Here is a thorough breakdown of the COX (cyclooxygenase) pathway, compiled from Firestein & Kelley's Textbook of Rheumatology, Lippincott's Pharmacology, and Basic Medical Biochemistry.
The Cyclooxygenase (COX) Pathway
Overview
The COX pathway is one arm of the eicosanoid biosynthesis cascade. It converts arachidonic acid (AA) - a 20-carbon polyunsaturated fatty acid - into prostanoids: prostaglandins (PGs), thromboxanes (TXs), and prostacyclin (PGI2). These lipid mediators regulate inflammation, vascular tone, platelet aggregation, renal function, and many other physiologic processes.
Step 1 - Release of Arachidonic Acid
Arachidonic acid is stored esterified in membrane phospholipids. The first step is its liberation by phospholipase A2 (PLA2) - triggered by mechanical, chemical, or inflammatory stimuli.
Glucocorticoids inhibit PLA2 (by inducing lipocortin/annexin A1), which is one mechanism behind their broad anti-inflammatory effect.
Step 2 - The COX Enzyme (PGHS)
The key enzyme is prostaglandin G/H synthase (PGHS), a bifunctional homodimeric enzyme with two catalytic activities:
- Cyclooxygenase (COX) activity - oxygenates arachidonic acid
- Peroxidase activity - reduces the initial product
There are two isoforms:
| Feature | COX-1 (PGHS-1) | COX-2 (PGHS-2) |
|---|
| Expression | Constitutive (always present) | Inducible |
| Gene | PTGS1 | PTGS2 |
| Location | Platelets, endothelium, gastric mucosa, renal tubules, seminal vesicles | Macrophages, synoviocytes, endothelium, brain, kidney (macula densa) |
| Function | Homeostatic - gastric protection, platelet TXA2, renal blood flow | Inflammatory - prostaglandins at sites of injury/chronic disease |
| Induced by | Constitutive (Sp1 transcription factor) | IL-1β, TNF-α, NF-κB, AP-1; also oxidative stress, ischemia, seizures |
| Inhibited by | NSAIDs (non-selective) | NSAIDs, glucocorticoids, selective COX-2 inhibitors (coxibs) |
| Active site | Narrower hydrophobic channel | Slightly larger channel (allows selective inhibitor entry) |
COX-2 mRNA also contains ~12 AUUUA instability motifs, making the transcript short-lived and its expression tightly controlled.
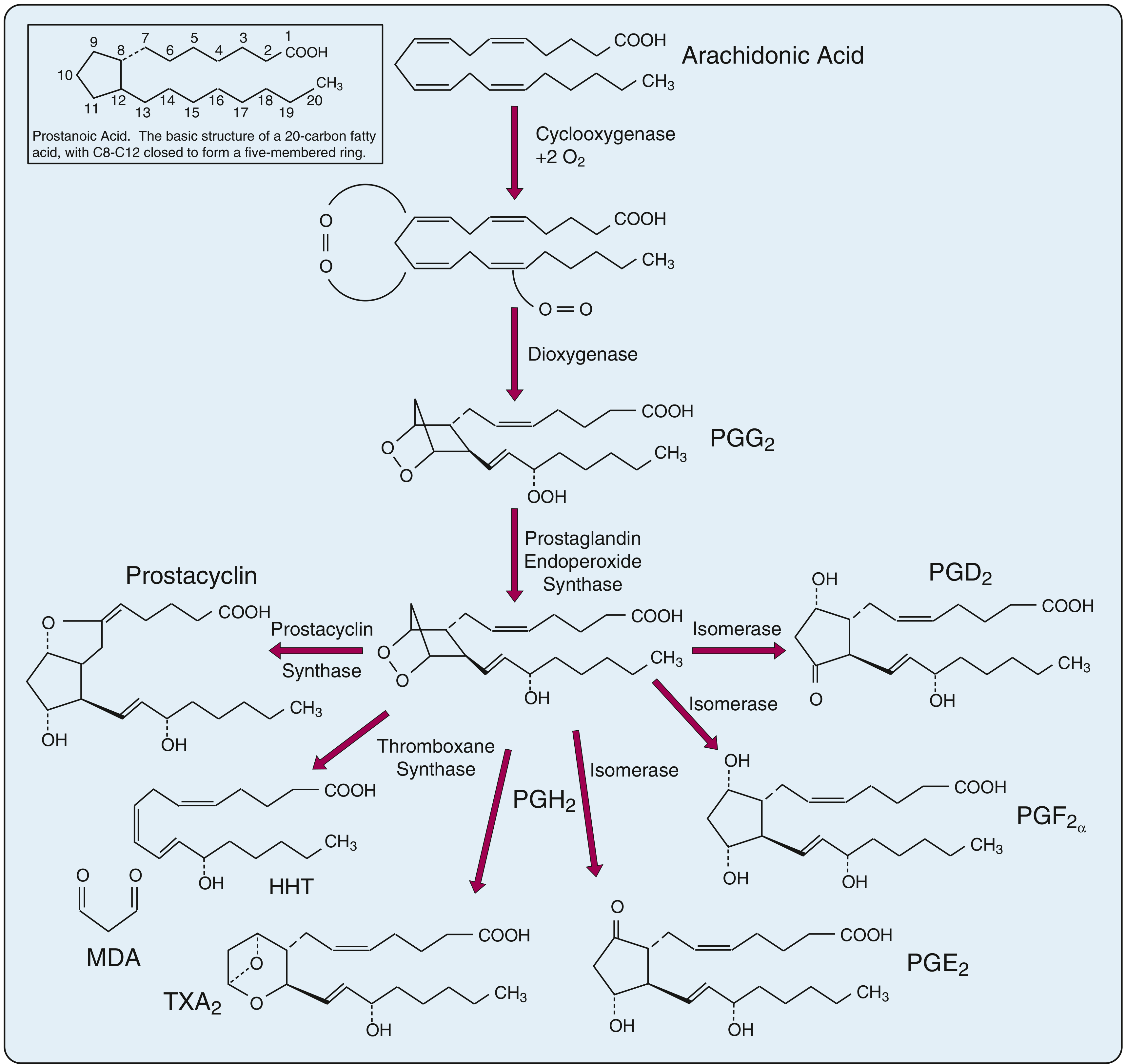
Step 3 - Biosynthetic Reactions
Fig. Cyclooxygenase pathway from arachidonic acid to PGH2 and downstream prostanoids (Firestein & Kelley's Rheumatology)
Reaction 1 - COX activity: AA → PGG2
- Cyclooxygenase activity inserts 2 O2 molecules across carbons 9 and 11, and at carbon 15
- Ring closure occurs between C8 and C12, creating the five-membered cyclopentane ring
- Product: PGG2 (an unstable bicyclic endoperoxide with a hydroperoxy group at C15)
- Requires double bonds at C8, C11, and C14 in the precursor fatty acid
Reaction 2 - Peroxidase activity: PGG2 → PGH2
- The hydroperoxy group (-OOH) at C15 is reduced to a hydroxyl group (-OH) by the peroxidase activity of the same enzyme
- Glutathione (GSH) serves as the reducing agent
- Product: PGH2 (prostaglandin H2) - the key branch-point intermediate
Step 4 - Tissue-Specific Downstream Products from PGH2
PGH2 is acted on by terminal synthases that vary by cell type:
| Terminal Synthase | Product | Primary Source | Key Actions |
|---|
| Thromboxane synthase | TXA2 | Platelets | Potent vasoconstrictor; platelet aggregation; promotes thrombosis |
| Prostacyclin synthase | PGI2 (prostacyclin) | Vascular endothelium | Vasodilator; inhibits platelet aggregation (opposes TXA2) |
| PGE synthase | PGE2 | Macrophages, fibroblasts | Vasodilation, fever, pain sensitization, inhibits gastric acid |
| PGD synthase | PGD2 | Mast cells, brain | Bronchoconstriction, sleep induction, allergy |
| Endoperoxide reductase / PGE 9-ketoreductase | PGF2α | Uterus, lung | Uterine contraction, bronchoconstriction |
TXA2 is chemically unstable (half-life ~30 sec) and hydrolyses spontaneously to inactive TXB2. PGI2 also has a short half-life (~2 min) and converts to 6-keto-PGF1α.
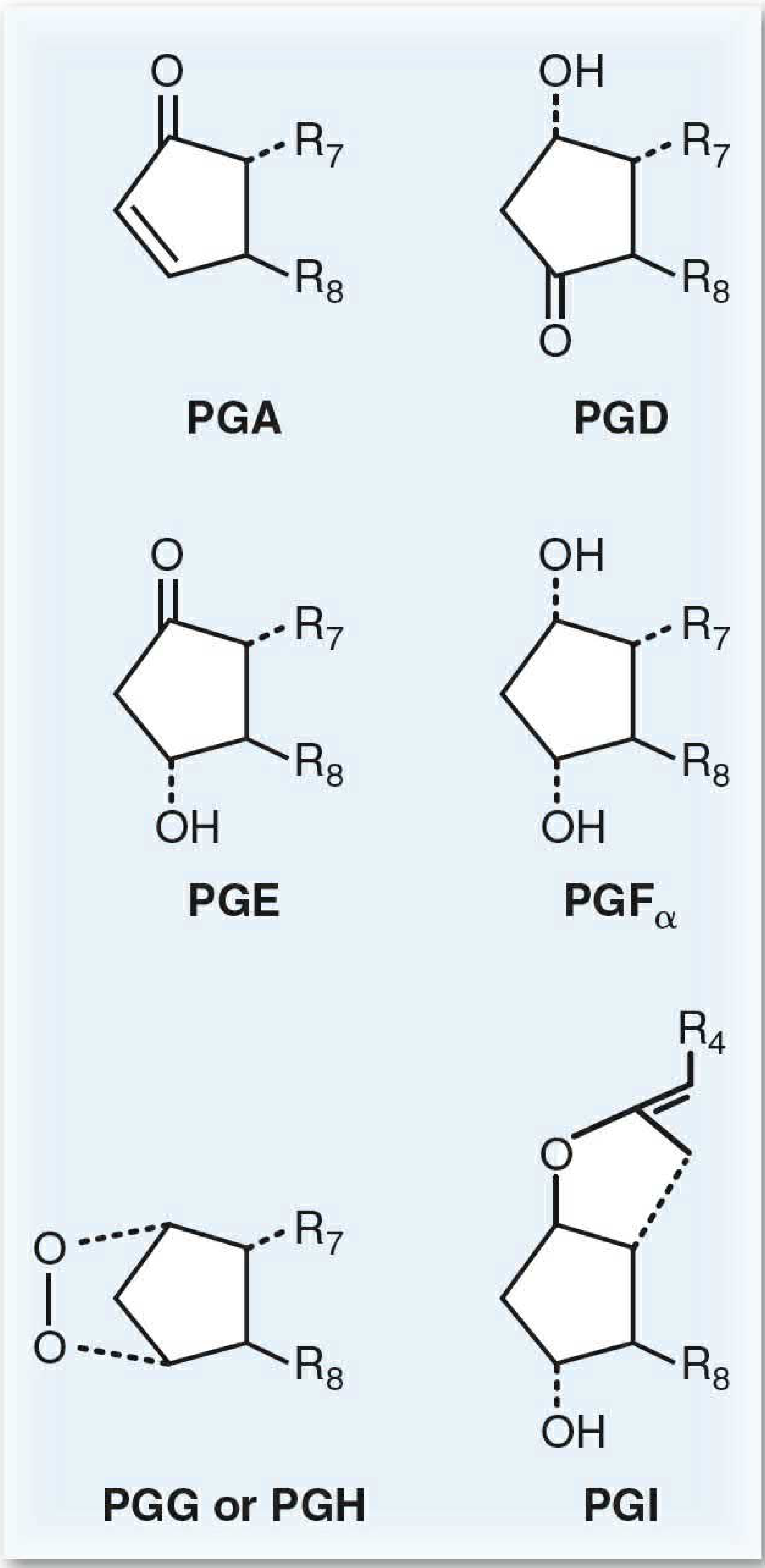
Prostaglandin Nomenclature
Fig. Ring substituents of the prostaglandin series (Basic Medical Biochemistry)
- Letter (PGE, PGF, etc.) = configuration of the ring substituents
- Subscript number (PGE2) = number of double bonds in the linear chain (series 2 comes from arachidonic acid, the most common in humans)
- Greek letter (PGF2α) = orientation of the C9 hydroxyl (only in F series)
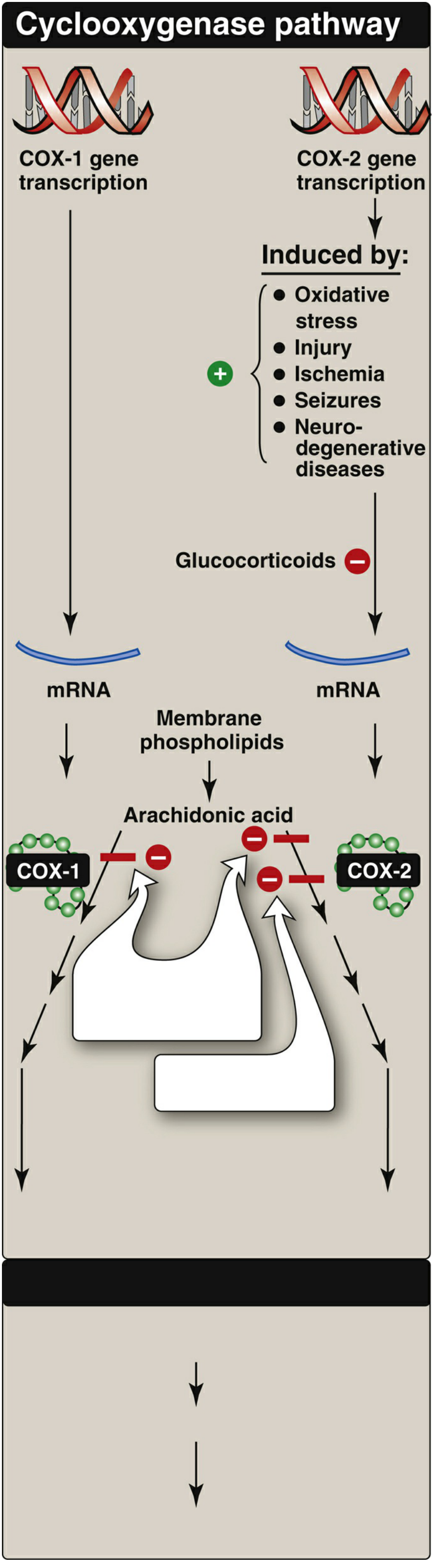
COX Pathway Gene Regulation
Fig. Regulation of COX-1 and COX-2 synthesis (Lippincott's Pharmacology)
- COX-1: constitutive expression via the Sp1 transcription factor; TATA-less promoter; cannot be readily induced or silenced
- COX-2: key transcriptional elements include NF-κB and the AP-1/cAMP response element; activated by inflammatory cytokines (IL-1β, TNF-α), oxidative stress, ischemia, and growth factors; suppressed by glucocorticoids
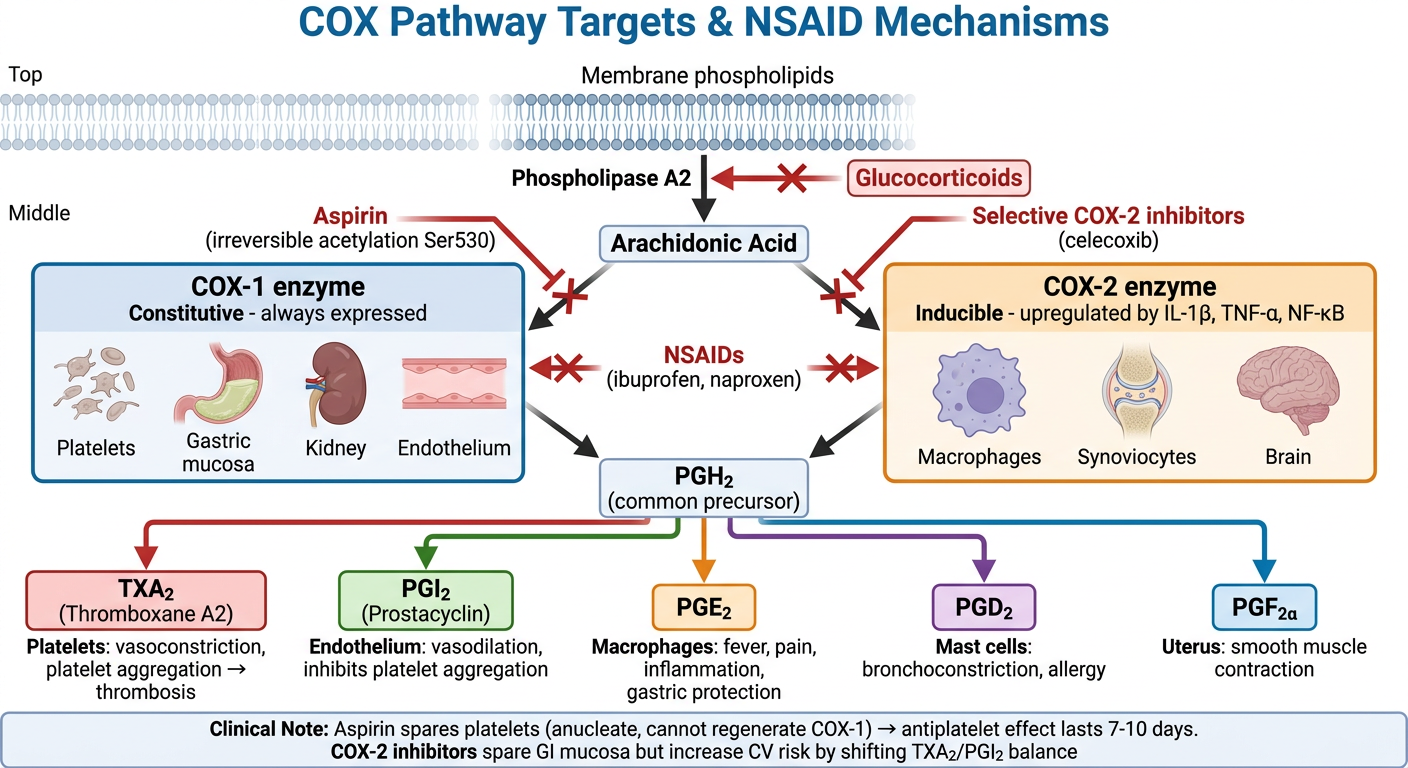
Pharmacological Targets in the COX Pathway
| Drug Class | Mechanism | Example Drugs |
|---|
| Non-selective NSAIDs | Block both COX-1 and COX-2 by occluding the active-site hydrophobic channel | Ibuprofen, naproxen, indomethacin |
| Aspirin | Irreversible acetylation of COX-1 (and COX-2 at higher doses) at Ser530; particularly prevents TXA2 in platelets | Aspirin |
| Selective COX-2 inhibitors (coxibs) | Fit into the larger COX-2 active site; spare COX-1 (gastric protection) | Celecoxib, etoricoxib |
| Glucocorticoids | Inhibit PLA2 (reduce AA release) + suppress COX-2 gene transcription | Dexamethasone, prednisolone |
Aspirin's irreversible block is especially important in platelets because platelets are anucleate - they cannot regenerate COX-1. So even low-dose aspirin (~81 mg) provides long-lasting antiplatelet effect for the 7-10 day platelet lifespan.
Physiological Roles of Key Prostanoids
| Prostanoid | Vascular | Platelets | Kidney | Uterus | GI tract |
|---|
| TXA2 | Vasoconstriction | Aggregation ↑ | - | - | - |
| PGI2 | Vasodilation | Aggregation ↓ | Renal blood flow ↑ | - | - |
| PGE2 | Vasodilation | - | Renin release; Na+ excretion | Contraction | Mucus ↑; acid ↓ |
| PGF2α | Vasoconstriction | - | - | Strong contraction | - |
| PGD2 | Vasodilation | Aggregation ↓ | - | - | - |
Clinical Relevance
- NSAIDs/aspirin - most widely used drugs acting on this pathway; side effects (peptic ulcer, renal impairment) are largely COX-1-mediated
- Coxibs - reduced GI risk but increased cardiovascular risk (by sparing PGI2 synthesis in endothelium while not reducing platelet TXA2)
- Misoprostol (PGE1 analog) - used to protect gastric mucosa or induce labor
- Carboprost / Dinoprostone (PGF2α / PGE2 analogs) - uterotonic agents
- Latanoprost (PGF2α analog) - reduces intraocular pressure in glaucoma
Sources:
- Firestein & Kelley's Textbook of Rheumatology, Chapter 27, p. 540
- Basic Medical Biochemistry - A Clinical Approach, 6e, Chapter 31, pp. 1136-1139
- Lippincott Illustrated Reviews: Pharmacology, Chapter 40, pp. 1334-1338