laproscopic instruments
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching the Web
laparoscopic instruments types classification surgery
Reading Web Page
https://operativereview.com/laparoscopic-instruments
Here is a thorough guide to laparoscopic instruments, drawing from surgical textbooks (Maingot's Abdominal Operations, Fischer's Mastery of Surgery, Berek & Novak's Gynecology, Campbell-Walsh Urology) and current surgical references.
Laparoscopic Instruments
Laparoscopic (minimally invasive) surgery requires a distinct set of instruments that work through small ports in the abdominal wall. They fall into several functional categories.
1. Access and Insufflation Instruments
Veress Needle
A spring-loaded needle (2–3 mm) used for closed-entry pneumoperitoneum. The outer needle is sharp to penetrate the abdominal wall; the inner spring-loaded blunt obturator retracts when resistance is felt and springs forward once inside the peritoneal cavity to protect viscera. CO₂ is insufflated to 12–15 mmHg.
- Initial insufflation pressure should not exceed 10 mmHg (higher pressure suggests misplacement, e.g., preperitoneal placement)
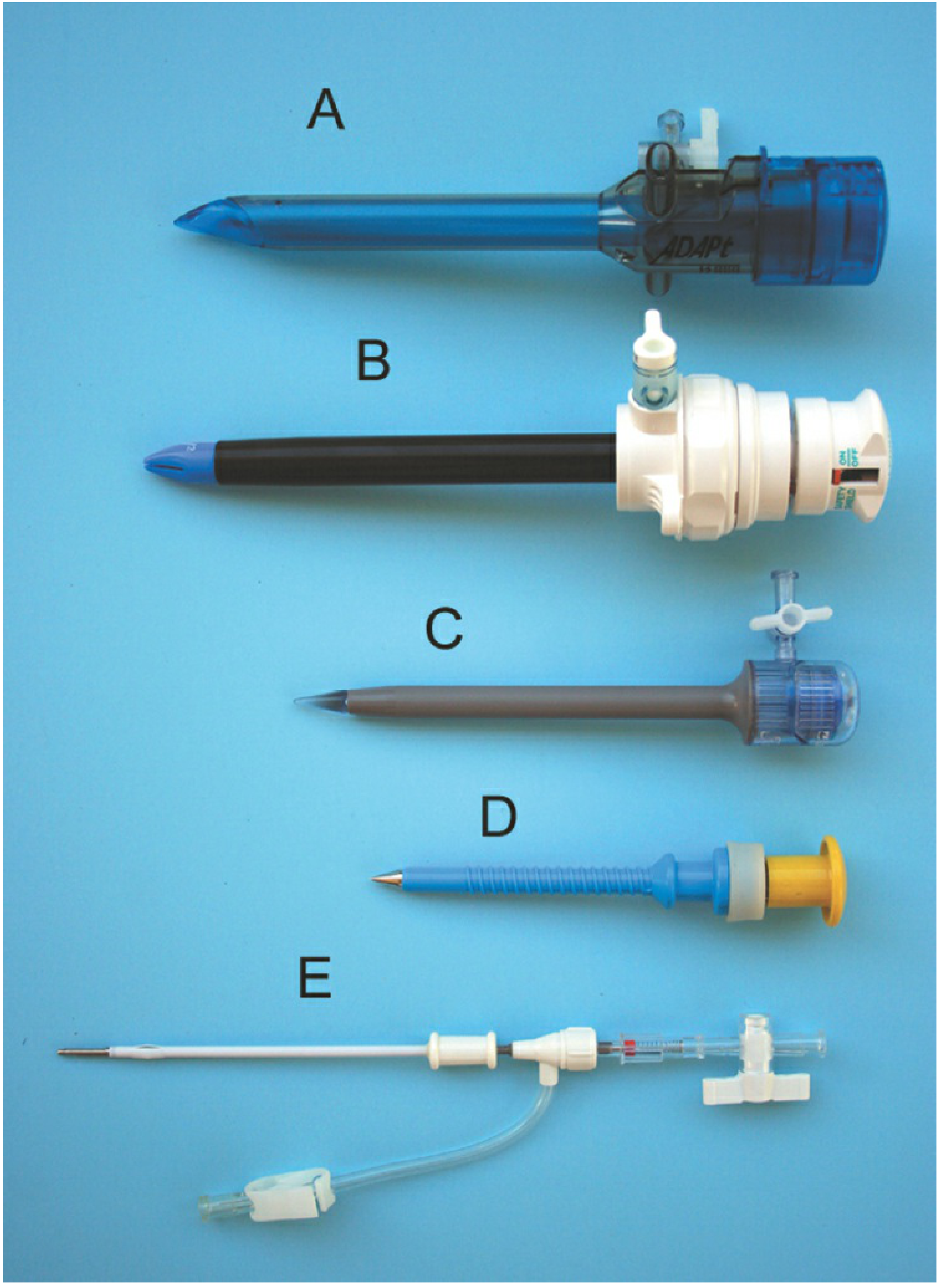
Trocars and Cannulas
A trocar is the full assembly of an obturator (pointed/blunt rod) + cannula (hollow tube). Once the obturator penetrates the abdominal wall, it is removed, leaving the cannula as a working channel.
Types of trocars:
| Type | Description |
|---|---|
| Bladed (sharp) | Traditional pyramidal/conical cutting tip; faster entry but higher vessel injury risk |
| Bladeless (dilating) | Dilates rather than cuts; less bleeding |
| Optical | Transparent tip allows visualization of each tissue layer during insertion |
| Hasson (blunt/open) | Used for open-entry technique; a purse-string suture secures it; safest for patients with prior abdominal surgery |
| Threaded (Ternamian EndoTIP) | Corkscrew design; rotated in without a sharp obturator |
Common sizes:
- 5 mm - for smaller instruments, clips, dissectors
- 10–12 mm - for camera, staplers, clip appliers, retrieval bags
- 15 mm - for large staplers or retrieval
Port placement rules (from Maingot's):
- All secondary cannulas must be inserted under direct laparoscopic vision
- Cannulas should be far enough apart to prevent instrument handle collision ("sword fighting")
- Direct them toward the surgical field for tension-free maneuverability
2. Visualization Equipment
Laparoscope (Telescope)
- A rigid Hopkins rod-lens telescope that transmits light and image
- 0° (forward-viewing) - straight view; simpler to use
- 30° (angled) - most commonly used; allows views "around corners"; standard for most abdominal procedures
- 45° - used in specific thoracoscopic or pelvic procedures
- Available in 5 mm and 10 mm diameters (10 mm gives brighter, higher-resolution image)
Camera System
- A CCD or CMOS camera head attaches to the laparoscope eyepiece
- Connected to a video processing unit and HD/4K monitor
- White balance and focus must be set before each case
Light Source and Fiber-Optic Cable
- Cold light (xenon or LED) transmitted via a fiber-optic cable to the laparoscope
- Provides illumination without heat inside the body cavity
CO₂ Insufflator
- Delivers CO₂ gas to maintain pneumoperitoneum at a set pressure (typically 12–15 mmHg)
- Monitors flow rate, total volume, and intraperitoneal pressure in real time
3. Graspers and Forceps
The workhorses of laparoscopic surgery. All are long-shafted (typically 33–45 cm) instruments inserted through 5 mm or 10 mm ports.
| Instrument | Jaw type | Use |
|---|---|---|
| Babcock forceps | Broad, rounded, atraumatic | Grasping bowel, appendix, fallopian tube - applied alongside bowel or on mesentery |
| Bowel grasper | Broad, perforated/fenestrated, atraumatic | Holding bowel with minimal serosal trauma |
| Alligator/Crocodile forceps | Wide flat jaws with serrations | Large surface contact; bowel mobilization |
| Blunt grasper | Smooth jaws | Gentle tissue retraction |
| DeBakey forceps | Fine longitudinal serrations | Delicate vascular tissue |
| Duckbill (fundus) grasper | Wide flat jaw | Uterine fundus, gallbladder |
| Allis forceps | Interlocking teeth | Firmer grip on tissue to be excised |
| Rat-tooth / Claw forceps | Sharp teeth | Specimen retrieval; traumatic grip |
| Tenaculum forceps | Single sharp tooth | Uterine or cervical manipulation |
| Gallbladder grasper | Curved serrated jaws | Gripping gallbladder wall |
| Appendix grasper | Atraumatic wide jaws | Holding appendix base |
Fenestrated graspers have "windows" (openings) in the jaws, which distribute grip pressure and prevent slippage.
4. Dissectors
Used for separating tissue planes by blunt dissection.
| Instrument | Description |
|---|---|
| Plain dissecting forceps | Fine-tipped, for blunt spreading dissection |
| Maryland dissector | Most widely used; fine curved jaws; can also be used with monopolar electrosurgery |
| Mixter (right-angle) forceps | L-shaped jaw; passes behind vessels/ducts for clipping or ligation; essential in cholecystectomy (dissecting the cystic duct/artery) |
| Bullet-nose forceps | Blunt rounded tip; safer near vessels |
| Dolphin-nose forceps | Tapered tip for fine plane dissection |
5. Scissors
| Type | Use |
|---|---|
| Straight scissors | Clean linear cuts on tissue/suture |
| Curved (Metzenbaum) | Fine dissection along curved planes |
| Hook scissors | Often coupled with monopolar cautery; cut and coagulate simultaneously |
Curved scissors allow more maneuverability and cauterization capability, saving operating time (Maingot's).
6. Energy Devices (Electrosurgical and Ultrasonic)
Monopolar Electrosurgery
- Hook electrode, spatula electrode, or scissors with cautery attachment
- Current passes from the instrument tip through the patient to a return plate
- Used for cutting and coagulation
- Risk: thermal spread to adjacent structures
Bipolar Forceps
- Current passes between the two jaws only - confined thermal effect
- Safer near nerves and delicate structures
- Used for vessel sealing and hemostasis
LigaSure (Vessel Sealing Device)
- Combines bipolar electrical energy + pressure to fuse vessel walls and collagen/elastin
- Seals vessels up to 7 mm diameter reliably
- Tissue bundles and mesenteric vessels in colorectal surgery
Harmonic Scalpel (Ultrasonic Dissector)
- Uses ultrasonic vibration (55,000 Hz) to cut and coagulate simultaneously
- Minimal thermal spread (~1.5 mm lateral spread vs. ~3 mm for monopolar)
- Better precision; preferred near delicate structures
- Can seal vessels up to 5 mm
7. Clip Appliers
- Automatic clip applier - applies titanium or polymer (Hem-o-lok) clips to seal ducts and vessels
- Available in single-fire or multi-fire (reloadable) formats
- Standard in cholecystectomy (cystic duct/artery) and other procedures
- Vascular pedicles in colorectal, urologic, and gynecologic surgery
8. Staplers
| Type | Use |
|---|---|
| Linear stapler (Endo-GIA) | Cuts and staples simultaneously; bowel transection, vascular pedicles |
| Circular stapler (EEA) | Intraluminal anastomosis; colocolic, ileocolic, esophagogastric joins |
The linear stapler has a dual purpose: a standard load for bowel and a vascular load for pedicles. Special maneuvers allow creation of J-pouches and side-to-side anastomoses.
Long instruments (38–40 cm) are required for procedures reaching the flexures or deep pelvis (e.g., total proctocolectomy, APR).
9. Suturing Instruments
| Instrument | Description |
|---|---|
| Laparoscopic needle holder | Straight or curved-head; straight or curved handles (curved handles reduce wrist angulation); various jaw configurations |
| Knot pusher | Allows extracorporeal knot tying; pushes tied knot down the suture into the body |
| Endo Stitch device (Medtronic) | Automated suture passing; needle toggles between jaws; widely used |
| Laparoscopic loop ligature | Pre-tied loop (e.g., Endoloop); one-handed application; quick ligation of appendix stump, ducts |
| Articulating suturing devices | Manual or motorized; greater degrees of freedom; useful in single-site surgery |
Surgeons should practice with multiple needle holder configurations to find what suits their technique best (Fischer's Mastery of Surgery).
10. Retractors
- Fan retractor - wide, deployable fan shape; liver retraction during upper abdominal surgery
- Paddle/flat retractors - organ displacement
- Must be placed to maintain exposure without obstructing the camera or instrument triangulation
11. Irrigation and Suction
- Combined suction-irrigator device: delivers warmed saline to wash the field and aspirates blood/smoke
- Smoke evacuator via the suction channel is standard in electrosurgery cases
12. Specimen Retrieval Bags
- Impermeable plastic bags introduced through a port
- Specimen (gallbladder, appendix, ovarian cyst, lymph nodes) is placed inside before extraction
- Prevents port-site contamination and spillage of bile, pus, or malignant cells
General Instrument Principles
- All laparoscopic instruments share a common structure: handle - shaft - working tip
- Shaft length is typically 33–45 cm; longer instruments needed for deep pelvic/colonic work
- Reusable vs. disposable versions exist for most instruments
- Handles may have a ratcheting lock (maintains grip without continuous pressure) or a slide lock
- Insulation of the shaft is critical for monopolar instruments to prevent capacitive coupling injuries
Sources: Maingot's Abdominal Operations; Fischer's Mastery of Surgery, 8th ed.; Berek & Novak's Gynecology; Operative Review of Surgery - Laparoscopic Instruments; Lapex Surgical A-to-Z Guide
This is a shared conversation. Sign in to Orris to start your own chat.