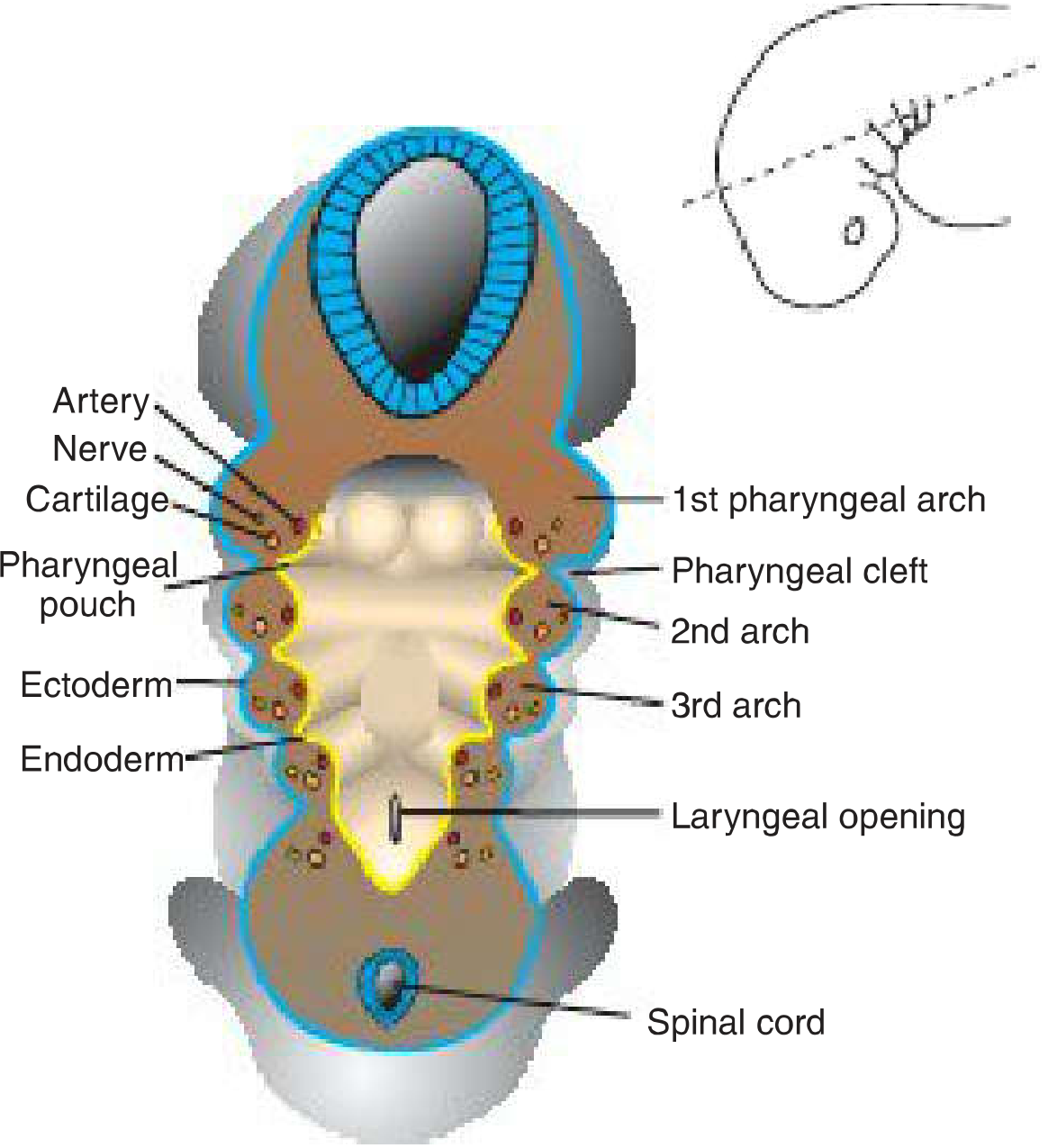
Cross-section through the embryo at the pharyngeal gut level, showing the arch components and their layer arrangement - Langman's Medical Embryology
The Six Pharyngeal Arches in Detail
Arch 1 - The Mandibular Arch
Nerve: Trigeminal nerve (CN V) - maxillary (V2) and mandibular (V3) branches
Cartilage: Meckel's cartilage (first arch cartilage)
- Dorsal end forms the malleus and incus (middle ear ossicles)
- Middle portion regresses, but its perichondrium persists as the anterior ligament of malleus and sphenomandibular ligament
- Mandible develops by intramembranous ossification of mesenchyme surrounding Meckel's cartilage (not directly from it)
- Maxillary process mesenchyme forms the premaxilla, maxilla, zygomatic bone, and part of temporal bone by membranous ossification
Muscles:
- Muscles of mastication (temporalis, masseter, medial and lateral pterygoids)
- Mylohyoid
- Anterior belly of digastric
- Tensor tympani
- Tensor veli palatini
Clinical note: Arch 1 has two prominences - the maxillary process (dorsal) and mandibular process (ventral, containing Meckel's cartilage).
Arch 2 - The Hyoid Arch
Nerve: Facial nerve (CN VII)
Cartilage: Reichert's cartilage
- Stapes (middle ear ossicle)
- Styloid process of temporal bone
- Stylohyoid ligament
- Lesser cornu (horn) of hyoid bone
- Upper part of body of hyoid bone
Muscles:
- Muscles of facial expression (frontalis, orbicularis oculi, orbicularis oris, buccinator, etc.)
- Stapedius
- Stylohyoid
- Posterior belly of digastric
- Auricular muscles (external ear)
Key point: Myoblasts from the 2nd arch migrate from the neck to the head to form the muscles of facial expression, carrying CN VII with them. This explains why CN VII innervates all muscles of facial expression.
Arch 3
Nerve: Glossopharyngeal nerve (CN IX)
Cartilage:
- Lower part of the body of hyoid bone
- Greater cornu (horn) of hyoid bone
Muscles:
- Stylopharyngeus (the only muscle derived from arch 3)
Arch 4
Nerve: Superior laryngeal branch of vagus nerve (CN X)
Cartilage (combined with arch 6):
- Thyroid cartilage (superior cornu)
- Contributes to cricoid, arytenoid, corniculate, and cuneiform cartilages
Muscles:
- Cricothyroid
- Levator veli palatini
- Constrictors of the pharynx (superior, middle, inferior)
Arch 5
Rudimentary - no significant derivatives
Arch 6
Nerve: Recurrent laryngeal branch of vagus nerve (CN X)
Cartilage (fused with arch 4):
- Cricoid cartilage
- Arytenoid, corniculate, and cuneiform cartilages
Muscles:
- Intrinsic muscles of the larynx (except cricothyroid)
- Striated muscles of the esophagus
Summary Table of Derivatives
| Arch | Nerve | Skeletal Derivatives | Muscle Derivatives | Ligaments |
|---|---|---|---|---|
| 1st (Mandibular) | CN V (V2, V3) | Malleus, Incus, Mandible, Maxilla, Zygomatic, Temporal bone | Mastication muscles, Mylohyoid, Ant. belly digastric, Tensor tympani, Tensor veli palatini | Ant. lig. of malleus, Sphenomandibular lig. |
| 2nd (Hyoid) | CN VII | Stapes, Styloid process, Lesser cornu & upper body hyoid | Facial expression muscles, Stapedius, Stylohyoid, Post. belly digastric, Auricular | Stylohyoid lig. |
| 3rd | CN IX | Greater cornu & lower body hyoid | Stylopharyngeus | - |
| 4th | CN X (superior laryngeal) | Superior cornu thyroid cartilage, Thyroid cartilage | Cricothyroid, Levator veli palatini, Pharyngeal constrictors | - |
| 6th | CN X (recurrent laryngeal) | Cricoid, Arytenoid, Corniculate, Cuneiform cartilages | Intrinsic laryngeal muscles, Esophageal striated muscle | - |
Cartilage Derivatives - Visual Summary
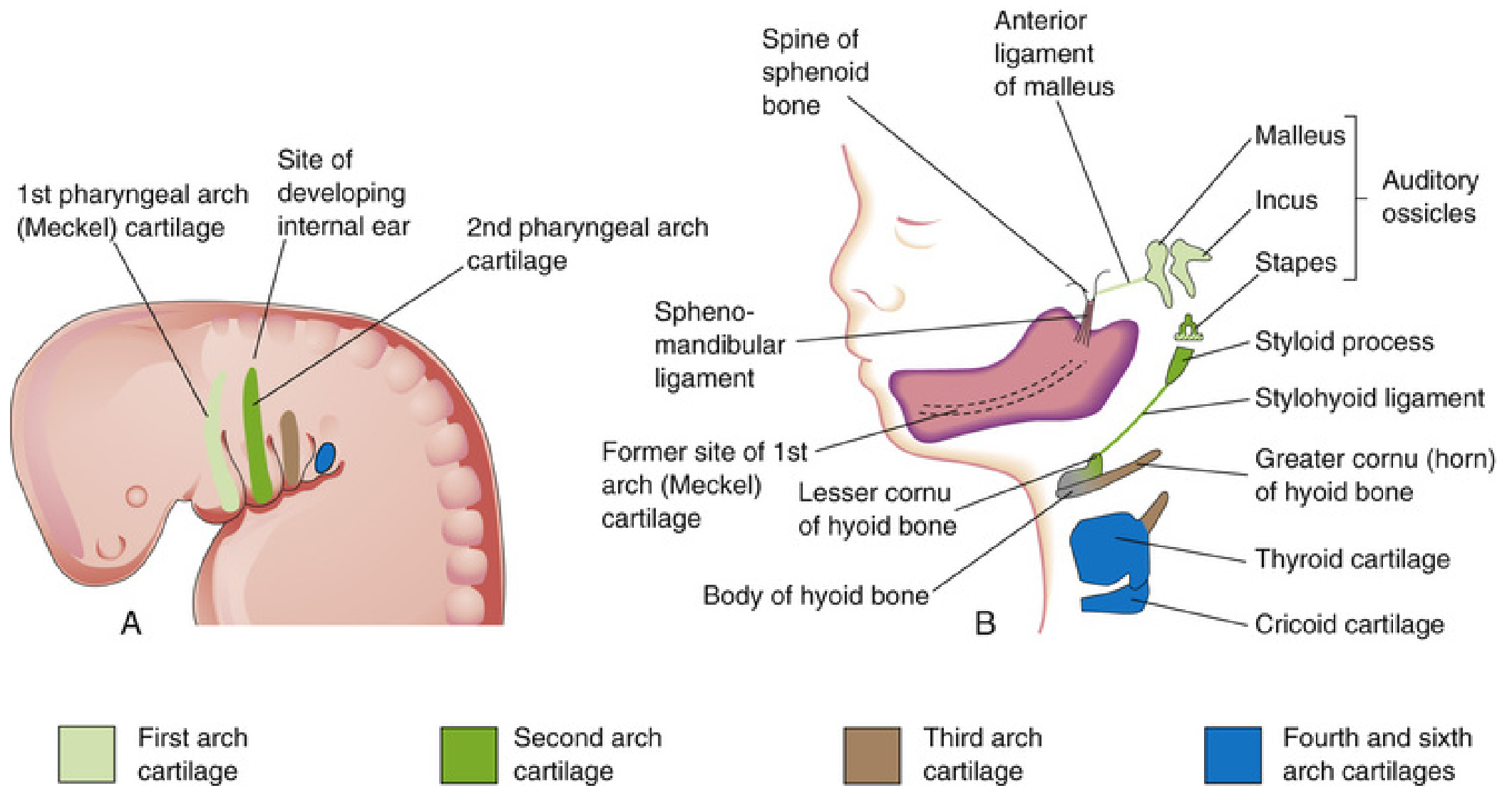
Arch cartilages at 4 weeks (left) and their derivatives at 24 weeks (right) - The Developing Human
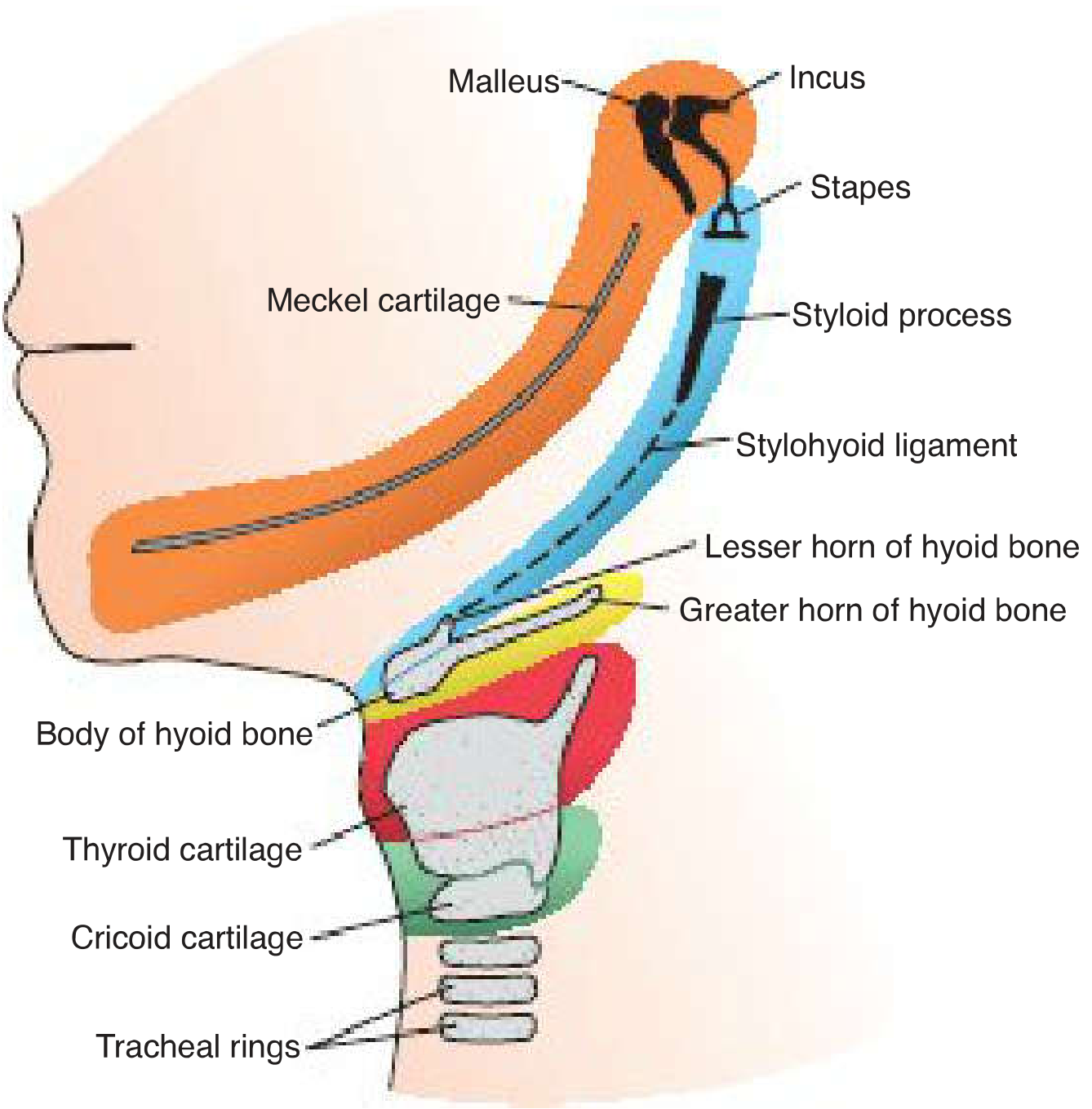
Definitive cartilage derivatives from each pharyngeal arch - Langman's Medical Embryology
Pharyngeal Pouches (Endodermal Derivatives)
Between the arches internally are 4 pairs of pouches (5th is rudimentary) lined by endoderm:
| Pouch | Derivative |
|---|---|
| 1st | Tubotympanic recess → middle ear cavity (tympanic cavity) + auditory (Eustachian) tube |
| 2nd | Palatine tonsil (tonsillar fossa) |
| 3rd (dorsal wing) | Inferior parathyroid glands (parathyroid III) |
| 3rd (ventral wing) | Thymus |
| 4th (dorsal wing) | Superior parathyroid glands (parathyroid IV) |
| 4th (ventral wing) | Ultimobranchial body → parafollicular (C) cells of thyroid |
Pharyngeal Clefts (Ectodermal Derivatives)
Only the 1st pharyngeal cleft persists and forms the external auditory meatus (EAM). Clefts 2-4 are obliterated by overgrowth of the 2nd arch, forming the cervical sinus of His. Failure of obliteration leads to lateral cervical (branchial) cysts and fistulas.
Clinical Correlates
1. First Arch Syndrome
Results from insufficient migration of neural crest cells into the first arch during week 4.
- Treacher Collins Syndrome (Mandibulofacial Dysostosis): Autosomal dominant; mutation in TCOF1 gene (encodes treacle protein involved in ribosomal RNA biogenesis). Features: malar hypoplasia, down-slanting palpebral fissures, lower eyelid defects, deformed external ears, possible middle/inner ear defects.
- Pierre Robin Sequence: Micrognathia (small mandible) → posterior tongue displacement → bilateral cleft palate. Most cases are de novo; rarely autosomal dominant.
2. DiGeorge Syndrome (22q11.2 Deletion Syndrome)
Failure of neural crest migration into pharyngeal arches 3 and 4. Results in:
- Absent/hypoplastic thymus → T-cell immunodeficiency
- Absent/hypoplastic parathyroids → hypoparathyroidism, hypocalcemia
- Cardiac outflow tract defects (aortic arch anomalies, VSD, truncus arteriosus)
- Facial features: shortened philtrum, low-set ears, nasal clefts
3. Branchial (Lateral Cervical) Cysts and Fistulas
Persistence of the cervical sinus (failure of 2nd arch to obliterate clefts 2-4). Present as painless lateral neck masses or sinuses along the anterior border of the sternocleidomastoid.
Memory Aids
Nerve supply mnemonic (1-2-3-4-6):
V - VII - IX - X(sup) - X(rec) "Very Fine Girls Are Exceptional"
Arch 2 muscle mnemonic (PSPAD-A):
Stapedius, Stylohyoid, Posterior belly digastric, Auricular, muscles of facial expression (All = CN VII)
"MIST" for 1st arch skeletal derivatives:
Malleus, Incus, Sphenomandibular ligament, Temporal bone (part)
Sources: The Developing Human: Clinically Oriented Embryology (Moore et al.); Langman's Medical Embryology (Sadler); General Anatomy and Musculoskeletal System - THIEME Atlas
gastrulation
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have all the content needed. Here is the full detailed answer on gastrulation.
Gastrulation
Definition and Timing
Gastrulation is the formative process by which the bilaminar embryonic disc (epiblast + hypoblast) is converted into a trilaminar embryonic disc containing all three primary germ layers: ectoderm, mesoderm, and endoderm. It also establishes the embryo's body axes (cranio-caudal, dorso-ventral, left-right).
-
Occurs during week 3 of development
-
The embryo during this stage is called a gastrula
-
It is the most significant developmental event of the third week and is the beginning of morphogenesis (development of body form)
-
Key signaling molecules: BMPs, FGF8, Sonic Hedgehog (Shh), Wnt, Tbx16, Tgifs
-
The Developing Human: Clinically Oriented Embryology, Langman's Medical Embryology
Background: The Bilaminar Disc
Before gastrulation, the embryonic disc has two layers:
- Epiblast (upper layer) - columnar cells forming the floor of the amniotic cavity
- Hypoblast (lower layer) - cuboidal cells forming the roof of the umbilical vesicle (yolk sac)
The epiblast is the source of all three germ layers through gastrulation. The hypoblast is displaced and eventually contributes to extraembryonic structures.
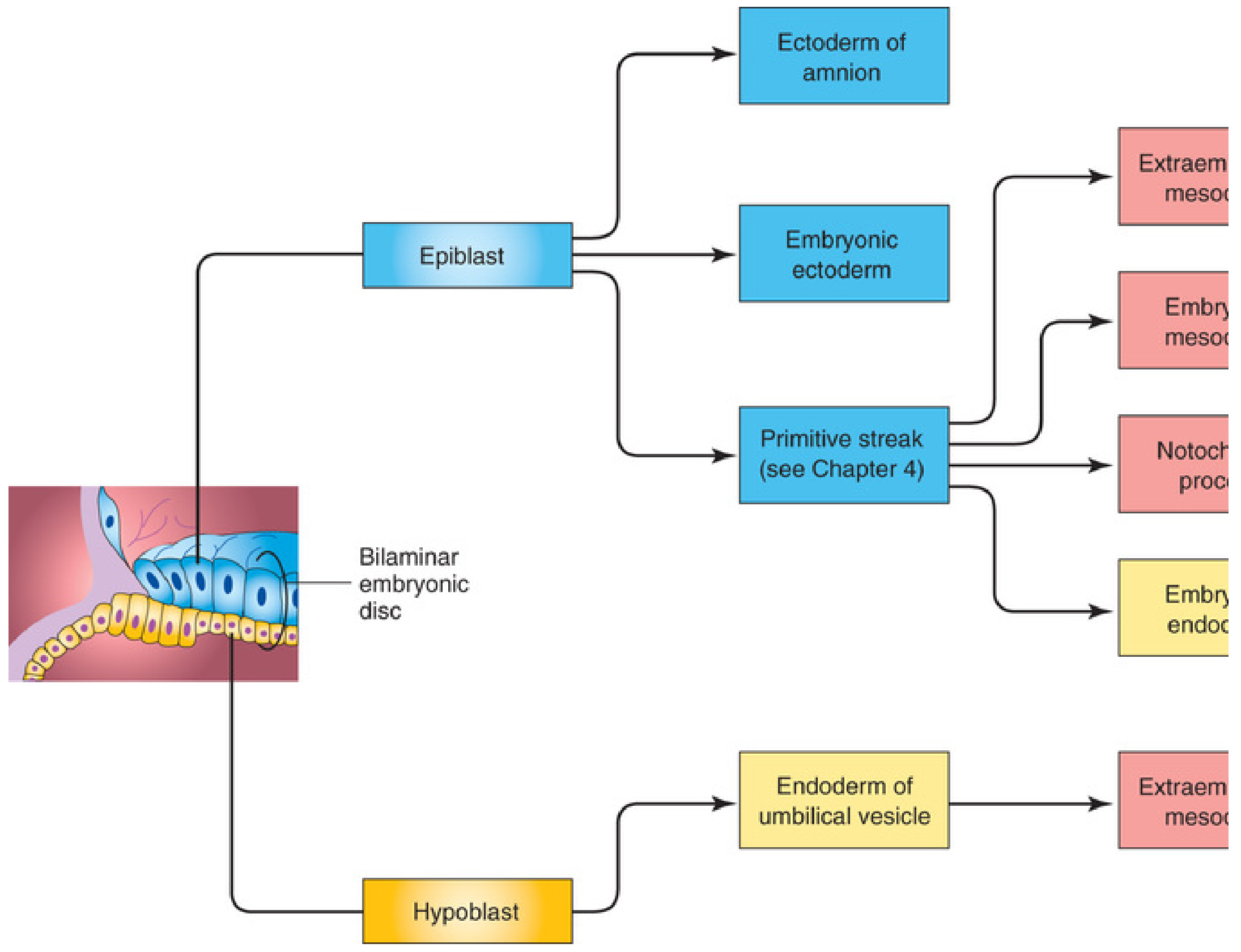
Origin of embryonic tissues from the bilaminar disc - The Developing Human
Step 1: Formation of the Primitive Streak
The first morphological sign of gastrulation is appearance of the primitive streak on the dorsal surface of the epiblast at the caudal end of the embryonic disc, beginning day 15.
How it forms:
- Epiblast cells proliferate and migrate toward the median plane at the caudal end
- This forms a thickened linear band called the primitive streak
- As the streak elongates caudally, its cranial end enlarges to form the primitive node (Hensen's node)
- The primitive node has a central depression called the primitive pit; the streak itself has a midline groove called the primitive groove, with slightly elevated edges called primitive ridges
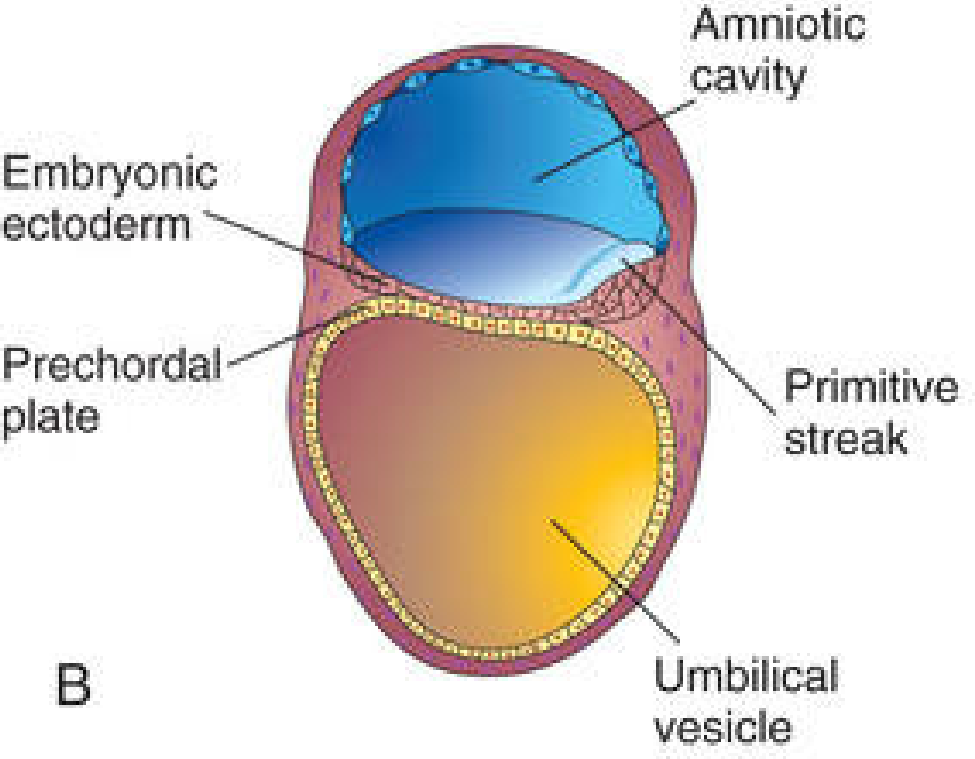
3-week embryo showing the primitive streak, prechordal plate, and embryonic ectoderm - The Developing Human
Significance of the primitive streak:
- Establishes the embryo's axes: once it appears, you can identify cranial/caudal ends, dorsal/ventral surfaces, and right/left sides
- The caudal end of the streak marks the future tail end; the cranial end marks the head end
Step 2: Invagination and Formation of Germ Layers
Epiblast cells migrate toward the primitive streak, become flask-shaped, detach from the epiblast layer, and slip beneath it - a process called invagination (also termed ingression).
FGF8 (secreted by streak cells) is the key molecular driver:
- It downregulates E-cadherin - loosening cell-cell adhesion between epiblast cells, allowing them to detach and migrate
- It regulates BRACHYURY (T) expression - specifying cells into mesoderm
Once invaginated, cells have two fates:
| Fate | What happens |
|---|---|
| Embryonic endoderm | Some invaginating cells displace the hypoblast entirely, creating the definitive endoderm lining the gut tube |
| Embryonic mesoderm | Other cells settle between the epiblast and newly formed endoderm, spreading laterally and cranially |
| Embryonic ectoderm | Epiblast cells that do NOT ingress remain as the ectoderm |
The key principle: the epiblast is the sole source of all three germ layers.
Step 3: Spread of Mesoderm and Fate Map
As more cells invaginate through different levels of the streak, they migrate cranially and laterally, spreading between ectoderm and endoderm:
- Cranially, they pass on either side of the prechordal plate (a midline region of tightly adherent ecto-endoderm that forms just cranial to the oropharyngeal membrane)
- Laterally, they establish contact with extraembryonic mesoderm covering the yolk sac and amnion
- Cranially and caudally, two membrane regions remain without mesoderm between them:
- Oropharyngeal membrane (cranially) - future mouth opening
- Cloacal membrane (caudally) - future anal/urogenital openings
Epiblast Fate Map (ingression through different streak levels)
| Region of ingression | Mesoderm formed |
|---|---|
| Cranialmost part of node | Prechordal plate and notochord |
| Lateral edges of node + cranial streak | Paraxial mesoderm (somites, head mesoderm) |
| Mid-streak region | Intermediate mesoderm (urogenital system) |
| More caudal streak | Lateral plate mesoderm (body wall, limbs) |
| Caudalmost streak | Extraembryonic mesoderm (chorion) |
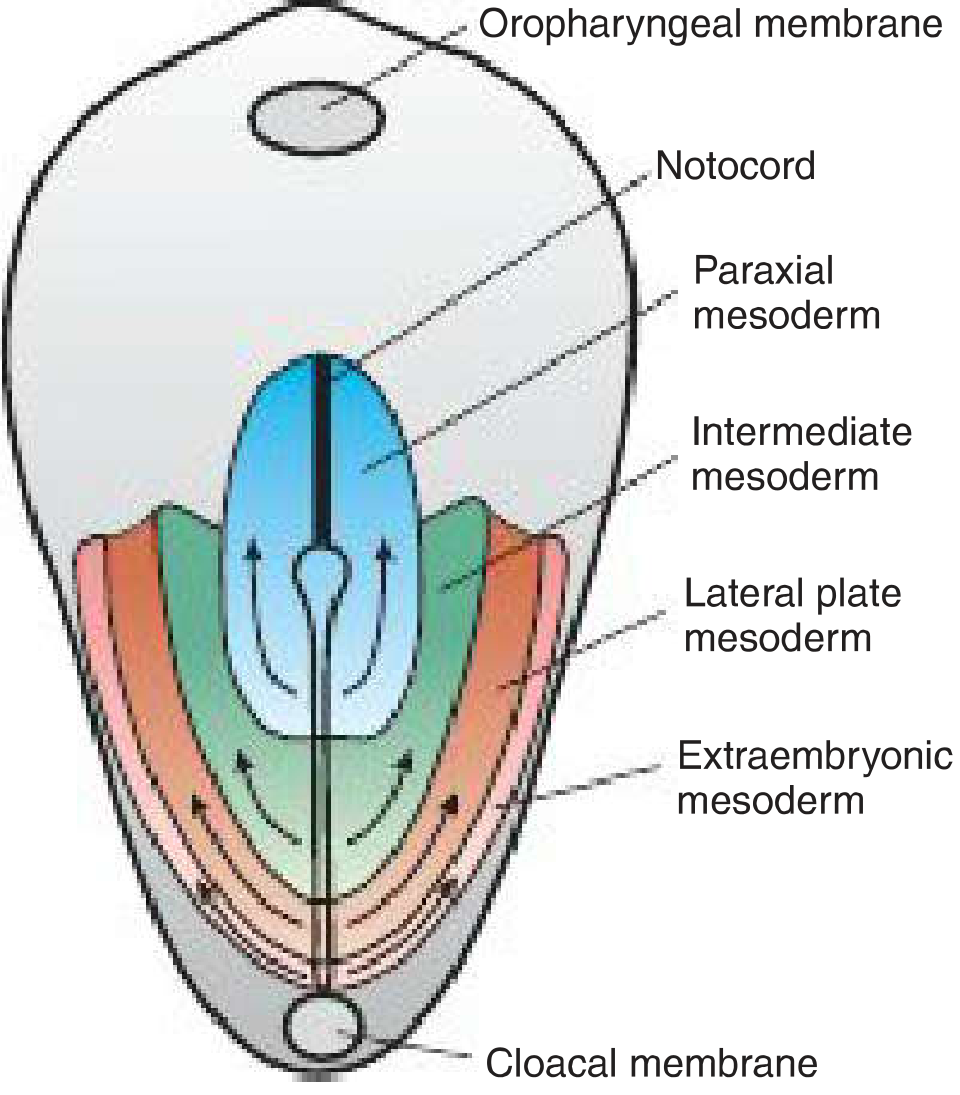
Fate map showing how different regions of the primitive streak produce different mesodermal subdivisions - Langman's Medical Embryology
Step 4: Formation of the Notochord
Prenotochordal cells that invaginate at the primitive node move cranially in the midline, between ectoderm and endoderm, all the way to the prechordal plate:
- These cells first intercalate into the hypoblast, creating a transient notochordal plate
- As endoderm cells replace the hypoblast, the notochordal plate cells proliferate and detach, forming a solid cellular rod - the definitive notochord
- The notochord initially forms a hollow tube (the notochordal canal), which temporarily communicates with the amniotic cavity above and the umbilical vesicle below through the neurenteric canal
- The floor of the canal degenerates, forming a flat notochordal plate, which then folds in on itself to create the solid notochord
- The neurenteric canal normally obliterates once notochord development is complete
Functions of the Notochord:
- Defines the primordial longitudinal axis of the embryo and gives it rigidity
- Acts as the primary inducer in the early embryo - induces the overlying ectoderm to thicken into the neural plate (primordium of the CNS)
- Contributes to the nucleus pulposus of intervertebral discs in adults
- Largely degenerates as vertebral bodies form around it
What the Three Germ Layers Give Rise To
| Germ Layer | Adult Derivatives |
|---|---|
| Ectoderm | Epidermis; CNS and PNS; eyes, internal ears; neural crest cells; connective tissues of the head |
| Mesoderm | All skeletal muscles; blood cells; blood vessel lining; smooth muscle (visceral); serosal linings of body cavities; reproductive and excretory ducts/organs; cardiovascular system; cartilage, bone, tendons, ligaments, dermis of trunk |
| Endoderm | Epithelial lining of respiratory and digestive tracts; liver, pancreas (glandular cells); glands opening into the GI tract |
Growth of the Embryonic Disc
- The disc is initially flat and nearly round; it elongates with a broad cranial end and narrow caudal end
- Growth occurs mainly in the cephalic region - driven by continuous cell migration from the primitive streak in the cranial direction
- The primitive streak remains relatively fixed in size at the caudal end
- By the end of week 4, the primitive streak shows regressive changes, rapidly shrinks, and disappears
- Development proceeds in a cephalocaudal direction: cranial germ layers differentiate by mid-week 3, while caudal regions are still forming germ layers by the end of week 4
Clinical Correlates
1. Caudal Dysgenesis (Sirenomelia)
Insufficient mesoderm formation in the caudal region of the embryo. Because this mesoderm contributes to the lower limbs, urogenital system (intermediate mesoderm), and lumbosacral vertebrae, defects in all these structures result:
- Hypoplasia and fusion of lower limbs (mermaid-like appearance)
- Vertebral abnormalities
- Renal agenesis
- Imperforate anus
- Genital anomalies
Associated with maternal diabetes in humans; in mice, caused by mutations in BRACHYURY (T), WNT, and ENGRAILED genes.
2. Sacrococcygeal Teratoma
Remnants of the primitive streak persist in the sacrococcygeal region. Because primitive streak cells are pluripotent, they proliferate and form teratomas containing tissues from all three germ layers. This is the most common tumor in newborns (frequency: 1 in 37,000). More common in female fetuses; may become malignant.
3. Teratogenic Sensitivity
The start of week 3 is the most teratogen-sensitive period in development - fate maps for organ systems such as the eyes and brain anlagen can be damaged. For example, high-dose alcohol at this stage kills cells in the anterior midline, contributing to holoprosencephaly and fetal alcohol spectrum disorders.
4. Laterality Defects
Establishment of left-right asymmetry occurs during gastrulation. Failure leads to:
- Situs inversus - complete mirror-image reversal of all organs
- Situs ambiguus (heterotaxy) - discordant organ positioning, with possible isomerisms or inversions of the heart chambers, associated with congenital heart defects
5. Notochordal Remnant Tumors (Chordomas)
Persistent notochordal tissue can form chordomas, slow-growing tumors. Approximately one-third occur at the base of the cranium and extend to the nasopharynx. Malignant forms infiltrate adjacent bone.
Summary: Key Events Week by Week
| Day | Event |
|---|---|
| Day 15 | Primitive streak appears on epiblast (caudal midline) |
| Day 15-16 | Primitive node and pit form at the cranial end of the streak |
| Day 16-17 | Epiblast cells invaginate through streak - endoderm and mesoderm form |
| Day 17-19 | Notochordal process extends cranially from primitive node to prechordal plate |
| Day 19-20 | Notochordal plate forms, then folds to create definitive notochord |
| Day 20+ | Neural plate induced by notochord; cephalocaudal germ layer differentiation underway |
| End of week 4 | Primitive streak regresses and disappears |
Sources: The Developing Human: Clinically Oriented Embryology (Moore et al.); Langman's Medical Embryology (Sadler); General Anatomy and Musculoskeletal System - THIEME Atlas of Anatomy; Creasy & Resnik's Maternal-Fetal Medicine
spermatogenesis and oogenesis
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Finding Sources
Reading File
Reading File
I now have everything needed for a thorough, well-illustrated answer. Here is the full detailed write-up.
Spermatogenesis and Oogenesis
Both are forms of gametogenesis - the process by which diploid precursor cells give rise to haploid gametes (spermatozoa and oocytes) through meiosis.
PART 1: SPERMATOGENESIS
Definition and Overview
Spermatogenesis is the sequence of events by which spermatogonia (primordial male germ cells) are transformed into mature spermatozoa. It occurs continuously in the seminiferous tubules of the testes from puberty (~age 13) throughout most of adult life, though it decreases in old age. The entire process takes approximately 64-74 days.
Production statistics: 2 million spermatogonia begin the process daily; each spermatogonium gives rise to 64 spermatozoa → approximately 128 million sperm produced daily.
- Costanzo Physiology 7th Edition, Guyton and Hall Textbook of Medical Physiology
Location: The Seminiferous Tubule
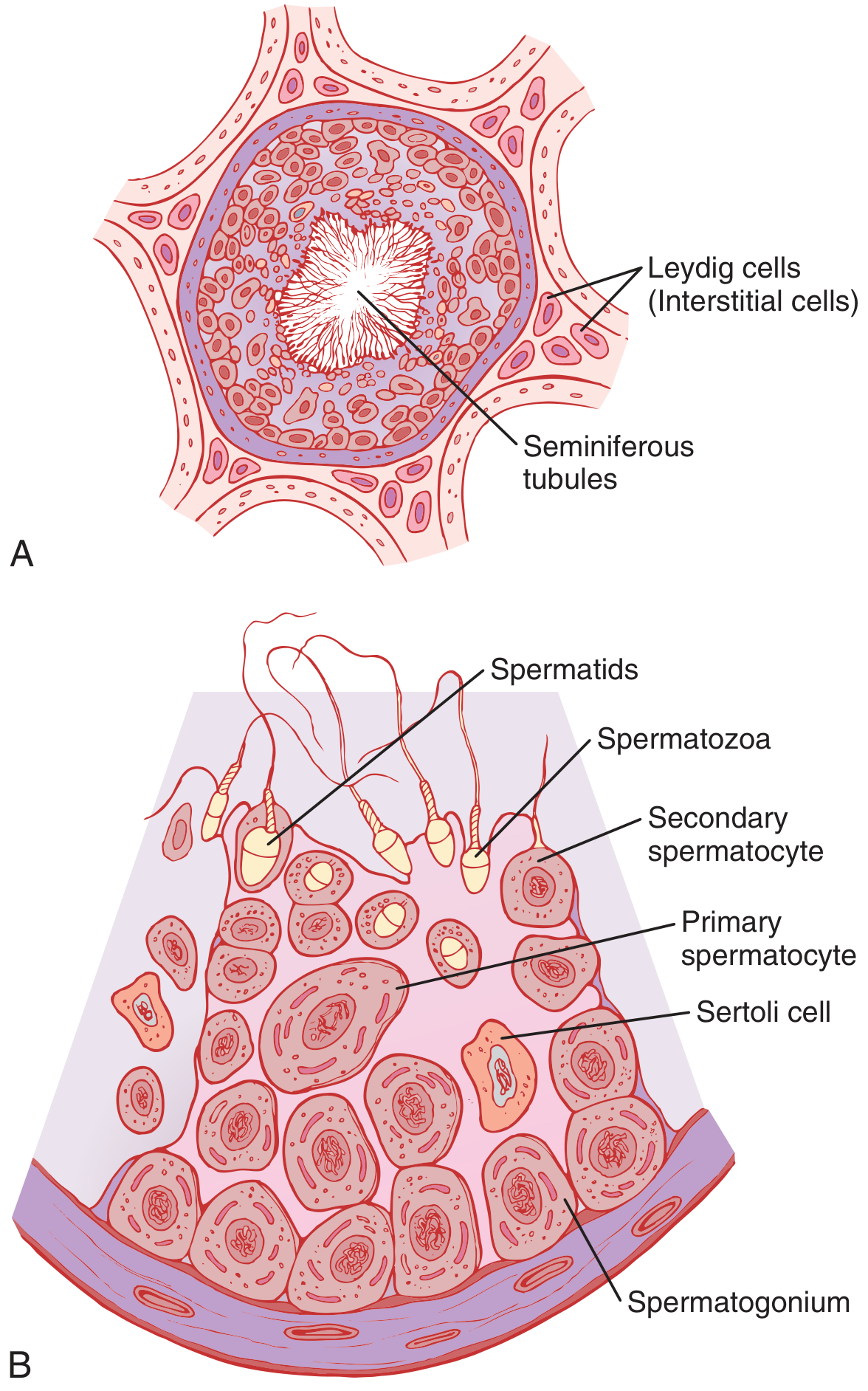
Seminiferous tubule histology showing stages of spermatogenesis - Guyton & Hall Medical Physiology
The seminiferous tubule wall has:
- Sertoli cells - large supporting cells with overflowing cytoplasm that surround, nurture, and regulate all developing germ cells
- Leydig (interstitial) cells - in the connective tissue between tubules; produce testosterone under LH stimulation
- A blood-testis barrier formed by tight junctions between Sertoli cells, dividing the tubule into a basal compartment (spermatogonia) and an adluminal compartment (all later stages)
Three Phases of Spermatogenesis
Phase 1 - Mitotic Proliferation (Spermatogonia)
Spermatogonia lie in the basal compartment against the basement membrane. They are classified as:
| Type | Role |
|---|---|
| Type A (pale, Ap) | Stem cells - divide at 16-day intervals, self-renew AND produce committed progenitors |
| Type A (dark, Ad) | Reserve stem cells - remain quiescent, replenish Ap population |
| Type B | Committed progenitor cells - undergo a final mitotic division to produce primary spermatocytes |
Key feature: Mitotic divisions occur with incomplete cytokinesis - cells remain connected by cytoplasmic bridges, forming a spermatogenic syncytium. This allows haploid cells to share products of the complete diploid genome (including X- and Y-linked proteins) and coordinates progression through meiosis.
- Junqueira's Basic Histology
Phase 2 - Meiotic Divisions (Spermatocytes)
Primary spermatocytes cross the blood-testis barrier into the adluminal compartment and enter meiosis - the longest phase of spermatogenesis.
Meiosis I (Reductive division):
- Primary spermatocyte (2n, 4C = diploid, 4N DNA) → 2 secondary spermatocytes (haploid, 2N DNA)
- This is the longest phase - primary spermatocytes spend ~3 weeks in prolonged prophase I (leptotene → zygotene → pachytene → diplotene → diakinesis)
- Crossing-over (recombination) occurs during prophase I, generating genetic diversity
Meiosis II (Equatorial division):
- Each secondary spermatocyte → 2 spermatids (haploid, 1N DNA)
- Final result: 4 haploid spermatids from each primary spermatocyte
- Of the 4 spermatids: 2 carry the X chromosome, 2 carry the Y chromosome
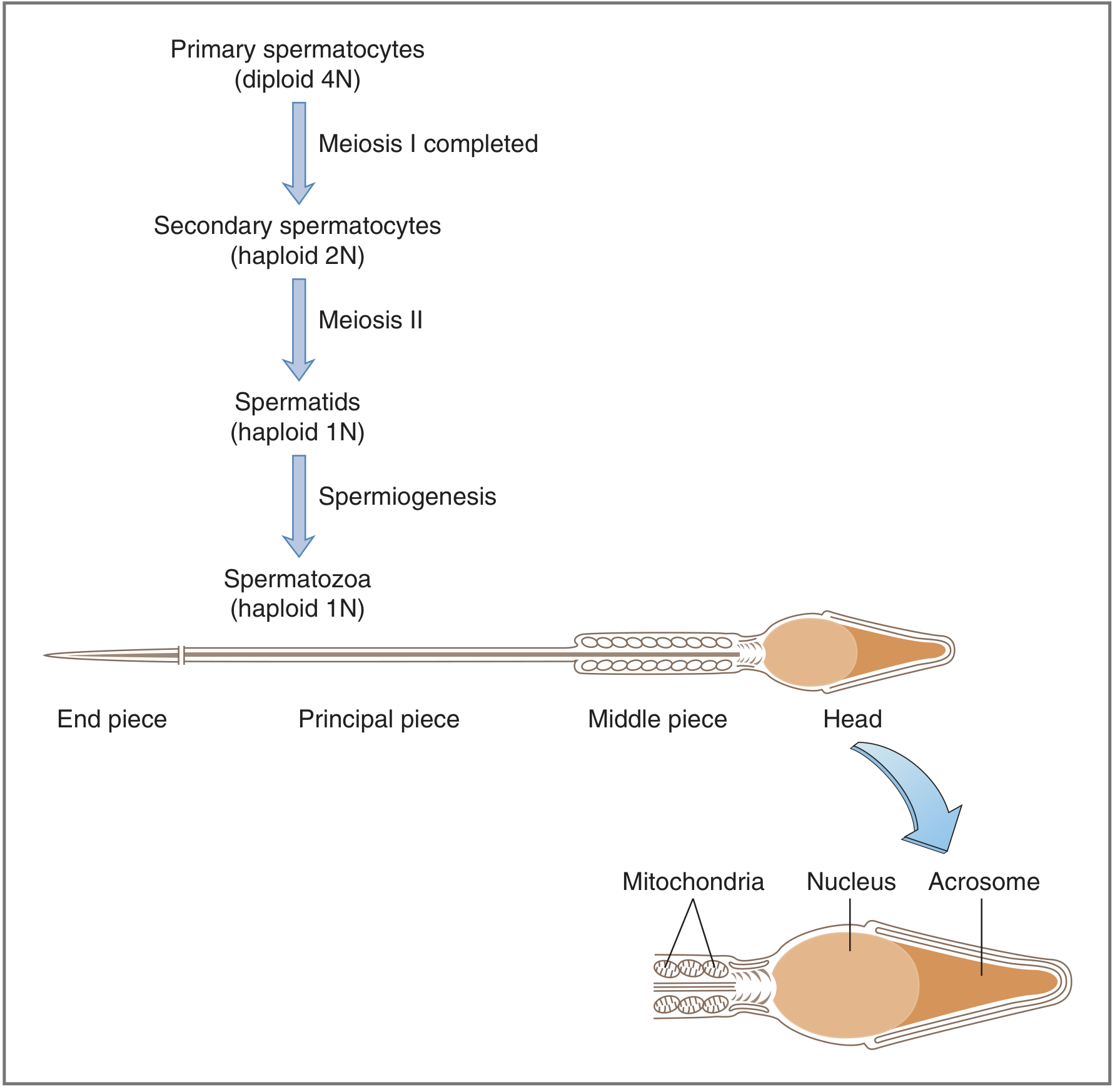
Stages of spermatogenesis and structure of the mature spermatozoon - Costanzo Physiology
Phase 3 - Spermiogenesis (Transformation of Spermatids → Spermatozoa)
Spermiogenesis is the final phase - a morphological transformation with NO cell division. Round spermatids (7-8 μm) are remodeled into streamlined spermatozoa.
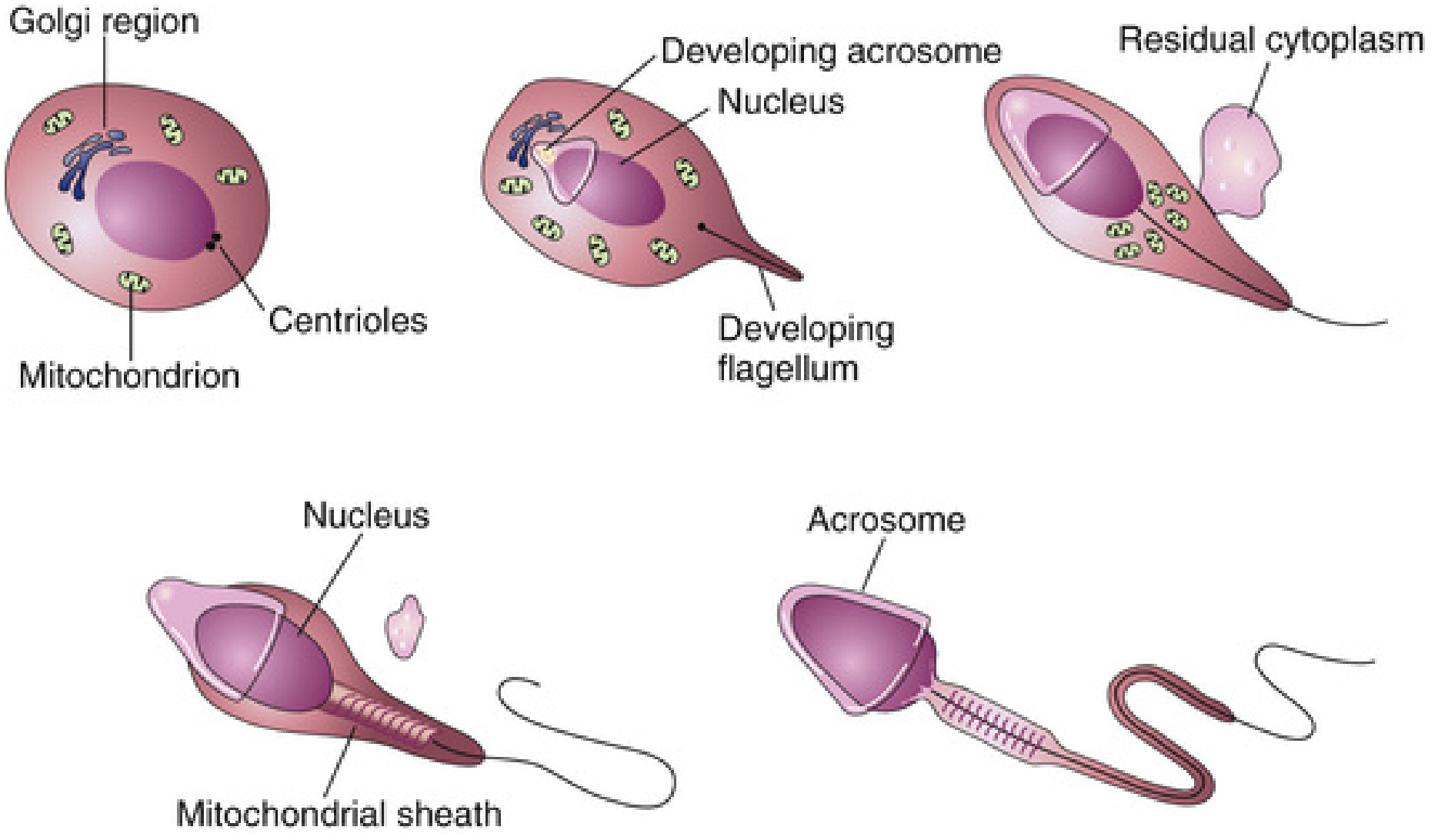
Stages of spermiogenesis showing acrosome formation, flagellum development, and cytoplasm loss - The Developing Human
Steps of spermiogenesis:
- Acrosome formation - Golgi apparatus vesicles merge over the nucleus to form the acrosomal cap (contains hyaluronidase, acrosin, neuraminidase, phospholipase A, and esterases)
- Nuclear condensation - Nucleus becomes elongated and compact (histones replaced by protamines)
- Flagellum development - Centrioles organize the axoneme (9+2 microtubule arrangement) that forms the tail
- Mitochondrial sheath - Mitochondria migrate to wrap around the proximal tail → middle piece
- Loss of excess cytoplasm - Residual cytoplasm shed as residual bodies (phagocytosed by Sertoli cells)
Structure of a Mature Spermatozoon
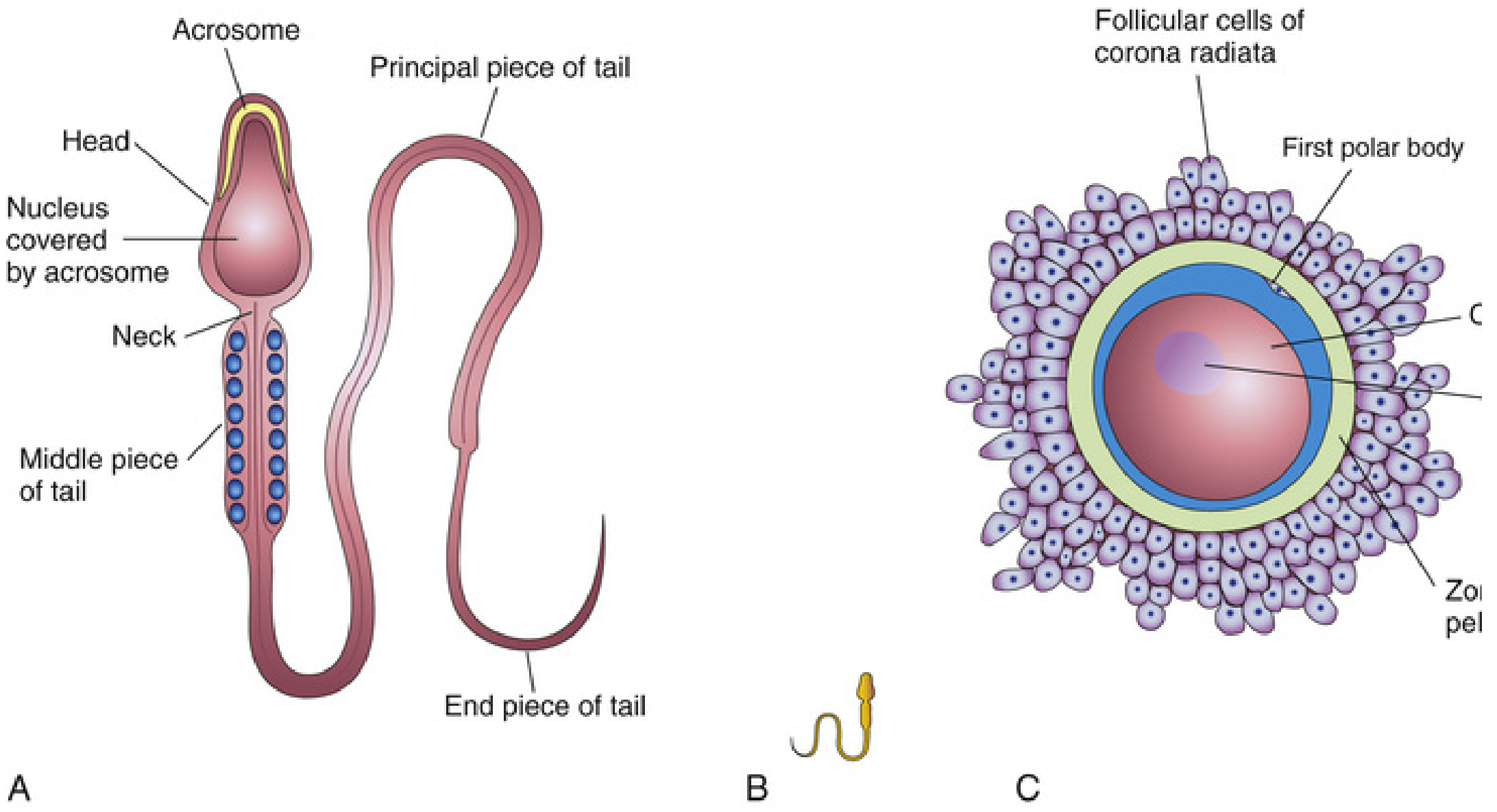
Human sperm (left) compared in scale to secondary oocyte (right) - The Developing Human
| Region | Contents | Function |
|---|---|---|
| Head | Nucleus (haploid) + acrosome (anterior 2/3) | Carries genetic material |
| Acrosome | Hydrolytic enzymes (hyaluronidase, acrosin) | Penetrates corona radiata and zona pellucida |
| Neck | Centrioles | Junction between head and tail |
| Middle piece | Mitochondria arranged in helical sheath | ATP production for motility |
| Principal piece | Fibrous sheath around axoneme | Main motile segment |
| End piece | Axoneme only | Terminal flagellar motion |
Hormonal Regulation of Spermatogenesis
| Hormone | Source | Action |
|---|---|---|
| GnRH | Hypothalamus (pulsatile) | Stimulates anterior pituitary to release FSH and LH |
| FSH | Anterior pituitary | Acts on Sertoli cells → stimulates spermatogenesis; induces androgen-binding protein (ABP) secretion |
| LH (ICSH) | Anterior pituitary | Acts on Leydig cells → testosterone production |
| Testosterone | Leydig cells | Essential for spermatogenesis; acts via androgen receptors on Sertoli cells; also responsible for male secondary sexual characteristics |
| Inhibin | Sertoli cells | Negative feedback to pituitary → suppresses FSH |
| Activin | Sertoli cells | Positive regulation of FSH |
| DHT | Target tissues (via 5α-reductase) | Active androgen in prostate, skin, external genitalia |
Temperature requirement: Spermatogenesis requires a temperature 2-3°C below core body temperature (maintained by the pampiniform venous plexus acting as a countercurrent heat exchanger). Cryptorchidism causes azoospermia due to heat damage.
Sperm Transport and Maturation
After spermiogenesis, spermatozoa enter the tubule lumen and are transported to the epididymis, where:
- They acquire forward motility and fertilizing capacity over ~2 weeks
- They can be stored for several months while remaining viable
- Capacitation (final activation) occurs in the female reproductive tract over 4-6 hours: inhibitory seminal factors are washed away, cholesterol is withdrawn from sperm membrane, Ca²⁺ influx increases, and the acrosomal membrane fuses with the outer sperm membrane
Accessory gland contributions to semen:
- Seminal vesicles (60%): fructose (energy), prostaglandins, fibrinogen, citrate
- Prostate (30%): citrate, calcium, alkaline enzymes (neutralizes acid, increases motility)
- Bulbourethral glands (5%): mucus
PART 2: OOGENESIS
Definition and Key Contrast with Spermatogenesis
Oogenesis is the sequence of events by which oogonia are transformed into mature oocytes. It is fundamentally different from spermatogenesis in several critical ways:
| Feature | Spermatogenesis | Oogenesis |
|---|---|---|
| Onset | Puberty | Begins in fetal life (week 8-9) |
| Duration | Continuous from puberty | Begins fetal life, completes at fertilization |
| Output | 4 functional haploid cells per meiosis | 1 functional oocyte + up to 3 polar bodies |
| Arrest | None | Arrested at prophase I (until puberty), then metaphase II (until fertilization) |
| Production | Continuous throughout adult life | Fixed pool - no new oogonia after birth |
| Number | ~128 million/day | ~400-500 ovulated in lifetime |
| Cytoplasm division | Equal | Unequal - oocyte retains most cytoplasm |
Prenatal Phase: Oogonia → Primary Oocytes
Timing: Weeks 8-9 of gestation to ~6 months after birth
- Primordial germ cells migrate from the dorsal endoderm of the yolk sac along the mesentery of the hindgut to the germinal epithelium of the ovarian cortex
- They divide mitotically to produce oogonia - peak at ~7 million oogonia by weeks 20-24 of gestation
- From week 8-9 onward, oogonia begin entering meiosis I, becoming primary oocytes
- Meiosis is immediately arrested in late prophase I (dictyotene stage) - this suspended state can last up to 50 years (until menopause)
- Connective tissue cells surround each primary oocyte to form a primordial follicle (primary oocyte + single layer of flattened granulosa cells)
- By birth: only ~1-2 million primary oocytes remain (massive atresia reduces the pool)
- No new oogonia are produced after birth - females work from this fixed, declining pool
Postnatal Phase: Follicular Development and Ovulation
At birth → puberty: massive atresia continues; by puberty only ~300,000-400,000 primary oocytes remain
Three stages of follicular development:
Stage 1 - Primordial → Primary → Secondary Follicle (Years)
- Granulosa cells proliferate and become cuboidal → columnar
- Primary oocyte grows and develops zona pellucida (glycoprotein coat: ZP1, ZP2, ZP3)
- Theca interna cells differentiate and begin steroid production
- Granulosa cells begin secreting fluid
- Duration: 13-50 years (minimum age at first ovulation to menopause)
Stage 2 - Secondary → Graafian (Antral) Follicle (70-85 days)
- Occurs only during reproductive period
- Fluid accumulates in a central cavity - the antrum (contains steroids, mucopolysaccharides, proteins, FSH)
- Follicle reaches 2-5 mm diameter - called a Graafian follicle
- Several follicles enter this stage each cycle
Stage 3 - Dominant Follicle Selection and Ovulation (5-7 days before ovulation)
- A single dominant follicle achieves dominance; its cohorts undergo atresia
- Within 48 hours, dominant follicle grows to ~20 mm
- On day 14 of a 28-day cycle, the LH surge triggers ovulation
- The primary oocyte COMPLETES meiosis I just before ovulation:
- → Secondary oocyte (retains most cytoplasm) + 1st polar body (extruded, degenerates)
- The secondary oocyte then enters meiosis II but arrests again at metaphase II
Meiotic Arrests Summarized
| Stage | Cell | Where arrested | What triggers completion |
|---|---|---|---|
| Prophase I | Primary oocyte | Ovarian follicle | LH surge (puberty onward) |
| Metaphase II | Secondary oocyte | Fallopian tube | Penetration by spermatozoon |
| Completion of meiosis II | Secondary oocyte → Ovum | - | Fertilization → 2nd polar body extruded → haploid ovum |
Oocyte maturation inhibitor (OMI) - secreted by granulosa cells; keeps meiosis arrested in prophase I until the LH surge overcomes it.
Comparison of Oocyte Numbers Through Life
| Stage | Oocyte count |
|---|---|
| Peak (gestational weeks 20-24) | ~7 million oogonia |
| Birth | ~1-2 million primary oocytes |
| Puberty | ~300,000-400,000 |
| Lifetime ovulations | ~400-500 |
| Menopause | Near zero |
The long duration of meiotic arrest (up to 45 years in some oocytes) explains the increase in meiotic errors (nondisjunction, aneuploidy) with advancing maternal age - e.g., trisomy 21 (Down syndrome) rates rise sharply after age 35.
Corpus Luteum
After ovulation, the ruptured follicle collapses and is transformed into the corpus luteum (composed of granulosa and theca cells, capillaries, fibroblasts):
- Secretes progesterone and estrogen to prepare the endometrium for implantation
- If fertilization occurs: hCG from the trophoblast maintains the corpus luteum until the placenta takes over hormone production (~weeks 8-10)
- If no fertilization: corpus luteum degenerates after ~14 days → corpus albicans → progesterone withdrawal → menstruation
Hormonal Regulation of Oogenesis / Ovarian Cycle
| Hormone | Source | Action |
|---|---|---|
| GnRH | Hypothalamus (pulsatile) | Drives FSH and LH release |
| FSH | Anterior pituitary | Stimulates follicle growth, granulosa proliferation, estrogen synthesis |
| LH | Anterior pituitary | LH surge → triggers ovulation and completion of meiosis I; stimulates corpus luteum |
| Estrogen | Granulosa/theca cells | Stimulates endometrial proliferation; positive feedback → LH surge |
| Progesterone | Corpus luteum | Prepares endometrium for implantation; negative feedback on hypothalamus/pituitary |
| Inhibin | Granulosa cells | Suppresses FSH |
Clinical Correlates
| Condition | Mechanism | Result |
|---|---|---|
| Trisomy 21 (Down syndrome) | Nondisjunction during meiosis I of oogenesis; frequency increases with maternal age | Trisomy 21 |
| Klinefelter syndrome (47, XXY) | Nondisjunction in meiosis I (maternal or paternal) | Testicular failure, azoospermia |
| Turner syndrome (45, X) | Loss of X chromosome; accelerated oocyte atresia | Premature ovarian failure, infertility |
| Cryptorchidism | Undescended testis - elevated temperature disrupts spermiogenesis | Azoospermia/infertility if untreated |
| Y chromosome microdeletions | Deletions in AZF (azoospermia factor) loci on Y chromosome | Oligospermia/azoospermia, male infertility |
| Polycystic ovary syndrome | Failure of dominant follicle selection; LH/FSH imbalance | Anovulation, infertility |
| Premature ovarian insufficiency | Accelerated oocyte atresia | Early menopause, infertility |
Sources: The Developing Human: Clinically Oriented Embryology (Moore et al.); Langman's Medical Embryology (Sadler); Costanzo Physiology 7th Ed.; Guyton & Hall Textbook of Medical Physiology; Junqueira's Basic Histology
yolk and twin pregnancy
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Loading Image
Finding Sources
I now have all the key content and images needed. Let me write the complete detailed answer.
Yolk Sac (Umbilical Vesicle) and Twin Pregnancy
PART 1: THE YOLK SAC (UMBILICAL VESICLE)
Terminology
The structure commonly called the "yolk sac" is more accurately termed the umbilical vesicle in humans, because - unlike in birds and reptiles - it contains no nutritive yolk. The term yolk sac is retained in clinical usage but this distinction is important.
- The Developing Human: Clinically Oriented Embryology
Formation: Primary vs. Secondary Umbilical Vesicle
The yolk sac forms in two stages during weeks 2-3 of development:
Primary Umbilical Vesicle (Day 8-12)
- After implantation, cells from the hypoblast (lower layer of the bilaminar disc) migrate around the inside of the cytotrophoblast shell
- These cells form a thin membrane lining the blastocyst cavity, creating the primary umbilical vesicle
- The bilaminar disc - composed of epiblast (above) and hypoblast (below) - forms the roof of this vesicle
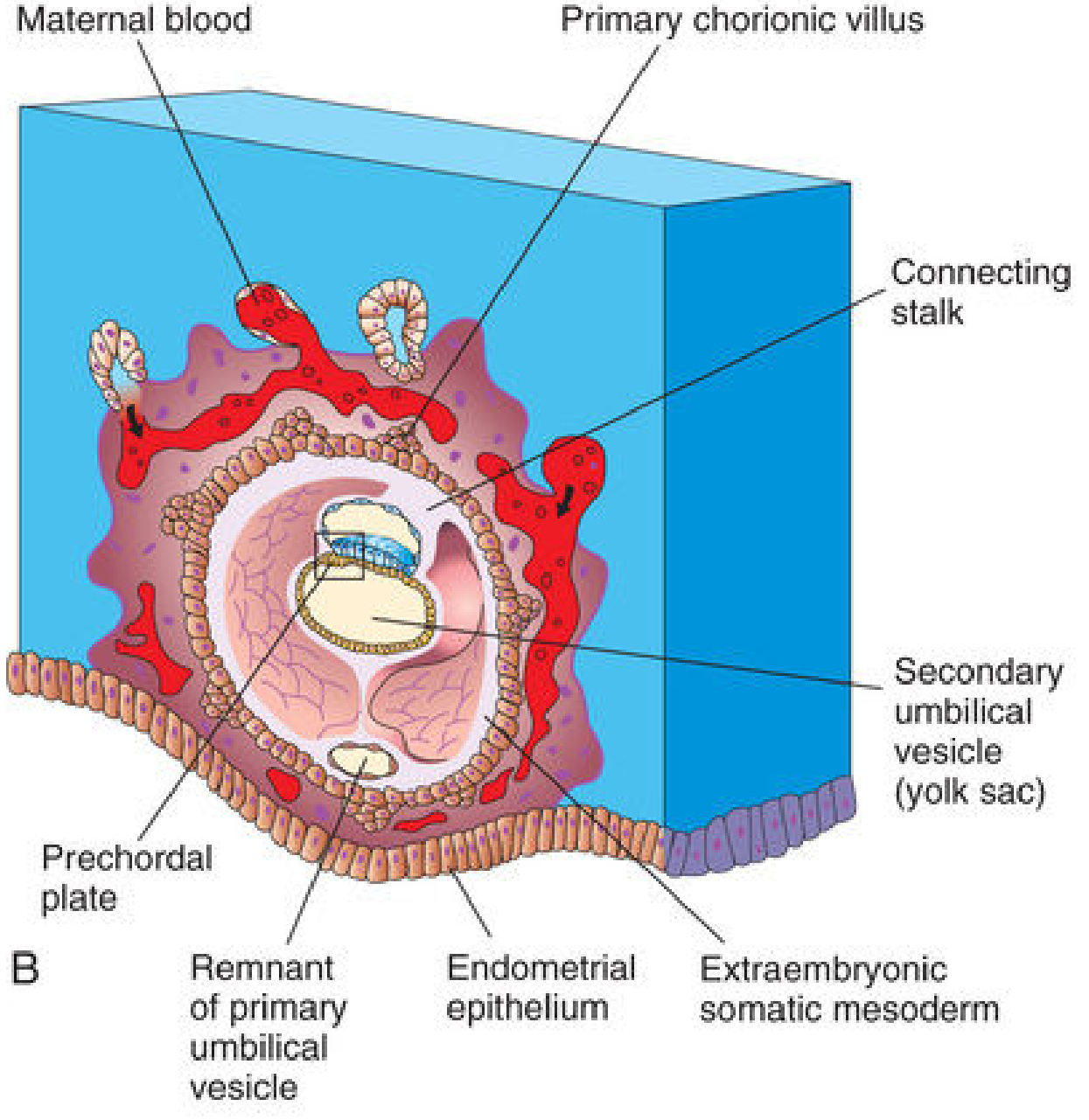
14-day embryo showing the secondary umbilical vesicle (yolk sac) and its relationship to the bilaminar disc - The Developing Human
Secondary Umbilical Vesicle (Day 13-14)
- As the extraembryonic coelom (chorionic cavity) forms and enlarges, it pinches and compresses the primary vesicle
- Extraembryonic endodermal cells migrating from the hypoblast form a smaller, secondary umbilical vesicle - this is what is commonly called "the yolk sac"
- A portion of the primary vesicle is pinched off and remains as a small remnant outside the secondary vesicle
- The secondary vesicle is surrounded by extraembryonic splanchnic mesoderm
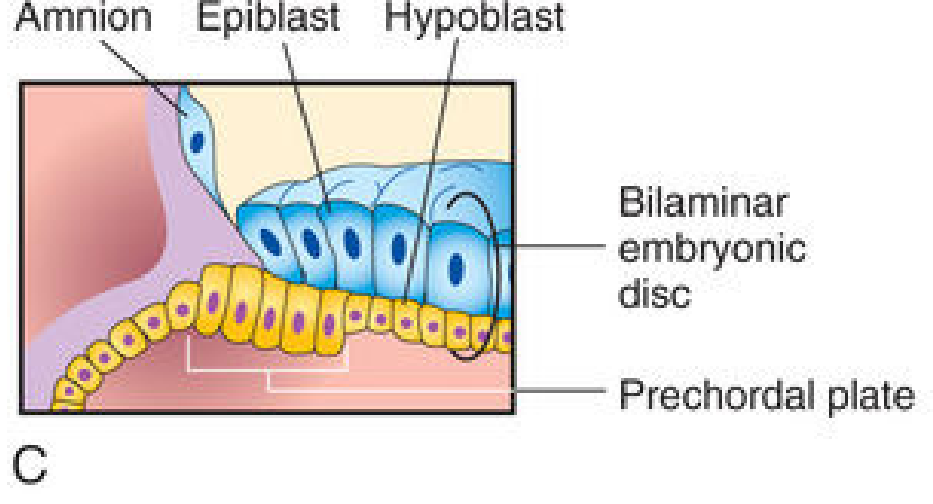
Bilaminar embryonic disc at 14 days - the hypoblast forms the roof of the secondary umbilical vesicle - The Developing Human
Structure
The secondary umbilical vesicle is suspended within the chorionic cavity (extraembryonic coelom) by the connecting stalk (future umbilical cord). Its wall has two layers:
- Inner layer: Extraembryonic endoderm (continuous with the embryonic endoderm)
- Outer layer: Extraembryonic splanchnic mesoderm
Functions of the Yolk Sac
The yolk sac is metabolically active and performs several essential roles, especially in the first trimester before the placenta is established:
| Function | Details |
|---|---|
| 1. Nutrition (early) | Absorbs and transfers nutrients from the trophoblast lacunae/coelomic cavity to the embryonic disc via selective processing |
| 2. Hematopoiesis | The first site of blood cell formation (weeks 3-6): blood islands in the yolk sac wall produce primitive erythrocytes; hematopoietic stem cells later migrate to liver, then spleen, then bone marrow |
| 3. Origin of primordial germ cells (PGCs) | PGCs arise in the wall of the yolk sac near the allantoic outpouching; they migrate via the mesentery of the hindgut to the developing gonads (weeks 4-6) |
| 4. Gut epithelium | The roof of the yolk sac is incorporated into the embryo during lateral folding, forming the primitive gut tube (foregut, midgut, hindgut) |
| 5. Vitelline (omphalomesenteric) duct | The narrow stalk connecting the yolk sac to the midgut (normally obliterates by week 6-7) |
| 6. Allantoic diverticulum | A finger-like outpouching of the yolk sac into the connecting stalk → precursor of the urinary bladder and umbilical vessels |
Fate of the Yolk Sac
- Gradually becomes smaller as the embryo grows and folds
- By week 6-7, the vitelline (omphalomesenteric) duct - which connects it to the gut - normally obliterates
- The yolk sac eventually becomes a small vestigial structure lying outside the embryo within the umbilical cord
- It is usually no longer detectable ultrasonographically after 12 weeks
Clinical Relevance of Yolk Sac Remnant
Meckel's Diverticulum - Failure of the vitelline duct to obliterate → a finger-like projection from the ileum (the most common congenital anomaly of the GI tract, occurring in ~2% of the population - the "rule of 2s": 2% incidence, within 2 feet of the ileocecal valve, 2 inches long, presents before age 2). May contain ectopic gastric or pancreatic tissue.
Vitelline fistula - Complete failure of duct obliteration → open fistula between ileum and umbilicus (meconium or intestinal contents at the umbilicus).
Enterocystoma (vitelline cyst) - Partial obliteration → cyst along the path of the duct.
Yolk sac tumors (Endodermal sinus tumors) - Malignant germ cell tumors derived from primitive yolk sac cells; produce AFP (alpha-fetoprotein) as a tumor marker; most common in sacrococcygeal region and gonads of children.
Ultrasonographic Significance
- The secondary yolk sac is visible on transvaginal ultrasound as early as 5 weeks' gestation - the first structure identified within the gestational sac
- A visible yolk sac confirms an intrauterine pregnancy
- Abnormal yolk sac (too large >6mm, too small, irregular shape, or absent) is associated with early pregnancy failure/miscarriage
- The yolk sac and the embryo/fetal heartbeat together are the key first-trimester ultrasound landmarks
PART 2: TWIN PREGNANCY
Incidence and Classification
Multiple pregnancies are classified primarily by zygosity (how many fertilized eggs) and chorionicity (how many placentas/chorionic sacs).
Overall twin incidence: ~1 in 80 spontaneous pregnancies (rising with IVF/ART use)
Two fundamental types:
| Type | Also called | Origin | Genetics |
|---|---|---|---|
| Dizygotic (DZ) | Fraternal twins | 2 separate oocytes fertilized by 2 sperm | Not genetically identical; like any siblings (share ~50% genes) |
| Monozygotic (MZ) | Identical twins | 1 oocyte fertilized by 1 sperm → single zygote splits | Genetically identical |
Frequency: ~2/3 of twins are DZ; ~1/3 are MZ.
Dizygotic (DZ) Twins
DZ twins result from polyovulation - two oocytes released in one cycle and fertilized by two different sperms. They develop from two independent zygotes.
Key features:
- Always dichorionic - diamniotic (two separate chorionic and amniotic sacs)
- Placentas may be separate or fused (secondary fusion after close implantation)
- May be same sex or opposite sex
- No more genetically alike than any two siblings
Racial/familial frequency:
- Asian populations: ~1 in 500
- White populations: ~1 in 125
- Some African populations: ~1 in 20
- Hereditary tendency - recurrence ~3x that of general population; influenced by mother's genotype (not father's)
- Associated with: advanced maternal age, multiparity, gonadotropin-stimulating drugs (clomiphene), ART/IVF
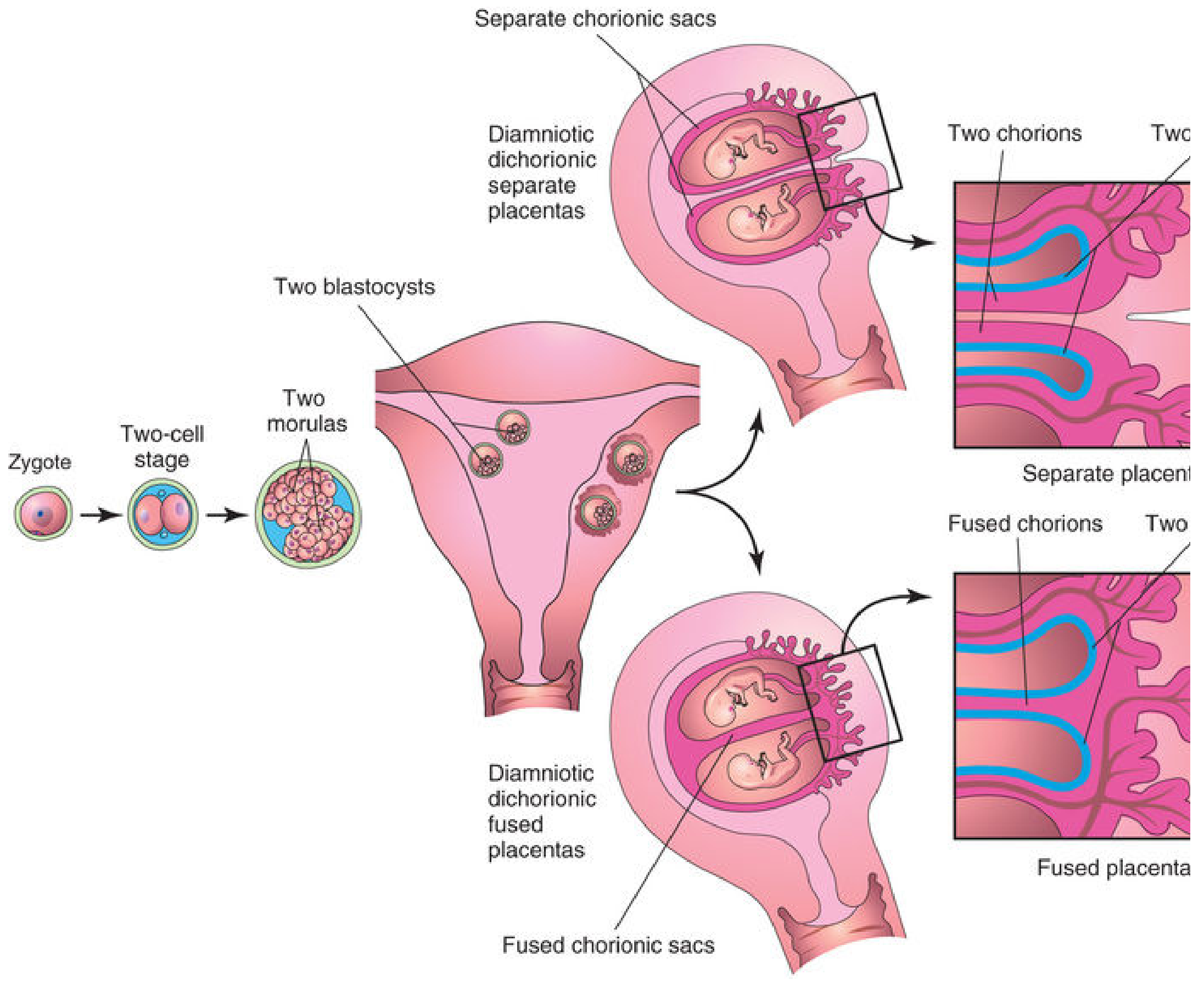
DZ twinning: two blastocysts, always dichorionic; placentas may be separate or fused - The Developing Human
Monozygotic (MZ) Twins
MZ twins arise from a single fertilized egg that splits at some point during early development. The timing of the split determines the chorionicity and amnionicity - this is the most important classification for clinical management and risk.
MZ Twin Types Based on Timing of Split
| Timing of division | Age of embryo | Result | Frequency |
|---|---|---|---|
| Days 1-3 (2-cell to morula) | Before inner cell mass forms | Dichorionic-Diamniotic (DCDA) - two chorions, two amnions, two placentas (may fuse) | ~35% of MZ twins |
| Days 4-8 (blastocyst stage, inner cell mass divides) | After trophoblast differentiated, before amnion | Monochorionic-Diamniotic (MCDA) - one chorion, two amnions, shared placenta | ~65% of MZ twins - MOST COMMON |
| Days 8-13 (after amnion has formed) | After amnion differentiated | Monochorionic-Monoamniotic (MCMA) - one chorion, one amnion, shared placenta | ~1% of MZ twins |
| After day 13 (embryonic disc forms but divides incompletely) | After primitive streak appears | Conjoined twins | ~1:50,000-100,000 births |
Membrane Structure Summary Table
| Feature | DZ Twins | MZ-DCDA | MZ-MCDA | MZ-MCMA |
|---|---|---|---|---|
| Chorions | 2 | 2 | 1 | 1 |
| Amnions | 2 | 2 | 2 | 1 |
| Placentas | 2 (or fused) | 2 (or fused) | 1 (shared) | 1 (shared) |
| Dividing membrane | Thick (4 layers) | Thick (4 layers) | Thin (2 layers) | None |
| Risk of TTTS | None | Very low | High (10-15%) | High |
| Cord entanglement | No | No | No | Yes |
Frequency of placental types (The Developing Human table):
- MZ: 1% monoamniotic-monochorionic; 64% diamniotic-monochorionic; 25% fused placentas; 10% separate placentas
- DZ: 40% fused placentas; 60% separate placentas
Clinical Complications of Twin Pregnancy
1. Twin-to-Twin Transfusion Syndrome (TTTS)
- Occurs in 10-15% of monochorionic-diamniotic (MCDA) twins
- Caused by unidirectional arteriovenous anastomoses in the shared placenta - arterial blood from one twin shunts into the venous circulation of the other
- Donor twin: small, pale, anemic, oligohydramnios, IUGR
- Recipient twin: large, polycythemic, polyhydramnios, cardiac overload, risk of congestive heart failure
- Placenta: pale portion (donor) vs. dark red (recipient)
- Treatment: Fetoscopic laser coagulation of placental vascular anastomoses (gold standard)
- Lethal if untreated in severe cases: anemia → death of donor; CCF → death of recipient
2. Cord Entanglement (MCMA twins)
- Monoamniotic twins share one amniotic sac → umbilical cords can intertwine
- Fetal mortality rates increased by up to 10% due to cord compression/interruption
- Management: close ultrasound surveillance; often planned delivery at 34 weeks
3. IUGR and Growth Discordance
- One twin may be significantly smaller, especially in MCDA twins
- Growth discordance >20% weight difference is clinically significant
4. Conjoined Twins
- Arise from incomplete division of the embryonic disc after day 13
- Named by site of union:
| Type | Union site | Frequency |
|---|---|---|
| Thoracopagus | Anterior thorax | Most common (~40%) |
| Omphalopagus | Anterior abdomen/umbilicus | ~33% |
| Pygopagus | Posterior pelvis/sacrum | ~18% |
| Craniopagus | Cranium | ~2% |
- Incidence: ~1 in 50,000-100,000 births
- Parasitic (heteropagus) twins (1:1,000,000): severely defective twin is attached to and dependent on the cardiovascular system of the complete twin
5. Anastomosis and Erythrocyte Mosaicism (DZ twins)
- In DZ twins with fused placentas, vascular anastomoses may result in erythrocyte mosaicism - each twin has two red blood cell populations with different blood groups
- Unlike in cattle, female DZ twins with a male co-twin do not develop masculinization (no freemartin effect in humans)
6. Discordance in MZ Twins
Despite being genetically identical, MZ twins can be discordant for disease due to:
- Somatic mutations post-zygotic splitting
- Uneven X-chromosome inactivation (lyonization) in female MZ twins
- Epigenetic differences
- Vascular abnormalities during development
- Chromosome aberrations originating in one blastocyst after the split
7. Early Death of a Twin ("Vanishing Twin")
- One twin dies early in pregnancy and is resorbed
- Common - seen on early ultrasound but not at delivery
- Clinical concern: if CVS or amniocentesis samples extraembryonic tissue from the resorbed twin, prenatal cytogenetic results may not match the live-born infant's karyotype
Determining Zygosity
Chorionicity ≠ zygosity. Importantly:
- All DZ twins are dichorionic, but ~35% of MZ twins are also dichorionic
- A dichorionic placenta cannot rule out MZ twinning
- Definitive zygosity determination: DNA molecular markers (any two non-MZ individuals will show differences in a large panel of DNA markers)
- Same sex, monochorionic → almost certainly MZ
- Opposite sex → always DZ
Why it matters: MZ twin zygosity is important for:
- Kidney/bone marrow organ transplantation (MZ twins are ideal donors)
- Risk counseling for genetic conditions
- Understanding disease concordance/discordance
Superfecundation and Superfetation
- Superfecundation: Fertilization of two oocytes by two different sperms (possibly from different fathers) at different times within the same ovulatory cycle. DZ twins with different fathers have been confirmed by genetic markers.
- Superfetation: Fertilization at different times in different menstrual cycles - extremely rare in humans; would require two implantations at different developmental stages in the same uterus.
Sources: The Developing Human: Clinically Oriented Embryology (Moore et al.); Langman's Medical Embryology (Sadler); Creasy & Resnik's Maternal-Fetal Medicine; Robbins Pathologic Basis of Disease; Costanzo Physiology 7th Edition
implantation
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Finding Sources
Loading Image
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
I now have comprehensive content from multiple authoritative sources. Here is the complete detailed answer.
Implantation
Definition and Timing
Implantation is the process by which the blastocyst embeds itself into the endometrium of the uterus. It begins at approximately day 6-7 after fertilization and is fully completed by the end of the second week (day 14). It is the event that establishes the physical connection between the embryo and the mother, initiating the uteroplacental circulation.
Normal implantation site: posterior wall of the upper body of the uterus (most commonly the posterior superior wall, close to the midline).
- The Developing Human: Clinically Oriented Embryology, Langman's Medical Embryology
Prerequisites for Implantation
Before the blastocyst can implant, two things must occur simultaneously:
1. Blastocyst Activation ("Hatching")
- After reaching the uterine cavity at day 4-5, the blastocyst must hatch from the zona pellucida
- Zona pellucida is dissolved by proteolytic enzymes (strypsin) secreted by the blastocyst
- Hatching exposes the trophoblast directly to the endometrial surface
- The blastocyst orients itself with the embryoblast (inner cell mass) pole - the polar trophoblast - facing the endometrium
2. Endometrial Receptivity - "Window of Implantation"
- The endometrium is only receptive for a brief 2-3 day window in the mid-luteal phase (days 20-24 of a 28-day cycle)
- This window is created by the synergistic action of progesterone (P4) and estradiol (E2) from the corpus luteum
- Progesterone triggers:
- Cessation of endometrial proliferation
- Transformation of stromal cells into large secretory decidual cells (decidualization)
- Influx of specialized immune cells (uterine NK cells, macrophages)
- Expression of surface adhesion molecules and signaling molecules
Key molecular mediators of receptivity:
| Molecule | Source | Role |
|---|---|---|
| HB-EGF (heparin-binding EGF) | Endometrial epithelium (pinopodia) | Critical for blastocyst attachment; binds ErbB1/ErbB4 receptors on polar trophoblast |
| LIF (Leukemia inhibitory factor) | Endometrial epithelium | Signals to blastocyst; essential for uterine receptivity |
| Integrins | Endometrial epithelium | Cell adhesion molecules; bind extracellular matrix |
| Pinopodes | Endometrial surface | Microscopic surface projections that appear only during the window of implantation; facilitate blastocyst-endometrium contact |
| BMPs | Endometrium | Expressed during implantation window; essential for fertilization and implantation |
| COX-2/Prostaglandins | Endometrial stroma | Induce angiogenesis; COX-2 regulated by P4 and hCG |
| HOXA10, HOXA11 | Endometrial epithelium | Transcription factors essential for endometrial receptivity |
| Wnt signaling | Endometrial epithelium | Required for attachment |
- Creasy & Resnik's Maternal-Fetal Medicine
Stages of Implantation: Day-by-Day Sequence
Day 6-7: Apposition and Initial Adhesion
- The zona-free blastocyst loosely appositions itself to the endometrial epithelium
- The polar trophoblast (over the ICM) aligns with the luminal epithelium
- This is a non-firm, reversible contact
Day 8: Adhesion and Early Invasion
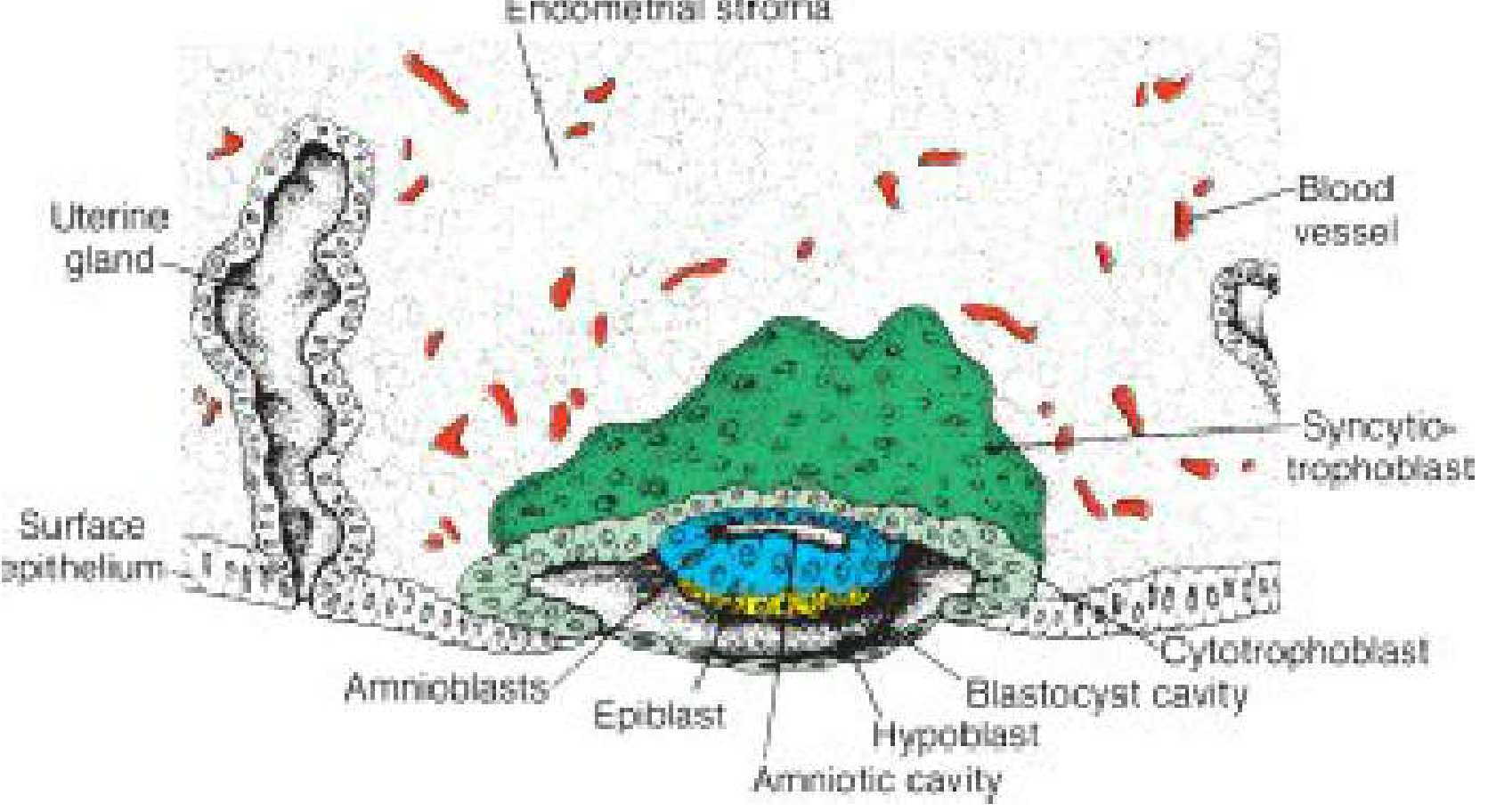
8-day blastocyst partially embedded in endometrial stroma, showing cytotrophoblast and syncytiotrophoblast differentiation - Langman's Medical Embryology
At day 8, the trophoblast differentiates into two distinct layers:
1. Cytotrophoblast (inner layer)
- Single layer of mononucleated cells
- Mitotically active - cells divide and migrate outward into the syncytiotrophoblast
- Trophoblast fusion regulated by the cyclic AMP pathway
- Source of new cells for syncytiotrophoblast
2. Syncytiotrophoblast (outer layer)
- Rapidly expanding multinucleated mass with no cell boundaries
- Formed by fusion of cytotrophoblast cells (which lose their individual membranes)
- No mitotic figures in syncytiotrophoblast - it grows only by incorporation of new cytotrophoblast cells
- Actively secretes enzymes that digest and invade the endometrial connective tissue
- Produces hCG (human chorionic gonadotropin)
Simultaneously within the embryoblast:
- Two layers form: epiblast (tall columnar cells, facing amnion) and hypoblast (cuboidal cells, facing blastocyst cavity)
- A small slit - the primordium of the amniotic cavity - appears within the epiblast
- Amnioblasts (epiblast cells adjacent to the cytotrophoblast) line the forming amniotic cavity
The endometrial stroma adjacent to the implantation site becomes edematous and highly vascular.
Day 9: Lacunar Stage
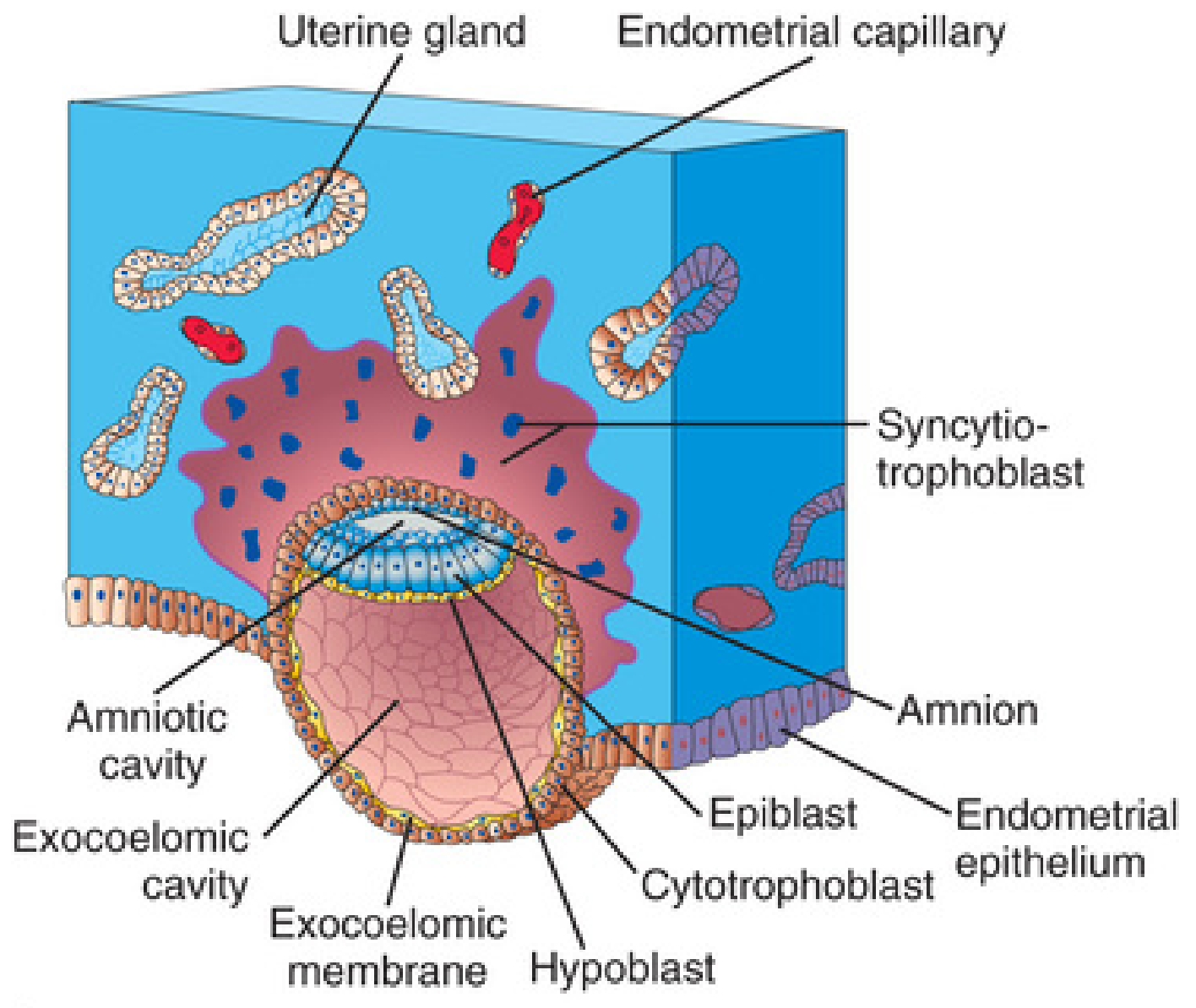
9-day blastocyst showing the lacunar stage and exocoelomic membrane formation - The Developing Human
- The blastocyst is more deeply embedded in the endometrium
- The surface epithelium defect is closed by a fibrin coagulum (closing plug)
- Vacuoles appear in the syncytiotrophoblast at the embryonic pole → fuse to form lacunae (spaces)
- This marks the lacunar stage of trophoblast development
- Cells from the hypoblast migrate to line the inside of the cytotrophoblast, forming the exocoelomic (Heuser) membrane → together with the hypoblast, this forms the primitive umbilical vesicle (primary yolk sac)
Days 11-12: Uteroplacental Circulation Established
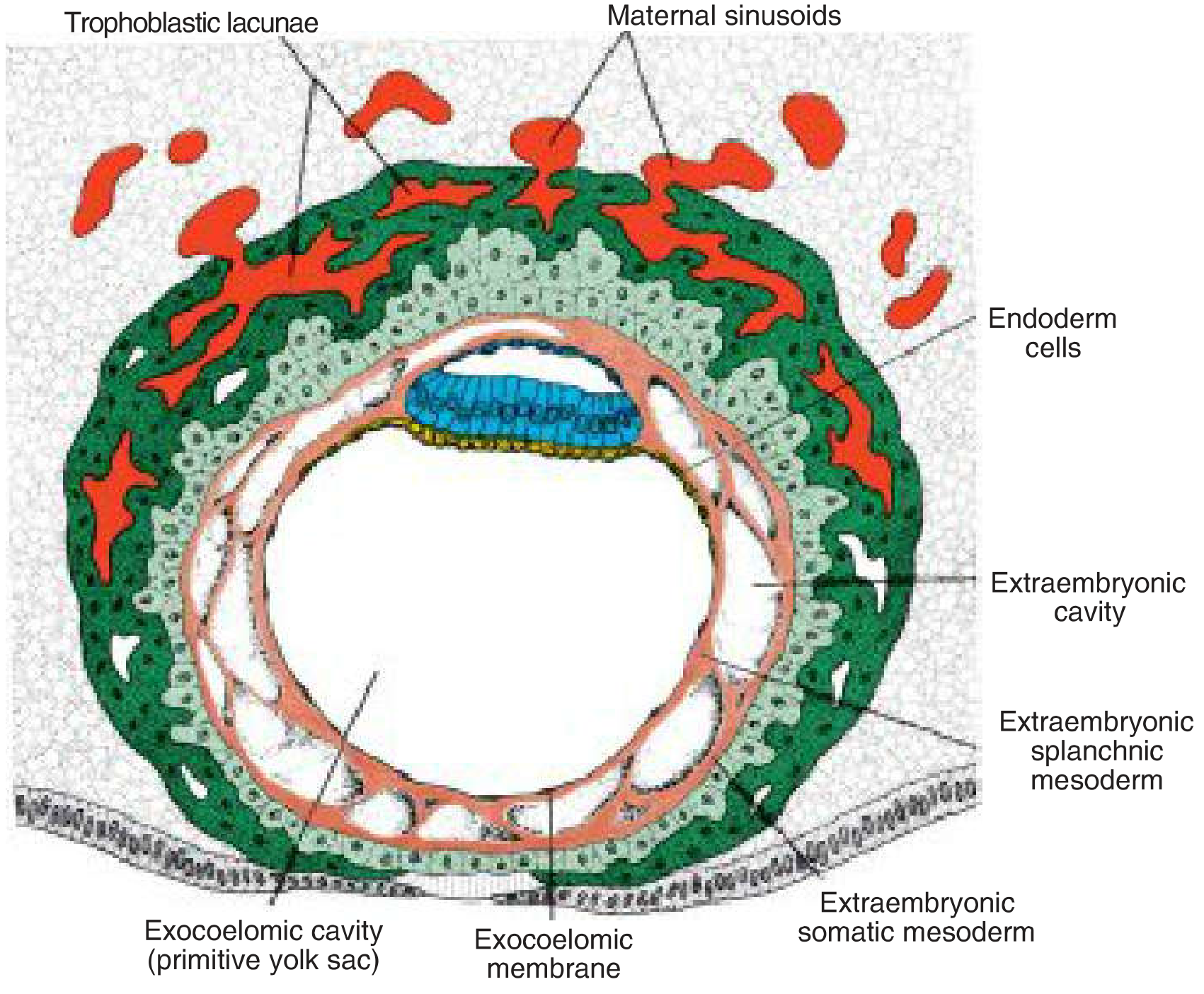
12-day blastocyst with trophoblastic lacunae connecting to maternal sinusoids, establishing uteroplacental circulation - Langman's Medical Embryology
Key events at days 11-12:
- Blastocyst is completely embedded in endometrial stroma; surface epithelium nearly fully covers the original defect
- Syncytiotrophoblast penetrates deeper into stroma and erodes the endothelial lining of maternal capillaries
- Maternal capillaries become engorged → called sinusoids
- Syncytial lacunae become continuous with sinusoids → maternal blood flows freely into the lacunar system → establishes the uteroplacental circulation
- Extraembryonic mesoderm forms from cells between the exocoelomic membrane and inner trophoblast; extraembryonic coelomic spaces begin to appear within it
- The syncytiotrophoblast begins eroding endometrial glands → glycogen-rich secretions flood the lacunae, providing early nutrition to the embryo
- Decidual reaction in the endometrium: stromal cells accumulate glycogen and lipids, become polyhedral (decidual cells); later spreads throughout the entire endometrium
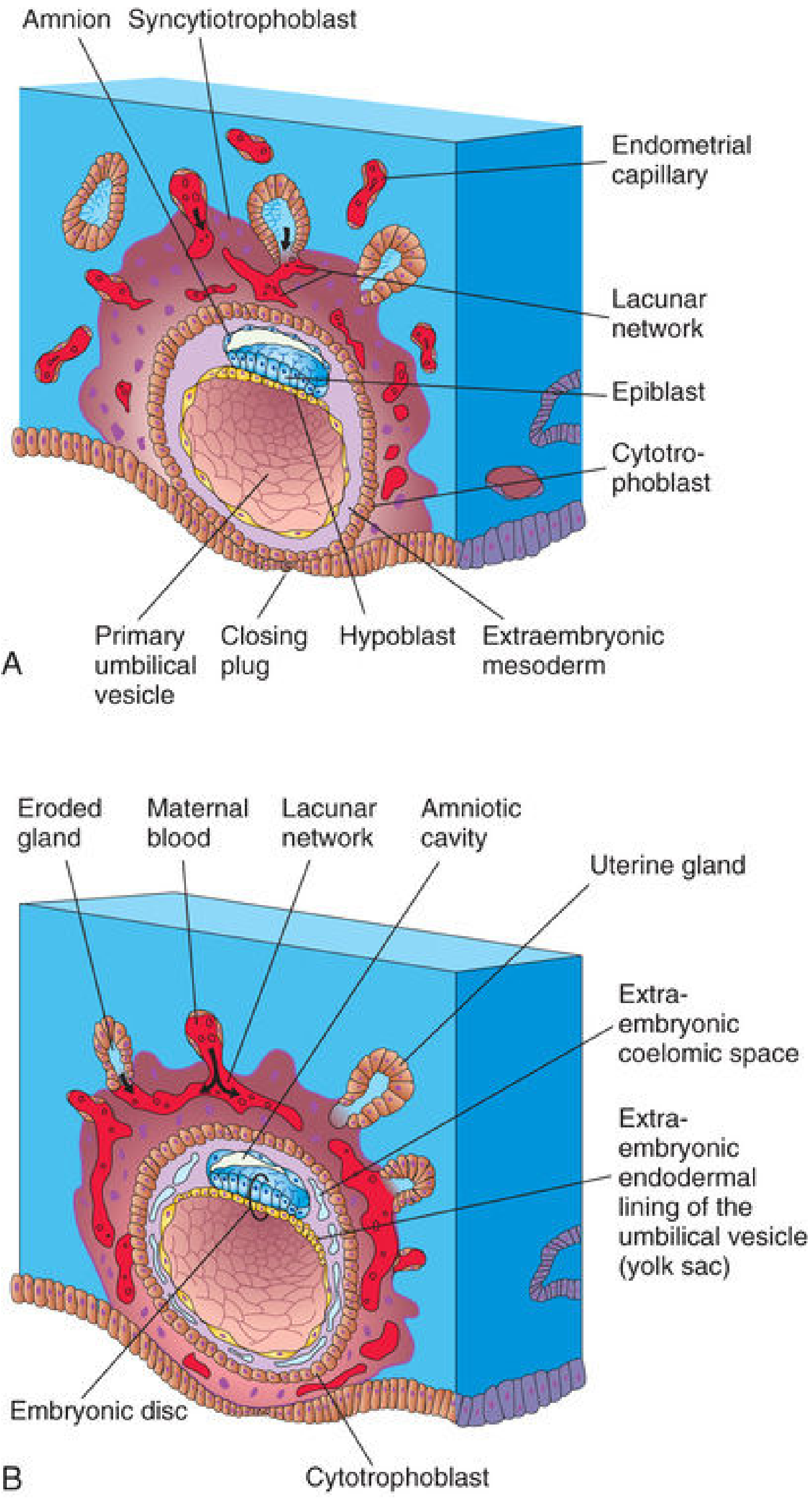
Comparison of 10-day (A) and 12-day (B) implanted embryos showing progressive invasion and lacunar network formation - The Developing Human
Day 13: Completion of Implantation
At day 13:
- Surface defect in endometrium has healed completely
- Occasional bleeding from increased blood flow into lacunae may occur around day 28, potentially confused with menstruation → can cause inaccuracy in estimated delivery date
- Cytotrophoblast cells proliferate locally and penetrate into syncytiotrophoblast → form cellular columns surrounded by syncytium → primary chorionic villi (first stage in placenta development)
- Secondary yolk sac forms (definitive yolk sac); the primary yolk sac is largely pinched off and leaves a remnant
- Extraembryonic coelomic spaces fuse to form the extraembryonic coelom (chorionic cavity)
- The connecting stalk forms - suspending the embryo, amnion, and yolk sac within the chorionic sac
hCG and the Rescue of the Corpus Luteum
The syncytiotrophoblast begins producing hCG (human chorionic gonadotropin) from the moment it forms. This is physiologically critical:
- hCG enters maternal blood via the lacunar system
- It rescues the corpus luteum from regression, which would otherwise occur at day 23-24 (without pregnancy)
- The corpus luteum continues secreting progesterone and estrogen → maintains the endometrium and prevents menstruation
- hCG levels rise exponentially in early pregnancy, doubling every 48-72 hours → forms the basis of urine and blood pregnancy tests
- Enough hCG is produced by end of week 2 to give a positive pregnancy test, even before the woman knows she is pregnant
Molecular Summary of the Implantation Sequence
| Step | Process | Key Molecules |
|---|---|---|
| Pre-implantation | Zona hatching | Strypsin, embryonic proteases |
| Apposition | Loose contact | Pinopodia, HB-EGF |
| Adhesion | Firm attachment of polar TE to epithelium | Integrins, LIF, HB-EGF/ErbB1/ErbB4 |
| Invasion | Syncytiotrophoblast invades stroma | Matrix metalloproteinases (MMPs), endometrial apoptosis |
| Decidualization | Stromal transformation | Progesterone, prolactin, IGFBP-1, COX-2 |
| Nutrition | Glandular secretions, maternal blood in lacunae | Glycogen, lipids |
| Signaling | Corpus luteum rescue | hCG |
Normal vs. Abnormal Implantation Sites
Normal Site
- Posterior wall of upper body of uterus, close to midline (most common)
- Anterior wall also acceptable
Low Implantation → Placenta Previa
- Blastocyst implants in the lower uterine segment
- As the placenta grows, it overlies the internal cervical os → placenta previa
- Presents with painless antepartum hemorrhage; may require cesarean delivery
Abnormal Implantation Sites → Ectopic Pregnancy
Ectopic pregnancy = implantation outside the endometrial cavity. Incidence: ~2% of all pregnancies.
Sites (in order of frequency):
| Site | Frequency | Notes |
|---|---|---|
| Ampulla of uterine tube | ~70% of all ectopics | Most common; may rupture at 6-8 weeks |
| Isthmus of uterine tube | ~12% | Narrow, unexpandable → ruptures early with heavy bleeding (rich anastomosis between ovarian and uterine vessels) |
| Fimbriae | ~11% | May be expelled into peritoneal cavity |
| Interstitial/Cornual (intramural) | ~2-3% | May develop beyond 8 weeks before expulsion; rupture is profuse |
| Ovary | ~1% | Ovarian pregnancy |
| Abdominal/Peritoneal | ~1% | Implants in rectouterine pouch or on abdominal organs; risk of maternal death 90× intrauterine pregnancy; rarely survives to term |
| Cervix | Rare | Placenta attaches to cervical fibromuscular tissue; severe bleeding, may require hysterectomy |
Risk factors for ectopic pregnancy:
- Previous ectopic pregnancy (highest risk)
- Pelvic inflammatory disease (PID) - tubal scarring/adhesions
- Endometriosis
- Previous tubal surgery
- In utero DES exposure
- IVF/ART (incidence ~3/1000)
- IUCD (intrauterine contraceptive device)
Clinical presentation: Amenorrhoea, positive hCG, lower abdominal pain (unilateral), vaginal bleeding. Rupture → peritonism, hemodynamic shock.
Management:
- No embryo heartbeat + diameter <3 cm: methotrexate (1-2 oral/IM doses)
- Rupture or failed medical treatment: salpingectomy / salpingostomy (surgical)
- Heterotopic pregnancy (simultaneous intrauterine + ectopic): surgical removal of ectopic tube without disturbing the intrauterine pregnancy
The Decidua
The entire endometrium becomes the decidua after implantation. It is divided into three regions based on relation to the implanting embryo:
| Region | Location | Function |
|---|---|---|
| Decidua basalis | Between the embryo and myometrium | Forms the maternal part of the placenta |
| Decidua capsularis | Covers the embryo on the luminal side | Stretches as embryo grows; fuses with decidua parietalis by week 12 |
| Decidua parietalis | Lines the rest of the uterine cavity | Fuses with capsularis by week 12, obliterating the uterine cavity |
Decidual cells: Large, glycogen-rich polyhedral cells that protect the myometrium from invasion and provide nutrition to the early embryo via histiotrophic nutrition.
Summary Timeline
| Day | Event |
|---|---|
| Day 0 | Fertilization |
| Day 4-5 | Blastocyst enters uterine cavity |
| Day 5-6 | Zona pellucida hatches |
| Day 6-7 | Apposition of blastocyst to endometrium |
| Day 8 | Firm adhesion; cytotrophoblast and syncytiotrophoblast differentiate; amniotic cavity appears; bilaminar disc (epiblast + hypoblast) forms |
| Day 9 | Lacunar stage; exocoelomic membrane and primary yolk sac form; surface sealed by fibrin plug |
| Days 11-12 | Lacunae connect with maternal sinusoids → uteroplacental circulation begins; decidual reaction spreads |
| Day 13 | Complete embedding; primary chorionic villi; secondary yolk sac; extraembryonic coelom |
| End of week 2 | hCG levels sufficient for positive pregnancy test |
Sources: The Developing Human: Clinically Oriented Embryology (Moore et al.); Langman's Medical Embryology (Sadler); Creasy & Resnik's Maternal-Fetal Medicine; Medical Physiology (Boron & Boulpaep)
This is a shared conversation. Sign in to Orris to start your own chat.