Uti in detail
Reading File
Finding Sources
Searching PubMed
"urinary tract infection" management
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Searching Images
urinary tract infection pathogenesis anatomy diagram
I now have all the content needed to compile a comprehensive UTI overview. Let me synthesize everything into a detailed, well-organized response.
Urinary Tract Infection (UTI) — Comprehensive Overview
Definition
A urinary tract infection (UTI) is an infection somewhere along the urinary tract that produces clinical symptoms. It results from either bladder invasion by a new urinary pathogen or a shift in the existing urinary microbiota's equilibrium with the host, causing local tissue injury and inflammation.
Critical distinction: The mere presence of bacteria in the urine without symptoms = asymptomatic bacteriuria (ASB) — this is NOT a UTI and generally should NOT be treated (except in pregnancy and pre-urologic procedure settings).
— Harrison's Principles of Internal Medicine 22E (2025)
Classification
| Term | Definition |
|---|---|
| Cystitis | Symptomatic infection of the bladder (lower UTI) |
| Pyelonephritis | Symptomatic infection of the kidney parenchyma (upper UTI) |
| Prostatitis | Symptomatic infection of the prostate |
| Uncomplicated UTI | Infection confined to the bladder in a non-catheterized patient |
| Complicated UTI | Extends beyond bladder (pyelonephritis, bacteremia, catheter-associated) |
| CAUTI | Catheter-associated UTI |
| Recurrent UTI | ≥2 episodes in 6 months or ≥3 episodes in 12 months |
| ASB | Bacteriuria ≥10⁵ CFU/mL without symptoms |
Bacteriuria thresholds:
- ASB/pyelonephritis: ≥10⁵ organisms/mL
- Cystitis (with pyuria + symptoms): as few as 10² organisms/mL
- CAUTI: ≥10³ CFU/mL
— Comprehensive Clinical Nephrology 7th Ed.; Harrison's 22E
Epidemiology
- UTI is one of the leading reasons antibiotics are prescribed globally, both in hospitals and the community
- Far more common in women than men — the majority of clinical research involves young adult women
- ASB affects 2–9% of all pregnant women; higher in lower socioeconomic groups, older age, higher parity, women with urinary tract abnormalities, diabetics
- 1–2% of pregnancies complicated by acute cystitis; ~1% by pyelonephritis
- ~70% of women who develop acute pyelonephritis in pregnancy had preceding covert bacteriuria
- Treating ASB in pregnancy reduces pyelonephritis incidence by >80%
— Comprehensive Clinical Nephrology 7th Ed.
Pathogenesis
The outcome — infection, colonization, or elimination — is determined by the interplay between three factors:
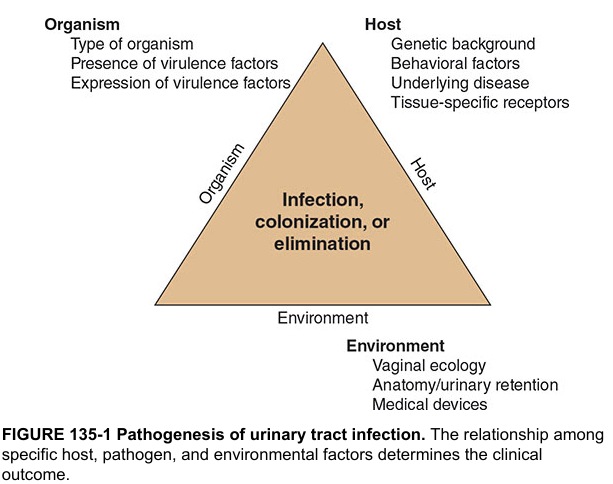
Organism Factors
- Virulence is critical: Uropathogenic E. coli (UPEC) possesses fimbriae/pili that allow adhesion to uroepithelial cells, enabling ascent from the perineum up the urethra to the bladder, and further to the kidneys
- Type 1 fimbriae bind to uroplakin on bladder epithelium; P-fimbriae bind to renal tubular epithelium
Host Factors
- Female anatomy: short urethra close to the perineum/anus = easiest access for pathogens
- Genetic background: women who don't express antibody to E. coli O antigen may have chronic colonization
- Behavioral factors: sexual activity, spermicide use, catheterization
- Tissue-specific receptors for bacterial adhesins
- Underlying disease: diabetes mellitus, structural urinary abnormalities, neurogenic bladder, immunosuppression
Environmental Factors
- Vaginal ecology (altered by antibiotics, spermicides, menopause)
- Anatomy/urinary retention: pregnancy causes ureteral dilation (especially right), poor bladder emptying, progesterone-induced smooth muscle relaxation → urinary stasis
- Medical devices: catheters, stents, stones
Causative Organisms
| Organism | Frequency | Notes |
|---|---|---|
| E. coli | ~75–85% | Most common; uropathogenic strains with adhesins |
| Klebsiella pneumoniae | 5–10% | Often in complicated/hospital-acquired |
| Proteus mirabilis | 3–5% | Associated with struvite stones (urease-positive) |
| Staphylococcus saprophyticus | Common in young sexually active women | |
| Enterococcus faecalis | Hospital/complicated UTI | |
| Pseudomonas aeruginosa | Hospital/catheter-associated | Often MDR |
| Group B Streptococcus | Pregnancy | |
| Staphylococcus aureus | Hematogenous seeding of kidney |
Pseudomonas UTIs are nearly always complicated — catheters, stents, or stones should be removed if possible. — Goldman-Cecil Medicine International Edition
Clinical Presentations
1. Acute Uncomplicated Cystitis
Symptoms:
- Dysuria (burning/pain on urination)
- Urinary frequency and urgency
- Suprapubic pain/tenderness
- Hematuria (gross or microscopic)
- No fever, no systemic signs
Key diagnostic rule: In a woman with ≥1 localizing urinary symptom and no complicating factors, the probability of UTI approaches 90% if vaginal discharge and complicating factors are absent. — Harrison's 22E
2. Acute Pyelonephritis (Upper UTI)
Symptoms:
- Fever, rigors, chills
- Flank pain / costovertebral angle (CVA) tenderness
- Nausea, vomiting, malaise
- May have associated lower urinary symptoms
- Can progress to urosepsis
3. Complicated UTI
- Any UTI with structural/functional abnormality, obstruction, immunocompromise, or catheterization
- Higher risk of treatment failure; broader-spectrum antibiotics often needed
- Includes pyelonephritis, renal abscess, emphysematous pyelonephritis
4. Recurrent UTI
- Relapse: same organism within 2 weeks — suggests inadequately treated upper tract infection
- Reinfection: different organism or same organism after >2 weeks — most common type in women
5. Catheter-Associated UTI (CAUTI)
- Bacteriuria is inevitable with catheterization; therefore, bacteriuria + pyuria alone is NOT sufficient for diagnosis
- Must have localizing urinary symptoms or unexplained fever, AND other causes systematically ruled out
- Threshold: ≥10³ CFU/mL
Diagnosis
History
Patient-reported symptoms have high positive predictive value in uncomplicated cystitis in adult women. Self-diagnosis in women with recurrent UTI is particularly accurate.
Urinalysis (Dipstick)
| Finding | Significance |
|---|---|
| Leukocyte esterase | Marker of pyuria (sensitivity ~75–96%) |
| Nitrites | Bacterial reduction of urinary nitrates (gram-negative bacteria); highly specific |
| Hematuria | Supports UTI but nonspecific |
| Positive LE + nitrites | ~90% positive predictive value for UTI |
Urine Culture
- Gold standard for diagnosis
- Required in: complicated UTI, pyelonephritis, pregnancy, recurrent UTI, treatment failure, atypical presentations
- Not routinely required for uncomplicated cystitis in women with classic symptoms
- Midstream clean-catch specimen preferred; catheter specimen in hospitalized patients
Microscopy
- Pyuria (>10 WBC/hpf) present in nearly all symptomatic UTIs
- Bacteriuria on Gram stain of unspun urine → correlates with ≥10⁵ CFU/mL
Imaging
- Not routine for uncomplicated UTI
- CT scan (non-contrast preferred for stones; with contrast for renal abscess, emphysematous pyelonephritis)
- Ultrasound to evaluate hydronephrosis, obstruction
- Voiding cystourethrogram (VCUG) for vesicoureteral reflux (VUR) evaluation
Management
Acute Uncomplicated Cystitis (Non-Pregnant Women)
| Antibiotic | Regimen | Notes |
|---|---|---|
| Nitrofurantoin macrocrystals | 100 mg BID × 5–7 days | First-line; avoid if CrCl <30 |
| Trimethoprim-sulfamethoxazole (TMP-SMX) | 160/800 mg BID × 3 days | Only if local resistance <20% |
| Fosfomycin trometamol | 3 g single dose | Excellent oral bioavailability |
| Pivmecillinam | 400 mg BID × 3–7 days | Available in some countries |
| Fluoroquinolones (ciprofloxacin, ofloxacin) | 3 days | Reserved for complicated cases; avoid as first-line for uncomplicated UTI |
| Beta-lactams (amoxicillin-clavulanate, cephalexin) | 3–7 days | Inferior efficacy; use if above not available |
Acute Pyelonephritis
Outpatient (mild–moderate):
- Ciprofloxacin 500 mg PO BID × 7 days (if susceptibility confirmed)
- TMP-SMX 160/800 mg PO BID × 14 days
- Oral beta-lactam × 10–14 days if susceptible
Inpatient (severe/septic):
- IV fluoroquinolone or aminoglycoside (± ampicillin for enterococcus coverage)
- Antipseudomonal beta-lactam (piperacillin-tazobactam, ceftriaxone) for complicated/hospital-acquired
- Duration: 7–14 days total; up to 2 weeks for severe cases
Complicated UTI / Pseudomonas UTI
- Remove or replace catheters/stents/stones when possible
- 7–14 days antibiotic treatment; up to 4–6 weeks for renal/perirenal abscess
- Drain abscesses ≥3 cm
- Options: ciprofloxacin IV, levofloxacin, aminoglycosides, antipseudomonal beta-lactams (pip-tazo, carbapenems), ceftazidime-avibactam, ceftolozane-tazobactam for MDR organisms — Goldman-Cecil Medicine International Edition
UTI in Pregnancy
- Screen all pregnant women at 12–16 weeks with urine culture (USPSTF Grade A)
- Treat ASB in pregnancy (up to 30% develop pyelonephritis if untreated)
- Safe antibiotics in pregnancy:
- Cephalexin 500 mg BID × 3–7 days
- Amoxicillin 500 mg TID × 7 days
- Nitrofurantoin 100 mg BID × 3–7 days (avoid in 1st trimester — possible birth defects; avoid near term — neonatal hemolysis)
- Avoid: Fluoroquinolones, tetracyclines throughout pregnancy; TMP-SMX in 1st trimester (folate antagonist) and 3rd trimester (kernicterus risk)
- Pyelonephritis in pregnancy: hospitalize, IV antibiotics (ampicillin + gentamicin), aggressive management — risk of premature labor, maternal sepsis, permanent renal injury
- Right-sided predominance (physiologic right ureteral dilation > left) — Rosen's Emergency Medicine; Tintinalli's Emergency Medicine; Comprehensive Clinical Nephrology 7th Ed.
Recurrent UTI Prevention
- Behavioral: post-coital voiding, adequate hydration, avoid spermicides
- Cranberry products (modest evidence — recent systematic review/meta-analysis, PMID 39030132)
- Antibiotic prophylaxis options:
- Post-coital single dose (TMP-SMX, nitrofurantoin)
- Daily low-dose prophylaxis (TMP-SMX 40/200 mg, nitrofurantoin 50–100 mg)
- Patient-initiated therapy (for women who can self-diagnose reliably)
- Topical vaginal estrogen in postmenopausal women (restores lactobacillus-dominant flora)
CAUTI Prevention & Management
- Remove or change catheter as soon as possible
- Avoid treating ASB in catheterized patients (Choosing Wisely recommendation — AUA)
- If catheter cannot be removed, treat CAUTI with systemic antibiotics for 7–14 days
- Use catheter only when necessary; use hydrophilic catheters for intermittent catheterization (especially in spinal cord injury)
Complications
| Complication | Notes |
|---|---|
| Pyelonephritis | Most serious complication of untreated lower UTI |
| Urosepsis | Life-threatening; requires IV antibiotics, ICU care |
| Renal abscess | Drain if ≥3 cm; prolonged antibiotics (4–6 weeks) |
| Emphysematous pyelonephritis | Gas-forming infection; predominantly diabetics; surgical/interventional urgency |
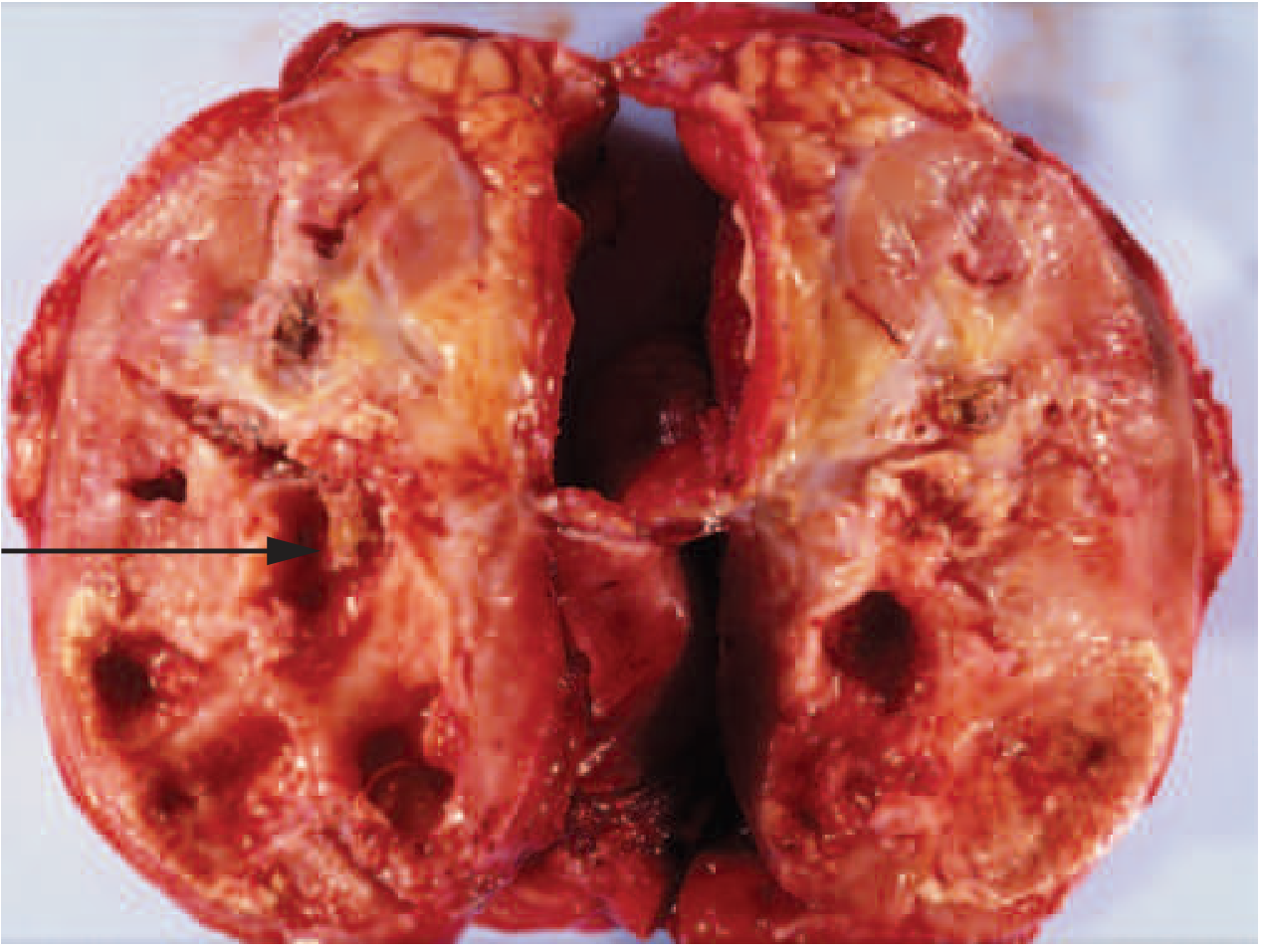
| Xanthogranulomatous pyelonephritis (XGP) | Chronic destructive infection; associated with staghorn calculi; can mimic renal malignancy |
| Papillary necrosis | Diabetics, analgesic abuse, sickle cell disease |
| Perinephric abscess | Extension beyond renal capsule |
| Premature labor, low birth weight | In untreated pyelonephritis in pregnancy |
| Chronic pyelonephritis/renal scarring | Especially with VUR in children |
Differential Diagnosis of UTI Symptoms
| Condition | Distinguishing Features |
|---|---|
| Urethritis (STI) — Chlamydia, Gonorrhea | Urethral discharge, sexual risk factors, gradual onset |
| Vaginitis | External dysuria, vaginal discharge, odor |
| Herpes genitalis | External dysuria, perineal burning, visible vesicles/ulcers |
| Appendicitis | Peritoneal signs, right iliac fossa pain, fever |
| Interstitial cystitis | Chronic, recurring; negative cultures |
| Ovarian torsion | Acute pelvic pain, nausea, adnexal tenderness |
| Renal calculi | Colicky flank pain radiating to groin, hematuria |
Special Populations
Spinal Cord Injury (SCI)
- UTI occurred in 100% of SCI patients with 40–50 year follow-up
- Risk factors: male sex, cervical injury level, condom catheter use
- Treat only symptomatic bacteriuria (National Institute consensus)
- Use antibiotics with minimal impact on normal flora; treat 5–14 days
- Do NOT use prophylactic antibiotics for indwelling or intermittent catheterization routinely — Campbell Walsh Wein Urology
Renal Transplant Recipients
- UTI common complication; hospitalization in 16.8% of patients within first 3 years
- Risk factors: obstructive uropathy, VUR, bladder abnormalities, ureteral stents
- TMP-SMX prophylaxis for P. jiroveci may reduce UTI incidence
- Avoid treating ASB without pyuria (risk of selecting resistant organisms)
Recent Guidelines (2024)
A WikiGuidelines consensus statement on UTI management (pediatrics + adults) was published in JAMA Network Open, November 2024 — WikiGuidelines UTI Consensus Statement (PMID 39495518). ACR Appropriateness Criteria for pediatric UTI imaging were updated in 2024 (PMID 38823954).
Summary Table
| Feature | Uncomplicated Cystitis | Pyelonephritis | CAUTI |
|---|---|---|---|
| Location | Bladder | Kidney | Catheterized bladder |
| Fever | No | Yes | Variable |
| CVA tenderness | No | Yes | Variable |
| Bacteriuria threshold | 10² (symptomatic) | 10⁵ | 10³ |
| Culture required? | No (classic symptoms) | Yes | Yes |
| Treatment duration | 3–7 days | 7–14 days | 7–14 days |
| Hospitalization | Usually No | Severe: Yes | Severe: Yes |
Sources: Harrison's Principles of Internal Medicine 22E (2025); Comprehensive Clinical Nephrology 7th Ed.; Rosen's Emergency Medicine; Tintinalli's Emergency Medicine; Campbell Walsh Wein Urology; Goldman-Cecil Medicine; Brenner and Rector's The Kidney; PMID 39495518; PMID 38823954; PMID 39030132
This is a shared conversation. Sign in to Orris to start your own chat.