Extraocular muscles
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Loading Image
Loading Image
I now have comprehensive content from multiple authoritative sources. Let me compile the full answer.
Extraocular Muscles
There are six extraocular muscles for each eye. They control all rotational movements of the globe and are innervated by three cranial nerves (CN III, IV, VI). Together they form one of the most precisely coordinated motor systems in the body.
Anatomy Overview
The globe is a sphere sitting in the bony orbit. Eye movements are pure rotations described along three axes that intersect at the center of the eyeball:
- Z axis (vertical) - horizontal movements (left/right)
- X axis (horizontal) - vertical movements (up/down)
- Y axis (sagittal) - torsional movements (intorsion/extorsion)
The orbital axis forms a 23° angle with the visual axis when the eye is in the primary position (looking straight ahead). This angular offset is what gives the vertical recti and obliques their subsidiary (secondary/tertiary) actions.
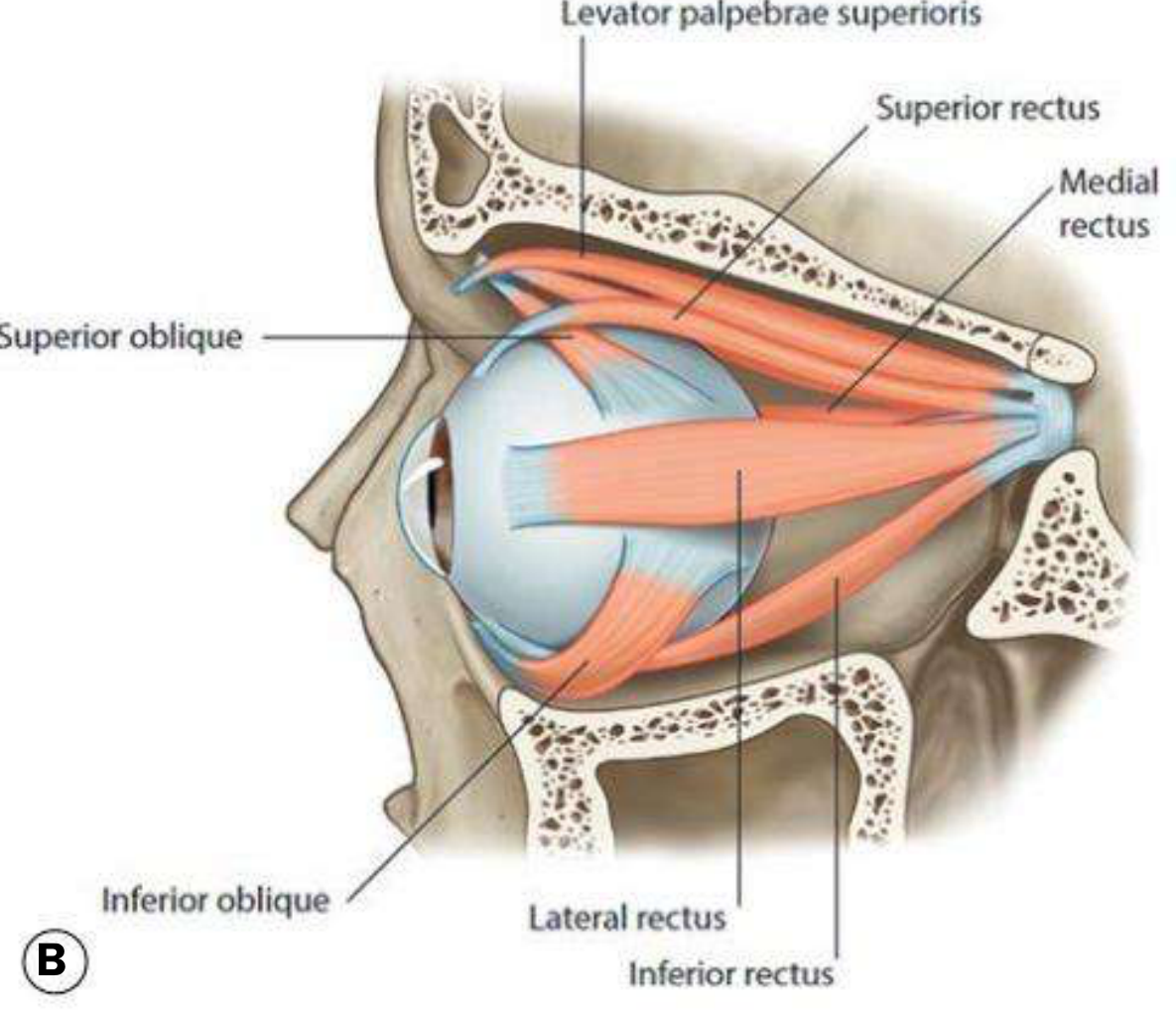
The Six Muscles
Rectus Muscles (4)
All four recti originate from the annulus of Zinn (common tendinous ring) at the orbital apex and insert anterior to the equator of the globe.
| Muscle | Insertion (from limbus) | Primary action | Secondary actions |
|---|---|---|---|
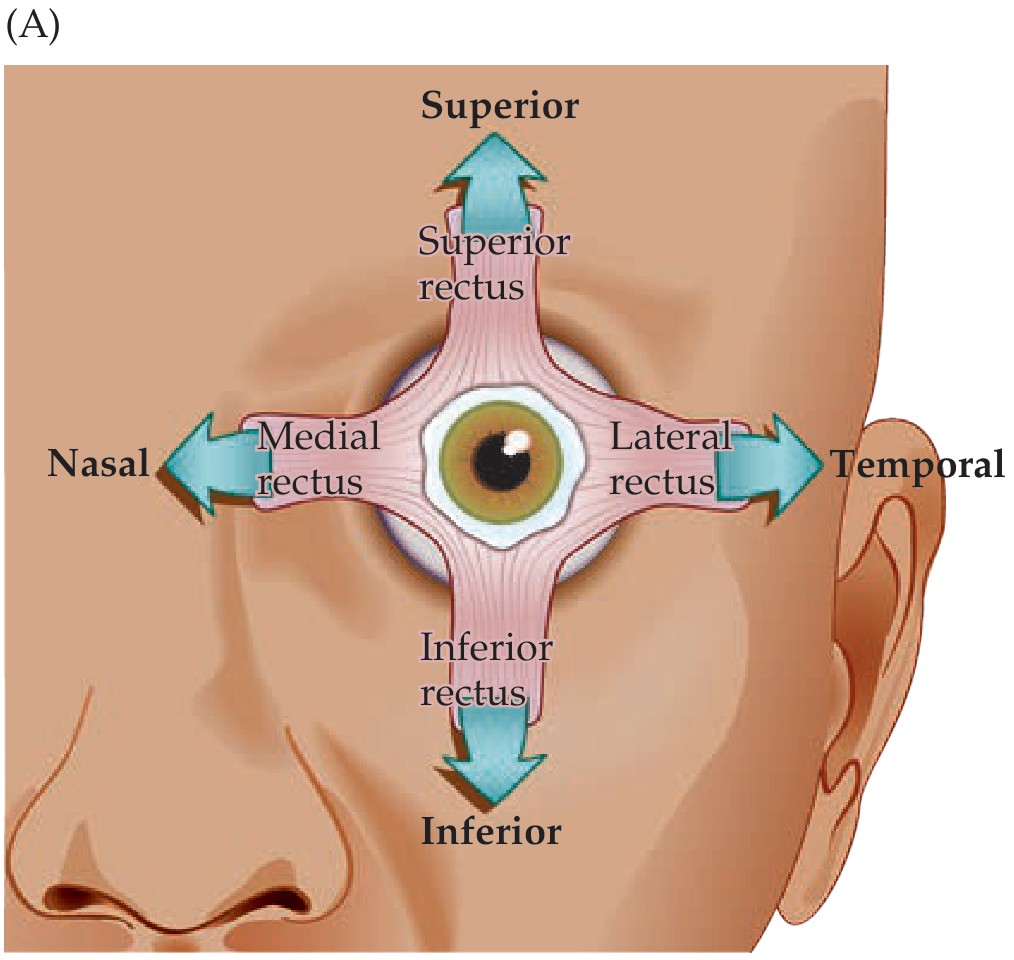
| Medial rectus | 5.5 mm (nasal) | Adduction | None in primary position |
| Lateral rectus | 6.9 mm (temporal) | Abduction | None in primary position |
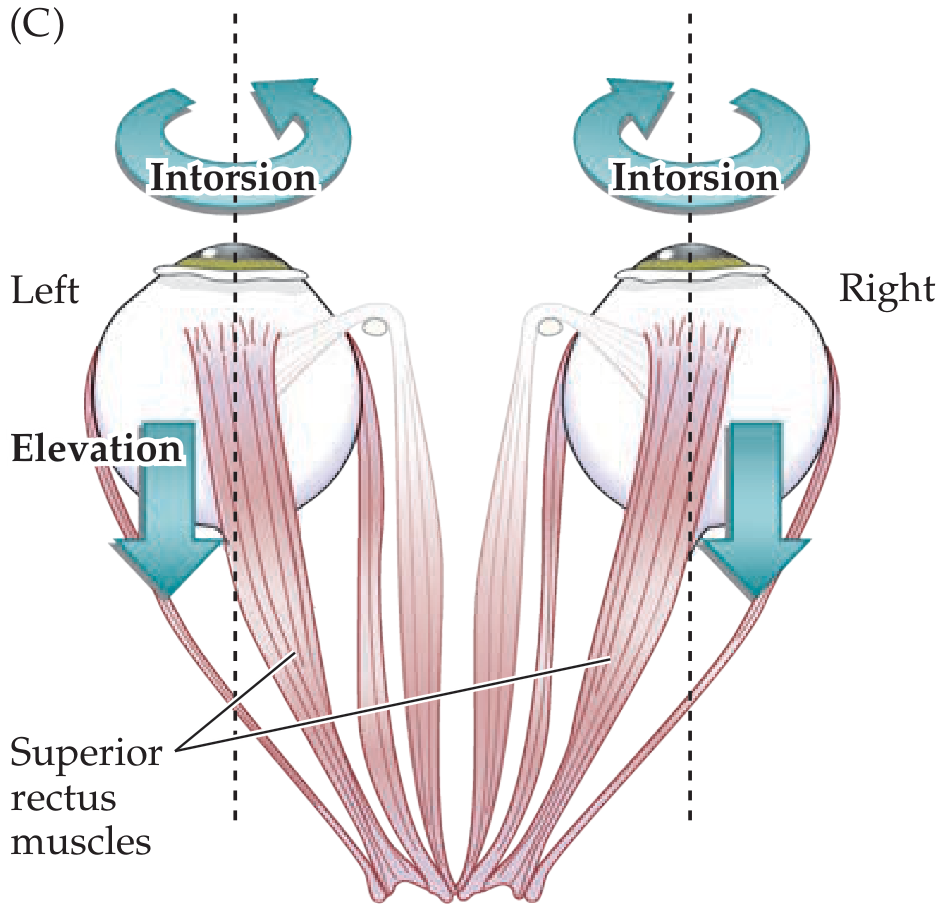
| Superior rectus | 7.7 mm (superior) | Elevation | Adduction, Intorsion |
| Inferior rectus | 6.5 mm (inferior) | Depression | Adduction, Extorsion |
The horizontal recti are pure horizontal movers with no secondary actions in the primary position because they lie exactly along the horizontal plane. The vertical recti, running along the orbital axis (23° from the visual axis), also produce adduction and torsion.
Testing tip: To isolate the superior rectus as a pure elevator, abduct the eye 23° so the visual axis aligns with the orbital axis - this eliminates all secondary actions.
The Spiral of Tillaux
The insertions of the four recti lie progressively further from the limbus in a spiral pattern: MR (5.5 mm) → IR (6.5 mm) → LR (6.9 mm) → SR (7.7 mm). This is a key surgical landmark during strabismus surgery.
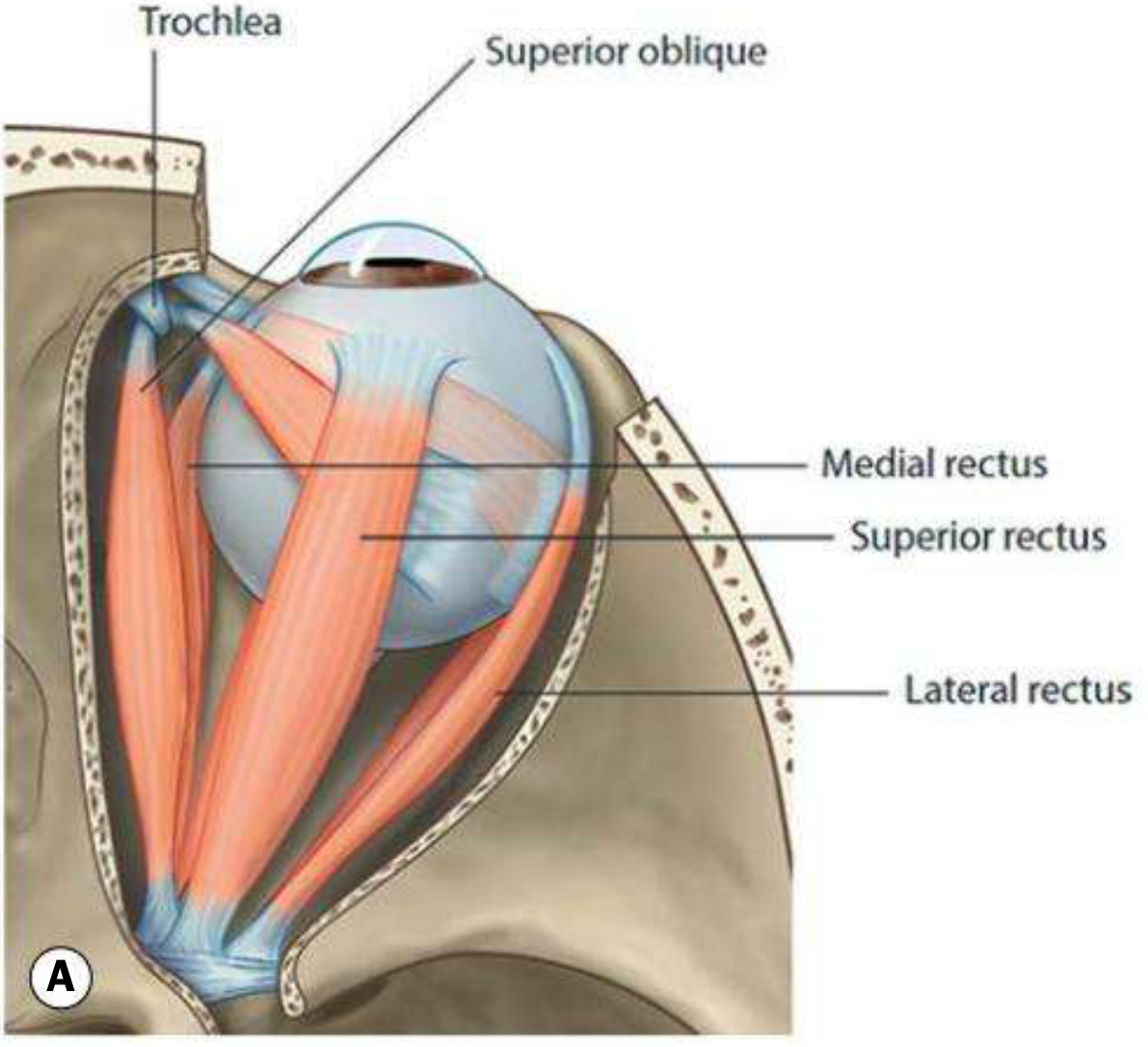
Oblique Muscles (2)
The obliques insert behind the equator and form an angle of 51° with the visual axis.
| Muscle | Origin | Special feature | Primary action | Secondary actions |
|---|---|---|---|---|
| Superior oblique | Superomedial to optic foramen | Passes through the trochlea (fibrocartilaginous pulley on the superomedial orbital rim), then inserts on the posterior superior temporal quadrant | Intorsion | Depression, Abduction |
| Inferior oblique | Anterior medial orbital floor (lateral to lacrimal sac) | No trochlea; inserts on posterior inferior temporal quadrant (near macula) | Extorsion | Elevation, Abduction |
Key clinical point: Although the superior oblique has an abducting action in primary position, its weakness is most apparent as failure to depress in adduction (the position where its visual axis aligns with its line of pull at 51° of adduction, making it a pure depressor). This is the standard test position for CN IV palsy.
Agonist-antagonist pairs (Sherrington's law):
- Medial rectus (adduction) ↔ Lateral rectus (abduction)
- Superior rectus (elevation) ↔ Inferior rectus (depression)
- Superior oblique (intorsion/depression) ↔ Inferior oblique (extorsion/elevation)
Muscle Pulleys
The four rectus muscles pass through condensations of connective tissue and smooth muscle just posterior to the equator. These pulleys act as the functional (effective) origins of the muscles. They minimize unwanted vertical movement of the medial/lateral recti during upgaze/downgaze and minimize horizontal movement of the superior/inferior recti during lateral gaze. Pulley displacement is a cause of "A- and V-pattern" strabismus and sagging eye syndrome.
Nerve Supply
Three cranial nerves innervate the six muscles. They pass through the cavernous sinus and enter the orbit via the superior orbital fissure.
| Nerve | Nucleus location | Muscles innervated |
|---|---|---|
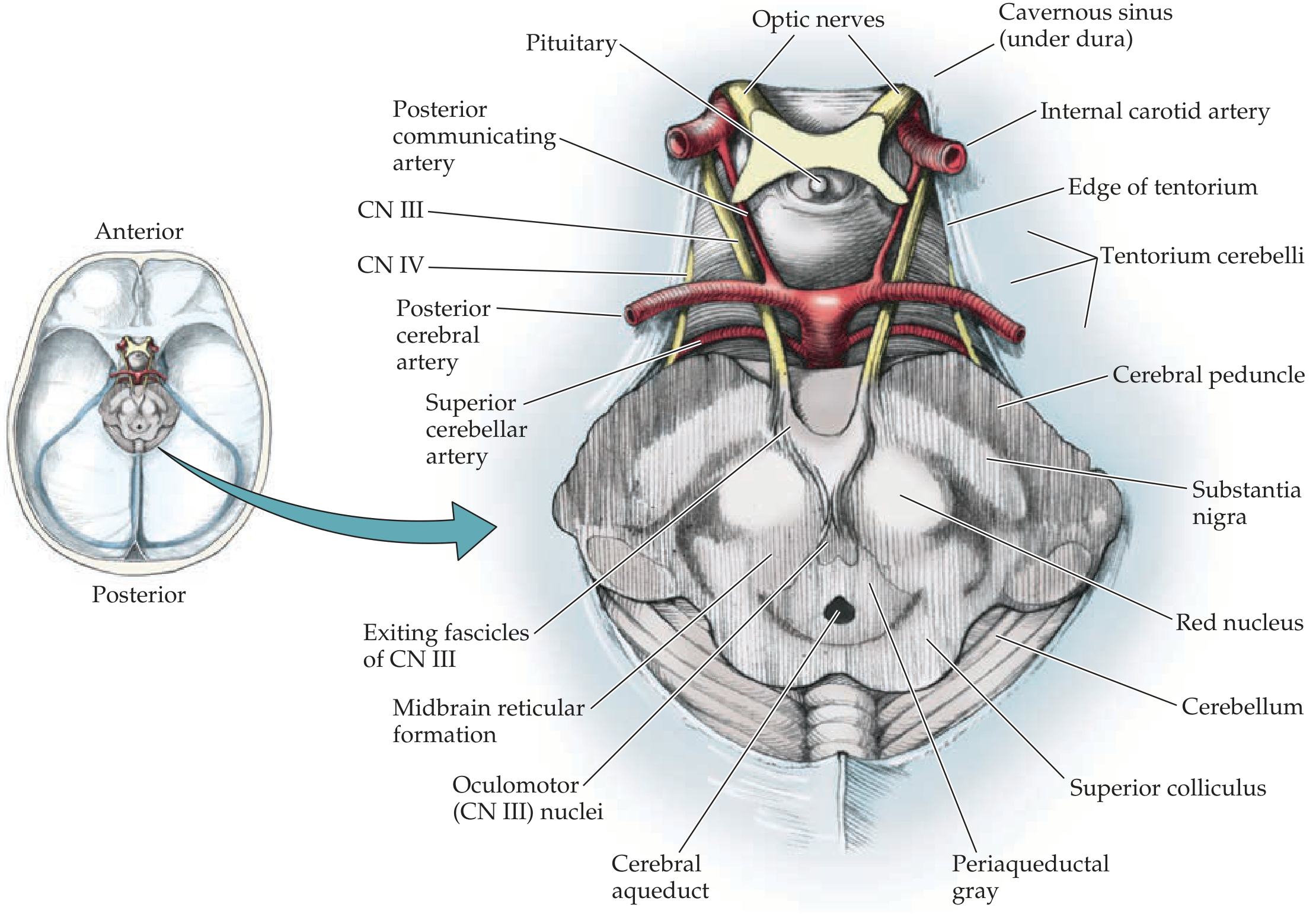
| CN III (Oculomotor) | Upper midbrain (level of superior colliculus), ventral to periaqueductal grey | Superior rectus (superior division), Medial rectus, Inferior rectus, Inferior oblique (inferior division); also levator palpebrae superioris |
| CN IV (Trochlear) | Lower midbrain (level of inferior colliculus) | Superior oblique only |
| CN VI (Abducens) | Pons (paramedian) | Lateral rectus only |
Mnemonic - LR6(SO4)3: Lateral Rectus = CN VI; Superior Oblique = CN IV; all others = CN III.
CN III also carries:
- Preganglionic parasympathetic fibers (from Edinger-Westphal nucleus) to the pupillary constrictor and ciliary muscle - these run superficially/medially in the nerve and are vulnerable to compression (e.g., posterior communicating artery aneurysm causes a "surgical" CN III palsy with pupil involvement).
Summary of Actions by Eye Position
The action of each muscle changes depending on eye position, because the angle between the muscle's line of pull and the globe's main axis changes as the eye rotates:
| Muscle | Primary | When abducted | When adducted |
|---|---|---|---|
| Superior rectus | Elevation + intorsion | Pure elevation | Mainly intorsion |
| Inferior rectus | Depression + extorsion | Pure depression | Mainly extorsion |
| Superior oblique | Intorsion + depression | Mainly intorsion | Pure depression |
| Inferior oblique | Extorsion + elevation | Mainly extorsion | Pure elevation |
Clinical Correlates
| CN palsy | Key sign | Other findings |
|---|---|---|
| CN III palsy | Eye is "down and out" (lateral rectus and superior oblique unopposed) | Ptosis (levator palpebrae), pupil dilation (if compressive) |
| CN IV palsy | Hypertropia worse in adduction; patient tilts head away | Vertical diplopia; most common cause of acquired vertical diplopia |
| CN VI palsy | Failure of abduction; convergent strabismus (esotropia) | Often first sign of raised intracranial pressure (long intracranial course) |
Sources: Kanski's Clinical Ophthalmology 10th ed., Neuroanatomy through Clinical Cases 3rd ed., Kandel Principles of Neural Science 6th ed.
This is a shared conversation. Sign in to Orris to start your own chat.