Hii
Hey there! How can I help you today?
Beta lectum antibiotcs in pharmacology
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a thorough pharmacology overview of Beta-Lactam Antibiotics, sourced from Katzung's Basic & Clinical Pharmacology (16th Edition).
Beta-Lactam Antibiotics
What Makes a Drug a "Beta-Lactam"?
All beta-lactam antibiotics share a four-membered beta-lactam ring as the core structural feature. This class includes:
- Penicillins
- Cephalosporins
- Monobactams
- Carbapenems
- Beta-lactamase inhibitors
1. Mechanism of Action
Beta-lactams are bactericidal and work by inhibiting bacterial cell wall synthesis.
Step-by-step:
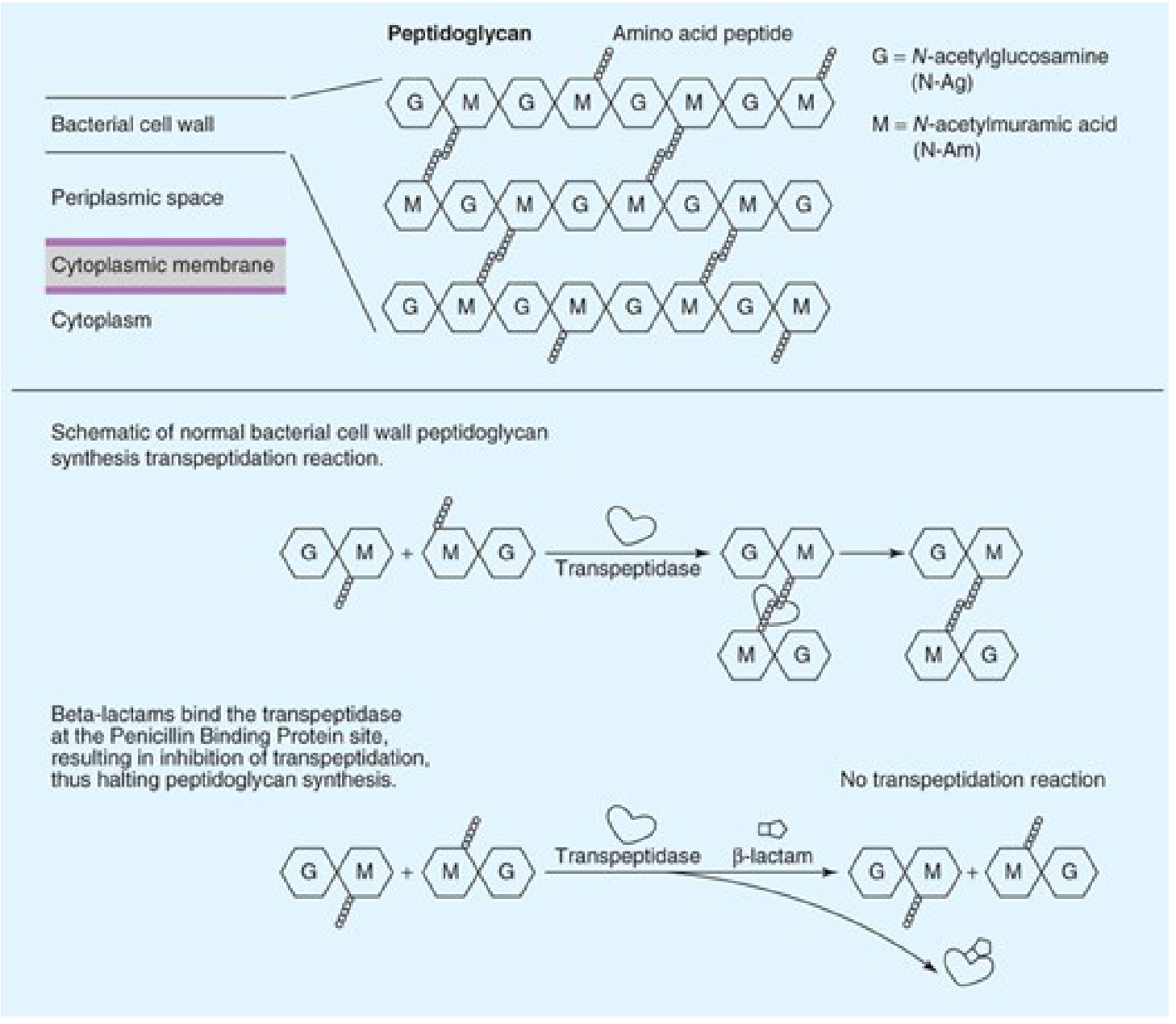
- Bacteria build their cell wall from peptidoglycan - alternating N-acetylglucosamine (G) and N-acetylmuramic acid (M) strands cross-linked by peptide chains.
- This cross-linking is done by an enzyme called transpeptidase (also called Penicillin-Binding Protein / PBP).
- Beta-lactams bind irreversibly to PBPs and block transpeptidation, so the cell wall cannot form properly.
- The bacterium cannot maintain osmotic integrity and lyses (dies).
2. Penicillins
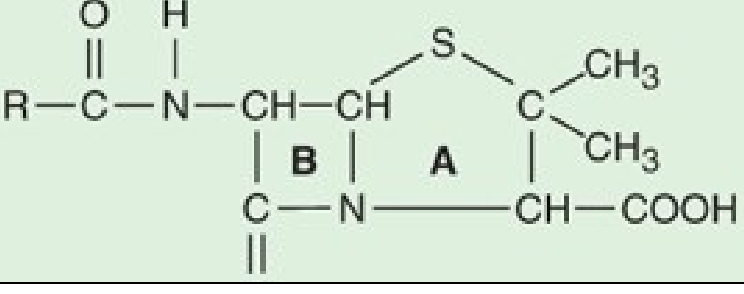
Structure: A thiazolidine ring (A) fused to the beta-lactam ring (B), with a side chain (R group) at the amino group position. The R group determines spectrum and stability.
Classification of Penicillins
| Group | Examples | Spectrum |
|---|---|---|
| Natural penicillins | Penicillin G (IV), Penicillin V (oral) | Streptococci, Neisseria, Treponema, anaerobes |
| Antistaphylococcal (penicillinase-resistant) | Nafcillin, Oxacillin, Dicloxacillin | Penicillinase-producing Staphylococci (not MRSA) |
| Aminopenicillins (extended spectrum) | Ampicillin, Amoxicillin | Gram+ + H. influenzae, E. coli, Listeria |
| Antipseudomonal | Piperacillin, Ticarcillin | Pseudomonas aeruginosa + gram-negatives |
Pharmacokinetics
- Penicillin G is acid-labile - must be given IV/IM
- Penicillin V, amoxicillin - acid-stable, given orally
- Excreted via the kidneys (dose-adjust in renal failure)
- Poor CNS penetration unless meninges inflamed
Clinical Uses
- Penicillin G: Streptococcal infections, syphilis, meningococcal meningitis
- Amoxicillin: Otitis media, sinusitis, H. pylori (with clarithromycin)
- Piperacillin-tazobactam: Hospital-acquired infections, Pseudomonas
3. Cephalosporins
Cephalosporins have the 7-aminocephalosporanic acid nucleus and are classified into generations based on their antibacterial spectrum.
Generations at a Glance
| Generation | Drugs | Coverage |
|---|---|---|
| 1st | Cefazolin, Cephalexin | Strong gram-positive (Staph, Strep); limited gram-negative |
| 2nd | Cefuroxime, Cefoxitin, Cefaclor | Expanded gram-negative (H. influenzae, Moraxella); Cefoxitin covers anaerobes |
| 3rd | Ceftriaxone, Cefotaxime, Ceftazidime | Broad gram-negative, penetrates CNS; Ceftazidime covers Pseudomonas |
| 4th | Cefepime | Very broad; Pseudomonas + gram-positives |
| 5th | Ceftaroline | MRSA activity (unique among cephalosporins) |
Key Points
- Ceftriaxone (half-life 7-8 hours): Once daily dosing; drug of choice for gonococcal infections and meningitis; biliary excretion (no renal dose adjustment needed)
- Ceftazidime: Only 3rd-gen with Pseudomonas coverage
- Ceftaroline: Only cephalosporin active against MRSA
- Cephalosporins are NOT active against Listeria monocytogenes or Enterococci (except ceftaroline with some enterococcal activity)
4. Carbapenems
Imipenem, Meropenem, Ertapenem, Doripenem
- Broadest spectrum of all antibiotics
- Active against gram-positives, gram-negatives, and anaerobes
- Imipenem is given with cilastatin (inhibits renal dehydropeptidase that degrades imipenem)
- Meropenem/Doripenem: Stable to renal dehydropeptidase, given alone
- Drug of choice for ESBL-producing organisms
- NOT active against MRSA, Stenotrophomonas
5. Monobactams
Aztreonam - the only monobactam in clinical use
- Active only against gram-negative aerobes (including Pseudomonas)
- No activity against gram-positives or anaerobes
- Safe in penicillin-allergic patients (no cross-reactivity except with ceftazidime)
- Useful in gram-negative infections in patients with beta-lactam allergy
6. Beta-Lactamase Inhibitors
Given in combination with penicillins to overcome beta-lactamase-mediated resistance:
| Inhibitor | Partner Drug | Combination |
|---|---|---|
| Clavulanic acid | Amoxicillin | Co-amoxiclav (Augmentin) |
| Sulbactam | Ampicillin | Unasyn |
| Tazobactam | Piperacillin | Piperacillin-tazobactam (Tazocin) |
| Avibactam | Ceftazidime | Ceftazidime-avibactam |
7. Resistance Mechanisms
There are four main mechanisms of beta-lactam resistance:
- Beta-lactamase production (most common) - enzymes that hydrolyze the beta-lactam ring (e.g., ESBL, AmpC, carbapenemases like KPC, NDM)
- Modified PBPs - altered target with reduced affinity (e.g., MRSA has PBP2a encoded by mecA gene)
- Impaired drug penetration - loss of outer membrane porins in gram-negatives
- Efflux pumps - active expulsion of the drug
8. Adverse Effects
- Hypersensitivity/Allergy (most important): Ranges from maculopapular rash to anaphylaxis. IgE-mediated anaphylaxis is most dangerous. Cross-reactivity between penicillins and cephalosporins is low (~1-2%).
- GI disturbance: Diarrhea, nausea, C. difficile colitis (especially with broad-spectrum agents)
- Seizures: At high doses (especially imipenem and penicillin G in CNS)
- Nephrotoxicity: Methicillin (no longer used) caused interstitial nephritis
- Ceftriaxone: Can cause biliary sludge/pseudolithiasis, especially in children; avoid in neonates with hyperbilirubinemia (displaces bilirubin from albumin)
Summary Table
| Class | Mechanism | Key Spectrum | Resistance |
|---|---|---|---|
| Penicillins | PBP inhibition | Gram+ (natural); broad (extended spectrum) | Beta-lactamase, PBP mutation |
| Cephalosporins | PBP inhibition | Gen 1-5 expanding gram- coverage | ESBL, AmpC, MRSA PBP2a |
| Carbapenems | PBP inhibition | Broadest - all including anaerobes | Carbapenemases (KPC, NDM) |
| Monobactams | PBP inhibition | Gram-negatives only | - |
| Beta-lactamase inhibitors | Inhibit beta-lactamase | Used in combination only | ESBL, carbapenemases |
Source: Katzung's Basic and Clinical Pharmacology, 16th Edition - Chapter 43: Beta-Lactam & Other Cell Wall- & Membrane-Active Antibiotics
Penciline histery cositive organism Chemistry Classification Pharmakokinetics and pharmacodynamics Indication contraindication clinical use and adverse effects And dose and routes In pharmacology
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
Reading File
I now have all the content needed. Let me compile a comprehensive, well-structured answer.
Penicillin - Complete Pharmacology
Source: Goodman & Gilman's Pharmacological Basis of Therapeutics, Katzung's Basic & Clinical Pharmacology (16th Ed.)
1. HISTORY
- 1928 - Alexander Fleming, at St. Mary's Hospital London, observed that a mold (Penicillium notatum) contaminating a Staphylococcus culture caused bacterial lysis. He named the substance penicillin.
- 1940 - Howard Florey, Ernst Chain, and Abraham at Oxford purified it and showed dramatic therapeutic effect in mice with streptococcal infections.
- 1941 - First human trial: a policeman with severe mixed staph/strep infection was treated with penicillin - some recovered from the urine of other patients (hence the famous quote: "purified by passage through the Oxford Police Force").
- 1942 - 122 million units produced in the US; first clinical trials at Yale and Mayo Clinic.
- 1943 - Adopted by US Armed Forces; deep-fermentation procedure enabled mass production.
- By 1950: over 200 trillion units (nearly 150 tons) produced per year.
2. SENSITIVE (HISTORY-POSITIVE) ORGANISMS
Penicillin G is the drug of choice or highly active against the following:
Gram-Positive Cocci
| Organism | Notes |
|---|---|
| Streptococcus pyogenes (Group A) | Drug of choice |
| Streptococcus pneumoniae (sensitive strains) | Resistance increasing |
| Viridans streptococci (susceptible) | Mostly still sensitive |
| Enterococci | Aminopenicillin (ampicillin) needed; synergy with aminoglycosides |
Gram-Positive Rods
| Organism | Notes |
|---|---|
| Clostridium spp. | Highly sensitive |
| Actinomyces israelii | Drug of choice |
| Listeria monocytogenes | Ampicillin used |
Gram-Negative Cocci
| Organism | Notes |
|---|---|
| Neisseria meningitidis | Remains very sensitive to Pen G |
| Neisseria gonorrhoeae | Largely resistant now; ceftriaxone preferred |
Spirochetes
| Organism | Disease | Drug |
|---|---|---|
| Treponema pallidum | Syphilis | Benzathine Pen G - DOC |
| Borrelia burgdorferi | Lyme disease | Penicillin susceptible |
| Leptospira spp. | Leptospirosis | Penicillin G |
Gram-Negative Anaerobes
- Most susceptible except Bacteroides fragilis (resistant - produces cephalosporinase)
NOT Sensitive to Penicillin
- MRSA, most Staphylococcus aureus (>90% resistant via beta-lactamase)
- Most gram-negative enteric bacilli (E. coli, Klebsiella, Pseudomonas)
- Amebae, fungi, viruses, Rickettsiae, Mycoplasma
3. CHEMISTRY
Core Structure (6-Aminopenicillanic Acid)
- Ring A = Thiazolidine ring (5-membered, contains sulfur)
- Ring B = Beta-lactam ring (4-membered - the defining feature)
- R group = Side chain at the secondary amino group (RNH-); determines spectrum, stability, and route
- 6-aminopenicillanic acid nucleus = Rings A + B together - structural integrity is essential for activity
- Beta-lactamase opens the beta-lactam ring → yields penicilloic acid (inactive)
Key Points
- Carbapenems have a different stereochemical configuration in the lactam ring - this imparts resistance to most common beta-lactamases
- Monobactams have only the beta-lactam ring (no fused ring)
4. CLASSIFICATION
A. Natural Penicillins
| Drug | Route | Notes |
|---|---|---|
| Penicillin G (Benzylpenicillin) | IV, IM | Acid-labile; can't be given orally |
| Penicillin V (Phenoxymethylpenicillin) | Oral | Acid-stable; 2-5x better GI absorption |
| Penicillin G Benzathine | IM (long-acting) | Levels last ~26 days; used in syphilis, rheumatic fever prophylaxis |
| Penicillin G Procaine | IM (medium-acting) | Slower absorption than Pen G |
B. Antistaphylococcal (Penicillinase-Resistant) Penicillins
| Drug | Route | Indication |
|---|---|---|
| Nafcillin | IV | Serious MSSA infections (endocarditis) |
| Oxacillin | IV | Same as nafcillin |
| Cloxacillin | Oral | Mild-moderate staphylococcal infections |
| Dicloxacillin | Oral | Mild-moderate staphylococcal infections |
| Methicillin | Historical - withdrawn | Caused interstitial nephritis |
C. Aminopenicillins (Extended Spectrum)
| Drug | Route | Spectrum Addition |
|---|---|---|
| Ampicillin | IV/Oral | + H. influenzae, E. coli, Listeria, Enterococcus |
| Amoxicillin | Oral | Same as ampicillin; better absorbed (food doesn't impair) |
D. Antipseudomonal Penicillins
| Drug | Notes |
|---|---|
| Piperacillin | Active vs. Pseudomonas, Klebsiella, Bacteroides |
| Ticarcillin | Less active vs. Pseudomonas than piperacillin |
| Piperacillin-tazobactam | Most common clinical use; broad hospital-acquired infection coverage |
5. PHARMACOKINETICS
Absorption
| Drug | Oral Bioavailability | Note |
|---|---|---|
| Penicillin G | Poor (acid-labile) | Only IV/IM |
| Penicillin V | Good | Take 30 min before or 2 h after meals |
| Amoxicillin | ~90% | Food does NOT impair absorption |
| Ampicillin | ~50% | Food impairs absorption |
| Nafcillin | Erratic - NOT suitable oral | IV only |
| Dicloxacillin | Good | Take on empty stomach |
Distribution
- Widely distributed to joint fluid, pleural, pericardial fluid, bile
- Poor CNS penetration normally (<1% of plasma); increases to ~5% with meningeal inflammation
- Poor intracellular penetration (polar molecules - stay extracellular)
- Poor penetration: prostatic secretions, intraocular fluid, brain parenchyma
Metabolism & Excretion
- Eliminated rapidly via glomerular filtration + renal tubular secretion
- Half-life = 30-90 minutes (short)
- Probenecid (blocks tubular secretion) - delays excretion and prolongs action
- Dose adjustment needed in renal failure (except nafcillin - hepatic excretion)
- Anuria extends t1/2 of Pen G from 0.5 h to ~10 h
- Urine concentrations are very high (useful for urinary tract infections)
Long-acting Preparations
| Preparation | Peak | Duration |
|---|---|---|
| Penicillin G Procaine | Slower onset | 12-24 hours |
| Penicillin G Benzathine | Very slow onset | ~26 days |
6. PHARMACODYNAMICS
Mechanism of Action (Bactericidal)
- Bacteria build cell walls from peptidoglycan (alternating N-acetylglucosamine and N-acetylmuramic acid chains cross-linked by peptide bridges)
- Cross-linking is performed by transpeptidase enzyme located at Penicillin-Binding Proteins (PBPs)
- Penicillin binds irreversibly to PBPs and inhibits transpeptidation → peptidoglycan synthesis halts
- Cell wall weakens → bacterium lyses from osmotic pressure
Effect is TIME-DEPENDENT (not concentration-dependent) - efficacy correlates with time the drug level stays above MIC.
Resistance Mechanisms
| Mechanism | Example |
|---|---|
| Beta-lactamase production (most common) | S. aureus, H. influenzae, E. coli |
| PBP modification (altered target) | MRSA (PBP2a via mecA gene), resistant pneumococci, enterococci |
| Impaired penetration (outer membrane porins) | Gram-negative bacteria |
| Efflux pumps | P. aeruginosa |
7. INDICATIONS & CLINICAL USES
| Indication | Drug of Choice | Dose |
|---|---|---|
| Streptococcal pharyngitis | Penicillin V oral or Benzathine Pen G IM | Pen V: 250-500 mg 4x/day x 10 days; Benzathine: 1.2 MU single IM |
| Pneumococcal pneumonia (sensitive) | Penicillin G IV | 12-24 million units/day IV |
| Pneumococcal meningitis (empiric) | Vancomycin + 3rd gen cephalosporin (not penicillin alone - resistance risk) | - |
| Syphilis (primary/secondary) | Benzathine Penicillin G | 2.4 MU IM x 1 dose |
| Syphilis (neurosyphilis) | Penicillin G IV | 18-24 MU/day x 10-14 days |
| Rheumatic fever prophylaxis | Benzathine Pen G | 1.2 MU IM every 3-4 weeks |
| MSSA endocarditis / bacteremia | Nafcillin or Oxacillin IV | 8-12 g/day in divided doses |
| Enterococcal endocarditis | Ampicillin + ceftriaxone (or gentamicin) | Ampicillin 2 g IV q4h |
| Listeria meningitis | Ampicillin IV | High dose |
| H. pylori eradication | Amoxicillin + clarithromycin + PPI | Amoxicillin 1 g BD |
| Lyme disease | Penicillin G IV / Amoxicillin oral | Depending on stage |
| Actinomycosis | Penicillin G IV | 18-24 MU/day x 2-6 weeks |
| Mild skin/soft tissue (Staph) | Dicloxacillin or Cloxacillin oral | 0.25-0.5 g q4-6h |
| Otitis media, sinusitis (empiric) | Amoxicillin | 45-90 mg/kg/day in children |
| Community-acquired pneumonia (low risk) | Amoxicillin | 1 g q8h |
8. CONTRAINDICATIONS
| Contraindication | Reason |
|---|---|
| History of anaphylaxis / severe immediate hypersensitivity to penicillin | Risk of fatal anaphylaxis - absolute contraindication |
| Known allergy to penicillin + cephalosporins | Cross-reactivity ~1-2% for cephalosporins; higher for anaphylaxis history |
| Severe renal impairment (without dose adjustment) | Drug accumulation → neurotoxicity (seizures) |
| Infectious mononucleosis (ampicillin/amoxicillin) | ~100% rate of maculopapular rash |
Precautions:
- Use cautiously in history of asthma, hives, or atopy
- Mild penicillin rash (non-IgE) is NOT a contraindication to cephalosporins
9. ADVERSE EFFECTS
Hypersensitivity (Most Common & Important)
| Type | Manifestation | Mechanism |
|---|---|---|
| Immediate (<1 h) | Anaphylaxis, urticaria, angioedema, bronchospasm | IgE-mediated (minor determinants) |
| Accelerated (1-72 h) | Urticaria, rash | IgE-mediated (major determinants) |
| Delayed (>72 h) | Maculopapular rash, serum sickness, drug fever | IgG/immune complex |
- Anaphylaxis incidence: 0.004-0.04%; fatal anaphylaxis: 0.001%
- Penicillin acts as a hapten - penicilloyl moiety (major determinant) binds to proteins to trigger immune response
- Ampicillin rash: ~9% incidence; nearly 100% in patients with EBV (mono)
Other Adverse Effects
| Effect | Details |
|---|---|
| CNS - Seizures | High doses especially in renal failure; penicillin is neuroexcitatory |
| GI Disturbance | Diarrhea, nausea - disruption of gut flora |
| Interstitial Nephritis | Rare; methicillin (withdrawn), nafcillin, piperacillin most implicated |
| Coombs-positive hemolysis | Coombs test becomes positive with prolonged therapy; overt hemolytic anemia rare |
| Neutropenia | Up to 30% with nafcillin >8-12 g/day for >21 days; bone marrow arrest of maturation |
| Electrolyte disturbance | High-dose IV penicillin G contains sodium/potassium - risk of hypernatremia or hyperkalemia |
| Jarisch-Herxheimer reaction | When treating syphilis - fever, rigors, hypotension due to spirochete lysis (not a true allergy) |
| C. difficile colitis | Especially with broad-spectrum agents (ampicillin, amoxicillin-clavulanate) |
10. DOSES & ROUTES
Penicillin G
| Indication | Dose | Route |
|---|---|---|
| Minor infections | 600,000 - 1.2 MU/day | IM |
| Moderate infections | 4-8 MU/day | IV in 4-6 divided doses |
| Severe infections (meningitis, endocarditis) | 18-24 MU/day | IV continuous infusion or q4h |
| Syphilis (primary/secondary) | Benzathine 2.4 MU | Single IM dose |
| Syphilis (neurosyphilis) | Pen G 3-4 MU q4h x 10-14 days | IV |
| Rheumatic fever prophylaxis | Benzathine 1.2 MU | IM every 3-4 weeks |
Penicillin V
| Indication | Dose | Route |
|---|---|---|
| Streptococcal pharyngitis | 250-500 mg 4x/day x 10 days | Oral |
| Minor infections | 250-500 mg q6h | Oral |
Ampicillin
| Indication | Dose | Route |
|---|---|---|
| Moderate infections | 250-500 mg q6h | Oral |
| Serious infections (meningitis, endocarditis) | 2 g IV q4-6h (up to 12 g/day) | IV |
Amoxicillin
| Indication | Dose | Route |
|---|---|---|
| Otitis media (adult) | 500 mg-1 g q8h | Oral |
| Children (otitis media) | 45-90 mg/kg/day divided | Oral |
| H. pylori (triple therapy) | 1 g BD x 14 days | Oral |
| CAP (low risk) | 1 g q8h | Oral |
Nafcillin / Oxacillin (IV)
| Indication | Dose |
|---|---|
| MSSA bacteremia / endocarditis | 8-12 g/day IV in 6 divided doses (1-2 g q4h) |
Dicloxacillin (Oral)
| Indication | Dose |
|---|---|
| Mild-moderate skin/soft tissue | 0.25-0.5 g q4-6h (25-100 mg/kg/day in children) |
Piperacillin-Tazobactam
| Indication | Dose | Route |
|---|---|---|
| Hospital-acquired infections, febrile neutropenia | 3.375-4.5 g q6-8h | IV |
Memory Tip for Penicillin-Sensitive Organisms: "SPACE MLS"
- Streptococci (most) | Pneumococci (sensitive strains) | Actinomyces | Clostridium | Enterococci (ampicillin)
- Meningococci | Listeria (ampicillin) | Spirochetes (Treponema, Borrelia, Leptospira)
Sources: Goodman & Gilman's Pharmacological Basis of Therapeutics, 13th Ed., Chapter 58 | Katzung's Basic & Clinical Pharmacology, 16th Ed., Chapter 43
This is a shared conversation. Sign in to Orris to start your own chat.