Diltiazem in PSVT
Reading File
Finding Sources
Finding Sources
Searching PubMed
diltiazem "supraventricular tachycardia" treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything needed for a thorough, well-cited answer.
Diltiazem in PSVT
Mechanism of Action
Diltiazem is a non-dihydropyridine calcium channel blocker (Class IV antiarrhythmic, Vaughan Williams classification). It blocks L-type Ca²⁺ channels selectively in cardiac nodal tissue - unlike dihydropyridines (e.g. nifedipine) which act mainly on vascular smooth muscle. Its key electrophysiological effects are:
- Slows AV nodal conduction - decreases the velocity of impulse transmission through the AV node, increasing the PR interval
- Prolongs AV nodal refractory period - blocks the slow inward calcium current during depolarization
- Decremental conduction - both effects together produce AV nodal block
PSVT (most commonly AVNRT or orthodromic AVRT) is a reentrant tachycardia dependent on AV nodal conduction as part of its circuit. By blocking the AV node, diltiazem interrupts the reentrant loop and terminates the arrhythmia.
Its effects on AV nodal tissue are selective - it reduces conduction in the tissue responsible for the tachycardia while sparing normal conduction tissue.
- Goodman & Gilman's Pharmacological Basis of Therapeutics, p. 245-247
- Roberts and Hedges' Clinical Procedures in Emergency Medicine, p. 3737-3741
Clinical Indications
| Setting | Role |
|---|---|
| Acute PSVT (narrow-complex) | Rapid termination / conversion to sinus rhythm |
| Rate control in AF/atrial flutter | Ventricular slowing (without accessory bypass conduction) |
| Chronic PSVT prophylaxis | Oral diltiazem to prevent recurrent episodes |
| Automaticity-driven SVTs | Ectopic, multifocal, or junctional tachycardia (stable, narrow-complex) |
Parenteral diltiazem is approved for temporary control of rapid ventricular rate in atrial flutter/AF and for rapid conversion of PSVT to sinus rhythm - though IV adenosine has largely supplanted it for acute termination due to its shorter onset and action.
- Goodman & Gilman, p. 247
Position in the Treatment Algorithm
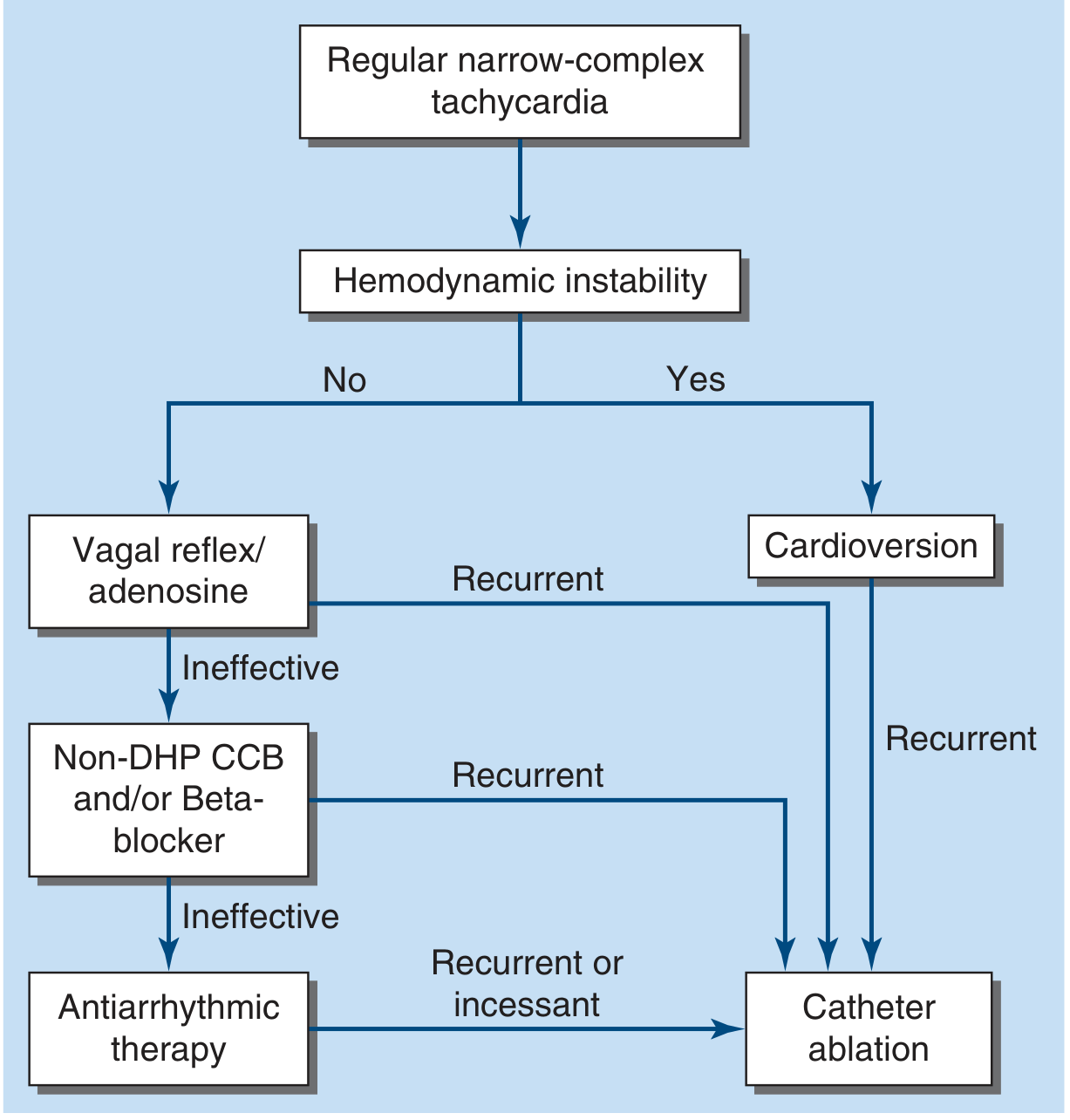
Step-wise approach for hemodynamically stable narrow-complex PSVT:
- Vagal maneuvers (Valsalva, carotid sinus massage) - first line
- IV Adenosine - if vagal maneuvers fail (terminates the vast majority of PSVT)
- Non-DHP CCB (diltiazem or verapamil) and/or beta-blocker - if adenosine fails or PSVT is recurrent
- Antiarrhythmic therapy - if above ineffective
- Catheter ablation - for recurrent/incessant PSVT
Hemodynamically unstable PSVT → immediate DC cardioversion.
Dosing (IV)
| Dose | Details |
|---|---|
| Initial bolus | 0.25 mg/kg IV |
| Repeat bolus | 0.35 mg/kg IV (if first dose insufficient) |
| Maintenance infusion | 5-15 mg/hr IV |
| Pre-treatment | Consider IV calcium (calcium gluconate) if patient is hypotensive |
For chronic/prophylactic use: oral diltiazem (various extended-release formulations).
- Roberts and Hedges' Clinical Procedures in Emergency Medicine, p. 3747
Contraindications
- Sick sinus syndrome, 2nd-degree or 3rd-degree AV block (unless internal pacer present)
- Severe hypotension / cardiogenic shock
- Hypersensitivity to diltiazem
- IV beta-blocker use within a few hours (risk of compounded AV blockade and bradycardia)
- WPW / LGL syndrome (AF or atrial flutter with accessory bypass tract) - diltiazem may paradoxically accelerate conduction down the accessory pathway, precipitating VF
- Ventricular tachycardia - Ca²⁺ channel blockers are generally ineffective and can be dangerous; this is a key pitfall when VT is misdiagnosed as PSVT
- Wide-complex tachycardia of uncertain origin - treat as VT until proven otherwise
- Roberts and Hedges', p. 3745
Adverse Effects
| Effect | Notes |
|---|---|
| Hypotension | Most important with bolus IV dosing; mitigated by pre-treating with IV calcium |
| Severe bradycardia / AV block | Especially in patients also on beta-blockers or with baseline conduction disease |
| Worsening LV dysfunction | Negative inotropy; avoid in significant systolic heart failure |
| Drug interaction - Digoxin | Both drugs can increase serum digoxin levels; risk of excess AV slowing in AF |
| Constipation | With oral (chronic) therapy |
The most dangerous scenario historically was IV diltiazem/verapamil given to a patient with VT misdiagnosed as PSVT - causing severe hemodynamic collapse.
- Goodman & Gilman, p. 252
Diltiazem vs. Verapamil in PSVT
| Feature | Diltiazem | Verapamil |
|---|---|---|
| Class | Non-DHP CCB | Non-DHP CCB |
| Effect on peripheral vasodilation | Intermediate | Least |
| Negative inotropy | Moderate | Greater |
| First-pass hepatic metabolism | Extensive | Extensive (stereoselective) |
| Hypotension risk (IV) | Less than verapamil | Greater |
| Oral dose for prophylaxis | Yes | Yes |
| Constipation | Less common | Common |
Special Considerations
- WPW with PSVT: If the tachycardia is orthodromic AVRT with a concealed or known low-risk accessory pathway, diltiazem/verapamil may be used. However, if there is overt preexcitation (delta waves) with AF/flutter, avoid all AV nodal blockers - use IV procainamide or cardioversion.
- Pregnancy: PSVT treatment in pregnancy follows the same algorithm (vagal maneuvers → adenosine → CCB); diltiazem/verapamil are options when adenosine fails.
- "Pill-in-the-pocket": For patients with recurrent PSVT and known low-risk APs, a single dose of oral beta-blocker, verapamil, or diltiazem taken at episode onset can terminate the arrhythmia.
- Long-term management: Most patients with recurrent PSVT are candidates for catheter ablation, which is curative. Diltiazem oral therapy is an alternative for those who decline ablation.
- Harrison's Principles of Internal Medicine 22E, p. 887-913
- Fuster and Hurst's The Heart, 15th Edition
Treatment for Iron deficiency anemia parenterslly in 8 th trimester
Asking for Preferences
Finding Sources
Finding Sources
Searching PubMed
parenteral iron deficiency anemia pregnancy third trimester
Reading File
Reading File
Searching PubMed
intravenous iron pregnancy anemia
Reading File
Finding Sources
Reading File
I now have comprehensive information from multiple authoritative sources. Here is the full answer:
Parenteral Iron for Iron Deficiency Anemia in the 3rd Trimester
Why Parenteral Iron is Preferred in the 3rd Trimester
Intravenous (IV) iron is the treatment of choice for all iron deficiency anemia (IDA) in the 3rd trimester (and for severe IDA with Hb < 9 g/dL in the 2nd trimester). Oral iron is avoided or insufficient at this stage because:
- There is inadequate time for GI absorption and response before delivery
- Oral iron absorption is further limited by physiologic GI changes in late pregnancy
- High iron demand in the 3rd trimester is difficult to meet with oral supplementation
- IV iron achieves target hemoglobin faster and more reliably than oral iron
Two meta-analyses confirm that after 4 weeks of treatment, Hb was significantly higher in IV-treated vs. oral-treated pregnant patients, with more patients achieving the target Hb of 11-12 g/dL and significantly fewer adverse events in the IV group.
- Rosen's Emergency Medicine, p. 839-840
- Creasy & Resnik's Maternal-Fetal Medicine, p. 1234-1240
Diagnosis First
| Lab | Significance in Pregnancy |
|---|---|
| Serum Ferritin | Most sensitive/specific marker; cutoff < 30 ng/mL (92% sensitivity, 98% specificity) |
| Hb < 11 g/dL | WHO definition of anemia in pregnancy |
| Hb < 9 g/dL | Severe IDA - warrants IV iron even in 2nd trimester |
| Hb < 7 g/dL | Consider blood transfusion |
| MCV, TIBC, transferrin | Less reliable due to plasma volume expansion in late pregnancy |
Approved Parenteral Iron Preparations
Six forms are approved in the United States. Their key differences:
| Preparation | Key Points | Notes in Pregnancy |
|---|---|---|
| Iron Sucrose | 100-300 mg per dose; slow IV injection or infusion; multiple doses needed | Most commonly used in pregnancy (used in 9/11 trials in major meta-analysis) |
| Ferric Carboxymaltose | Large single dose (up to 750-1000 mg); fewer infusions needed | Increasingly preferred - single or two-dose regimen |
| Iron Isomaltoside | High single-dose option | Safe in pregnancy |
| Low-MW Iron Dextran | 1 g single dose possible; requires 25 mg test dose first (risk of anaphylaxis) | Test dose mandatory |
| Ferumoxytol | 510-1020 mg; 1-2 doses | Monitor ≥30 min post-infusion for hypersensitivity |
| Sodium Ferric Gluconate | Multiple 125-250 mg doses | Avoided in pregnancy - contains benzyl alcohol preservative (potential fetal risk) |
- Creasy & Resnik's Maternal-Fetal Medicine, p. 1238
- Goodman & Gilman's Pharmacological Basis of Therapeutics
Dosing: Iron Sucrose (Most Common in Pregnancy)
The total iron deficit is calculated using the Ganzoni formula:
Total dose (mg) = Body weight (kg) × (Target Hb - Actual Hb) × 0.24 + 500 mg
- Target Hb: 11-12 g/dL
- Maximum per infusion: 200 mg
- Frequency: Every other day (split dosing)
Example: A 60 kg woman with Hb 8 g/dL:
60 × (12 - 8) × 0.24 + 500 = 57.6 + 500 = ~558 mg total → given as 200 mg every other day × 3 infusions
- Creasy & Resnik's, p. 1238
Contraindications / Precautions
- Not used in the 1st trimester (organogenesis concerns; iron dextran has shown fetal harm in animals)
- Severe anaphylaxis - now rare with modern preparations; test dose only required for low-MW iron dextran
- Iron dextran (high MW) is no longer recommended due to higher anaphylaxis risk
- Sodium ferric gluconate - avoid due to benzyl alcohol
Monitoring Adverse Effects
The most common adverse reactions across all IV iron preparations:
- Urticaria, pruritus
- Dyspnea
- Tachycardia
- Chills and arthralgias
- Hypotension (rare with modern preparations)
All IV iron infusions should be given in a facility equipped to manage hypersensitivity reactions. Monitor the patient for ≥30 minutes post-infusion.
Role of Erythropoietin
In cases of severe IDA unresponsive to iron therapy alone (Hb < 8.5 g/dL, failure of oral iron):
- Subcutaneous erythropoietin + oral or IV iron has been used successfully
- In one study, erythropoietin added to oral iron normalized Hb in 2 weeks in 73% of patients
- Caution: Erythropoietin carries a thromboembolism risk (already elevated in pregnancy) - use requires careful risk-benefit assessment
- Creasy & Resnik's, p. 1242
Summary: 3rd Trimester IDA Algorithm
IDA in 3rd trimester
↓
IV iron (treatment of choice)
↓
Iron Sucrose 200 mg every other day (most used)
OR Ferric Carboxymaltose (single/two-dose, convenient)
OR Iron Isomaltoside (single-dose option)
↓
Monitor Hb - expect rise of ~1 g/dL/week in severe cases
↓
If Hb <7 g/dL or no response → Blood transfusion
If Hb fails despite IV iron → Add Erythropoietin (with caution)
Recent evidence (Lancet Haematol, 2025 - PMID 40306833): Consensus guidelines now recommend IV iron as first-line (over oral) when Hb correction is urgently needed in late pregnancy, given its superior efficacy and safety profile.
Inj frrrous carboxymsltose
Finding Sources
Searching PubMed
"ferric carboxymaltose" iron deficiency anemia
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
I have comprehensive information. Here is the complete answer:
Injection Ferric Carboxymaltose (FCM)
Trade names: Injectafer (USA), Ferinject (Europe/India)
What Is It?
Ferric carboxymaltose is a 3rd-generation, high-dose parenteral iron preparation consisting of a ferric hydroxide core stabilized by a carbohydrate (carboxymaltose) shell. This structure allows controlled, slow release of iron without the risk of free labile iron toxicity, and permits rapid administration of large single doses.
- Goodman & Gilman's Pharmacological Basis of Therapeutics
Mechanism of Action
- After IV injection, FCM is rapidly cleared from circulation
- ~80% distributes to the bone marrow (primary site of erythropoiesis), with the remainder to liver and spleen
- Iron is incorporated into hemoglobin synthesis, replenishing depleted stores
- Results in: rise in serum iron → rise in serum ferritin → rise in transferrin saturation → correction of hemoglobin
Key Pharmacological Advantage
| Feature | FCM | Iron Sucrose | Iron Dextran |
|---|---|---|---|
| Max single dose | 750-1000 mg | 200 mg | 1000 mg |
| Infusion time | 15 min | 30-60 min | 60+ min |
| Test dose required | No | No | Yes |
| Number of infusions | 1-2 | 5-10 | 1 |
| Anaphylaxis risk | Very low | Very low | Highest |
| Generation | 3rd | 2nd | 1st |
Indications
- Iron deficiency anemia (IDA) with intolerance to oral iron
- Unsatisfactory response to oral iron (Hb not rising after 2 weeks)
- IDA in 3rd trimester of pregnancy (treatment of choice)
- IDA with malabsorption (post-bariatric surgery, IBD, celiac disease)
- IDA in non-dialysis-dependent CKD
- IDA in heart failure (improves exercise capacity and quality of life - FAIR-HF trial)
- Patients with ongoing blood loss too great for oral supplementation
Dosing
Standard Dosing (Adults)
| Parameter | Details |
|---|---|
| Dose 1 | 750 mg IV infusion |
| Dose 2 | 750 mg IV, at least 7 days after first dose |
| FDA-approved single dose | 1000 mg (approved 2021) |
| Infusion time | Over 15 minutes (1000 mg over 15-30 min) |
| Maximum per week | 750 mg |
| Total repletion | Usually 1500 mg over 2 infusions covers full deficit |
Dose Calculation (Ganzoni Formula)
Total iron dose (mg) = Body weight (kg) × (Target Hb - Actual Hb g/dL) × 0.24 + 500
- Target Hb: 12 g/dL (non-pregnant); 11-12 g/dL (pregnant)
In Pregnancy (3rd Trimester)
Same dosing applies. FCM is increasingly preferred over iron sucrose because fewer infusions are needed (1-2 vs. 5-10), which is more practical near delivery.
Administration
- Route: Intravenous only (IV infusion or slow IV push)
- Dilution: 750 mg in 100-250 mL normal saline (0.9% NaCl); do NOT dilute in dextrose
- Do NOT give IM - causes local staining and tissue necrosis
- No test dose required
- Observe patient for ≥30 minutes after infusion for hypersensitivity reactions
Adverse Effects
Common
- Headache, dizziness
- Nausea, abdominal pain, constipation, diarrhea
- Flushing, rash
- Injection site reactions
- Transient hypertension
Important / Clinically Significant
| Adverse Effect | Details |
|---|---|
| Hypophosphatemia | Most important unique adverse effect of FCM. Detectable within 1 week of infusion. Mechanism: FCM causes a 2-4 fold rise in FGF-23 → excessive renal phosphate wasting (phosphaturia) + inhibition of 1-alpha-hydroxylase → low 1,25-(OH)₂D. Can persist and cause osteomalacia and fractures if prolonged. Does NOT occur with ferumoxytol. |
| Severe hypotension | Rare; related to rapid injection rate |
| Hypersensitivity/anaphylaxis | Rare; manage with epinephrine, corticosteroids |
| MRI interference | IV iron can create artifacts on liver MRI; allow ≥1 week before imaging |
Hypophosphatemia is FCM's distinguishing complication - monitor serum phosphate after infusion, especially with repeat dosing. This is a key exam point. [Systematic review PMID 39935027, 2025]
Contraindications
- Known hypersensitivity to FCM or any component
- Iron overload states (hemochromatosis, hemosiderosis)
- Anemia NOT due to iron deficiency (e.g., hemolytic anemia, megaloblastic anemia)
- First trimester of pregnancy (avoid; use from 2nd trimester onward when needed)
- Non-iron deficiency anemia
Monitoring
| Parameter | When |
|---|---|
| Hemoglobin, hematocrit | Baseline, then 4 weeks post-infusion |
| Serum ferritin, transferrin saturation | Baseline, post-infusion |
| Serum phosphate | 1 week post-infusion (watch for FCM-induced hypophosphatemia) |
| Blood pressure | During and after infusion |
| Signs of hypersensitivity | ≥30 min post-infusion |
Comparison: FCM vs. Iron Sucrose in Pregnancy
| FCM (Injectafer) | Iron Sucrose (Venofer) | |
|---|---|---|
| Dose per infusion | 750-1000 mg | 100-200 mg |
| Total infusions needed | 1-2 | 5-10 |
| Infusion time | 15 min | 30-60 min |
| Hypophosphatemia risk | Yes | No |
| Preferred use | When convenience matters, near term | Standard in most trials |
| Evidence in pregnancy | Growing | Most RCT data (9/11 trials) |
Summary Points
- FCM is a high-dose, single-infusion parenteral iron ideal when rapid or convenient repletion is needed
- No test dose required, very low anaphylaxis risk
- 3rd trimester IDA - FCM is an excellent choice (1-2 infusions vs. multiple for iron sucrose)
- Unique risk: hypophosphatemia via FGF-23 elevation - monitor serum phosphate at 1 week; can cause osteomalacia/fractures if prolonged
- Does NOT interfere with erythropoiesis assessment unlike ferumoxytol's MRI effect
- In heart failure with iron deficiency, FCM improves exercise capacity and symptoms (FAIR-HF trial)
- Goodman & Gilman's Pharmacological Basis of Therapeutics
- Goldman-Cecil Medicine, p. 3116-3118
- The Washington Manual of Medical Therapeutics, p. 864-866
- Creasy & Resnik's Maternal-Fetal Medicine, p. 1238
- Goldman-Cecil Medicine, p. 1315-1316 (hypophosphatemia)
Can oral diltiazem and amiodarone be given together in VT patients?
Finding Sources
Finding Sources
Searching PubMed
diltiazem amiodarone combination ventricular tachycardia
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
I now have the critical information. The key Braunwald's quote is definitive. Let me compile the complete answer.
Oral Diltiazem + Amiodarone in VT Patients
Direct Answer: Generally Contraindicated / Strongly Cautioned Against
This combination should not be used in VT patients under most circumstances. Here is the full reasoning:
Why Diltiazem is Contraindicated in VT
First and most importantly - diltiazem itself is contraindicated in VT:
"Both agents [verapamil and diltiazem] are contraindicated for wide-complex tachyarrhythmias." - Tintinalli's Emergency Medicine
"Ca²⁺ channel blockers usually are not effective in VT. This was a particular problem when the drugs were used mistakenly in patients with VT misdiagnosed as PSVT, causing severe hemodynamic collapse." - Goodman & Gilman's
Why diltiazem fails in VT:
- VT is driven by abnormal ventricular automaticity or ventricular reentry circuits - these do NOT depend on the AV node
- Diltiazem (Class IV) works by blocking the AV node - it has no direct effect on ventricular myocardium at therapeutic doses
- In VT, diltiazem causes vasodilation + negative inotropy → hemodynamic collapse without terminating the arrhythmia
The Drug Interaction: Amiodarone + Diltiazem
Even if we set aside the VT contraindication, the combination itself carries serious interaction risks:
| Mechanism | Amiodarone | Diltiazem | Combined Effect |
|---|---|---|---|
| AV nodal conduction | Slows (Class III + blocks L-Ca²⁺ channels + antiadrenergic) | Slows (L-Ca²⁺ channel block) | Additive/synergistic AV block |
| Sinus node automaticity | Suppresses | Suppresses | Additive sinus bradycardia |
| Negative inotropy | Mild (IV > oral) | Moderate | Additive myocardial depression |
| Vasodilation / hypotension | Moderate | Moderate | Additive hypotension |
| CYP3A4 metabolism | Inhibits CYP3A4 | Metabolized by CYP3A4 | Amiodarone raises diltiazem plasma levels |
"Drugs with synergistic actions, such as beta blockers or calcium channel blockers, must be given cautiously [with amiodarone]."
- Braunwald's Heart Disease, 15th Edition, p. 466
"CCB and amiodarone exacerbates sick sinus syndrome and AV block."
- Brenner and Rector's The Kidney
"β-adrenoceptor antagonists, calcium-channel blockers, digoxin, sotalol, and amiodarone are some of the agents that most commonly cause significant sinus bradycardia or AV block."
- Fuster and Hurst's The Heart, 15th Edition
Amiodarone's Multi-Channel Profile Explains the Risk
Amiodarone is a unique antiarrhythmic - it acts on ALL four Vaughan Williams classes:
| Action | Class | Relevance to Interaction |
|---|---|---|
| Na⁺ channel block | I | - |
| Antiadrenergic (β-block) | II | Additive bradycardia with diltiazem |
| K⁺ channel block (prolongs APD/QT) | III | - |
| L-type Ca²⁺ channel block | IV | Direct overlap with diltiazem's mechanism |
Since amiodarone itself already blocks L-type Ca²⁺ channels (AV node) AND has beta-blocking activity, adding diltiazem (another Ca²⁺ channel blocker) results in double AV nodal blockade - greatly increasing the risk of:
- High-degree AV block (2nd or 3rd degree)
- Severe sinus bradycardia / sinus arrest
- Hemodynamic instability
Pharmacokinetic Interaction (CYP3A4)
Amiodarone is a potent inhibitor of CYP3A4, which is the primary enzyme responsible for diltiazem's hepatic metabolism. This means:
- Amiodarone increases diltiazem plasma concentrations by reducing its clearance
- The pharmacodynamic interaction (additive depression) is therefore amplified by a pharmacokinetic interaction
- Toxicity can occur at doses of diltiazem that would otherwise be safe
What Should Be Used for VT Instead?
| Setting | Preferred Drug |
|---|---|
| Acute VT (stable) | IV Amiodarone (150 mg over 10 min), Procainamide, Lidocaine |
| Acute VT (unstable) | Immediate DC cardioversion |
| Chronic VT suppression (oral) | Amiodarone alone, Mexiletine (often combined WITH amiodarone safely), Sotalol, Beta-blockers |
| If on amiodarone, rate control of concurrent AF needed | Digoxin (cautiously) - beta-blockers at reduced dose with careful monitoring |
Mexiletine + amiodarone is a recognised and safe combination for refractory VT suppression - mexiletine (Class IB) has complementary rather than overlapping mechanisms with amiodarone.
- Lippincott Illustrated Reviews: Pharmacology
Summary
| Question | Answer |
|---|---|
| Is diltiazem useful in VT? | No - no efficacy; causes hemodynamic collapse |
| Can amiodarone + diltiazem be combined? | Avoid - synergistic AV/sinus node suppression + CYP3A4 pharmacokinetic interaction |
| What is the risk? | High-degree AV block, severe bradycardia, sinus arrest, hypotension |
| Any exception? | Only with extreme caution, close monitoring, and a compelling indication separate from VT (e.g., controlling AF rate in a patient already established on amiodarone) - never together for VT management |
| Safe VT combination with amiodarone? | Mexiletine + amiodarone (complementary mechanisms) |
- Braunwald's Heart Disease 15th Ed, p. 465-466
- Goodman & Gilman's Pharmacological Basis of Therapeutics
- Tintinalli's Emergency Medicine
- Fuster and Hurst's The Heart, 15th Edition
- Brenner and Rector's The Kidney
Indication of using amiodarone
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
I have all the information needed. Now let me compile the comprehensive answer.
Indications for Amiodarone
Amiodarone is a Class III antiarrhythmic (Vaughan Williams) with the unique property of acting on all four antiarrhythmic classes simultaneously, making it the broadest-spectrum antiarrhythmic drug available.
Vaughan Williams Classification
| Class | Mechanism | Amiodarone's Action |
|---|---|---|
| I | Na⁺ channel block | Yes - use-dependent INa block |
| II | Beta-adrenergic block | Yes - noncompetitive α and β antagonism |
| III | K⁺ channel block (prolongs APD/ERP) | Yes - IKr block; primary mechanism |
| IV | L-type Ca²⁺ channel block | Yes - slows AV node, sinus rate |
This multi-channel profile gives amiodarone activity against virtually every type of arrhythmia mechanism.
FDA-Approved (Labeled) Indications
"Amiodarone is approved by the FDA for the treatment of patients with life-threatening ventricular tachyarrhythmias when other drugs are ineffective or not tolerated."
- Braunwald's Heart Disease, 15th Ed.
| Indication | Route | Notes |
|---|---|---|
| Recurrent hemodynamically unstable VT | IV / Oral | Primary FDA indication; first-line when other drugs fail |
| Recurrent VF | IV / Oral | Life-threatening; drugs of last resort apply |
| VT/VF refractory to defibrillation | IV | ACLS algorithm - only 2 drugs are recommended in cardiac arrest: epinephrine and amiodarone |
| Ventricular and supraventricular dysrhythmias | IV / Oral | Broader approval per Rosen's |
Off-Label (Widely Used) Indications
Despite the narrow FDA label, amiodarone is extensively used off-label due to its broad efficacy:
Ventricular Arrhythmias
| Indication | Details |
|---|---|
| Pulseless VT / VF (cardiac arrest) | IV 300 mg bolus; one of only two ACLS drugs recommended |
| Stable VT (acute) | IV 150 mg over 10 min - first-line drug treatment |
| VT storm | IV loading; suppresses incessant VT |
| ICD patients with frequent shocks | Oral - reduces frequency of VT/VF episodes and ICD discharges |
| VT with structural heart disease | Oral maintenance; often combined with mexiletine |
| Post-MI ventricular arrhythmia suppression | Oral - though ICD is superior for survival |
Supraventricular Arrhythmias
| Indication | Details |
|---|---|
| Atrial fibrillation - rate control | IV or oral; slows ventricular rate via AV nodal blockade |
| Atrial fibrillation - rhythm control | IV chemical cardioversion; oral maintenance of sinus rhythm |
| Atrial flutter - rate/rhythm control | Similar to AF |
| Postoperative AF prevention | IV/oral perioperative use (e.g., after cardiac surgery) |
| WPW with AF | Safe (unlike digoxin/CCBs) - blocks accessory pathway conduction |
| AVNRT / AVRT (refractory) | When adenosine and CCBs fail |
| Junctional tachycardia | Refractory cases |
Acute vs. Chronic Dosing
IV (Acute)
| Scenario | Dose |
|---|---|
| Cardiac arrest (pulseless VT/VF) | 300 mg IV push; can repeat 150 mg once |
| Stable VT / SVT | 150 mg IV over 10 min |
| Loading infusion | 1 mg/min × 6 hours, then 0.5 mg/min × 18 hours |
| Breakthrough VT/VF on infusion | Supplemental 150 mg over 10 min |
| Max 24-hour IV dose | ~2.2 g |
Oral (Chronic)
| Phase | Dose |
|---|---|
| Loading | 800-1200 mg/day × 1-3 weeks |
| Tapering | 600-800 mg/day × 1-2 months |
| Maintenance | 200 mg/day (lowest effective dose) |
| Minimum effective | 100 mg every other day in some patients |
Amiodarone has an extremely long half-life (40-55 days). Steady-state without loading takes ~265 days. Loading doses are essential to achieve rapid effect.
- Braunwald's Heart Disease, 15th Ed.
Why Amiodarone is Preferred Despite Its Toxicity
| Advantage | Explanation |
|---|---|
| Effective in structural heart disease | Does not suppress LV ejection fraction at oral doses (unlike many antiarrhythmics) |
| Very low proarrhythmic risk | Despite QT prolongation, TdP occurs in only 1-2% (due to multi-channel block preventing reentry) |
| No reverse use-dependence | Effect maintained at fast rates (unlike sotalol/dofetilide) |
| Works in ischemic/scarred myocardium | Effective even with heterogeneous conduction tissue |
| Reduces ICD shocks | Slows VT rate; may drop rate below ICD detection threshold (requires device reprogramming) |
| Safe in reduced EF | IV use with caution; oral use does not worsen EF |
Key Contraindications
| Contraindication | Reason |
|---|---|
| Sinus node dysfunction / sick sinus syndrome (without pacemaker) | Worsens bradycardia / sinus arrest |
| 2nd or 3rd degree AV block (without pacemaker) | Additive AV block |
| Cardiogenic shock | Vasodilation + negative chronotropy worsen shock |
| Severe hypersensitivity to iodine | 37% iodine by weight |
| Pregnancy (relative) | Class D - crosses placenta (10-50%); use only if no alternative |
| Breastfeeding | Excreted in breast milk - avoid |
Important Adverse Effects (Brief Summary)
| System | Effect |
|---|---|
| Pulmonary | Pulmonary toxicity (most serious) - pneumonitis/fibrosis; up to 10% mortality if missed |
| Thyroid | Hypothyroidism (2-4%) or hyperthyroidism (1-2%) - 37% iodine content |
| Cardiac | Bradycardia (~2%), AV block, TdP (1-2%), hypotension (IV) |
| Hepatic | Elevated LFTs (common); cirrhosis (rare) |
| Neurologic | Tremor, peripheral neuropathy, ataxia |
| Skin | Photosensitivity, blue-grey discolouration (long-term) |
| Eyes | Corneal microdeposits (nearly universal, usually asymptomatic); optic neuropathy (rare) |
| Drug interactions | ↑ Warfarin (INR), ↑ Digoxin levels - reduce doses by 1/3 to 1/2 |
Monitoring (Braunwald's Recommended Schedule)
| Test | Timing |
|---|---|
| ECG | Baseline + every clinic visit + at least annually |
| Thyroid function (TSH) | Baseline, then every 4-6 months |
| Liver function tests | Baseline, then every 6 months |
| Chest X-ray | Baseline, then annually |
| Pulmonary function (DLCO) | Baseline; repeat if symptoms develop |
| Ophthalmology | Baseline if visual impairment; annually or for any vision change |
Summary in One Table
| Setting | Amiodarone Role |
|---|---|
| Pulseless VT/VF (cardiac arrest) | First-line IV (ACLS) |
| Hemodynamically stable VT (acute) | First-line IV |
| Recurrent VT/VF prevention (chronic) | Oral - especially with structural heart disease |
| AF rate/rhythm control | IV or Oral (widely used off-label) |
| ICD patients with frequent shocks | Oral adjunct |
| Post-cardiac surgery AF prevention | IV/oral perioperative |
| VT with low EF | Safe oral option (does not suppress EF) |
- Braunwald's Heart Disease, 15th Ed., p. 463-466
- Rosen's Emergency Medicine, p. 1438-1447
- Goodman & Gilman's Pharmacological Basis of Therapeutics
- Roberts and Hedges' Clinical Procedures in Emergency Medicine
Labetalol dosing for hypertensive urgency
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
I now have comprehensive, well-sourced dosing data from multiple textbooks. Here is the complete answer:
Labetalol Dosing for Hypertensive Urgency
Urgency vs. Emergency - Key Distinction First
| Hypertensive Urgency | Hypertensive Emergency | |
|---|---|---|
| BP | Severely elevated (usually >180/120 mmHg) | Severely elevated |
| Target organ damage | Absent | Present (encephalopathy, AKI, dissection, pulmonary edema, etc.) |
| Treatment route | Oral preferred | IV required |
| BP reduction rate | Gradual - over 24-48 hours | Controlled reduction over minutes to hours |
| Setting | Outpatient / ED discharge | ICU / monitored bed |
Rapid BP reduction in urgency is not recommended - overly aggressive lowering risks cerebral, coronary, or renal ischemia. The goal is a controlled, gradual decrease.
Mechanism of Labetalol
Labetalol is a racemic mixture with both:
- α₁-adrenergic blockade → vasodilation, reduces peripheral resistance
- Non-selective β-blockade → reduces heart rate and cardiac output
Oral β:α ratio = 3:1 | IV β:α ratio = 7:1
This dual action lowers BP without reflex tachycardia, making it ideal for hypertensive crises.
- Katzung's Basic and Clinical Pharmacology, 16th Ed.
ORAL Labetalol - Hypertensive Urgency
| Parameter | Details |
|---|---|
| Initial dose | 200 mg orally |
| Repeat dose | 200-400 mg orally after 6-12 hours depending on BP response |
| When IV not yet available | 200 mg oral labetalol can be used as a bridging option |
| Onset of action (oral) | 20-120 minutes |
| Duration of action | 8-12 hours |
| Chronic oral dosing range | 200-2400 mg/day in divided doses |
| Typical chronic dose | 200 mg twice daily (starting); max 800 mg three times daily |
"When treatment for acute-onset severe HTN is needed and IV access has not yet been initiated, a 200 mg dose of labetalol can be administered orally."
- Swanson's Family Medicine Review
- The Washington Manual of Medical Therapeutics, p. 88
- Textbook of Family Medicine, 9th Ed.
IV Labetalol - Hypertensive Emergency
(Included for completeness and comparison)
Bolus Dosing (Preferred - due to 5-8 hour half-life)
| Dose | Frequency | Max Cumulative |
|---|---|---|
| 20-80 mg IV bolus | Every 5-10 minutes | 300 mg total |
| Onset | 5-10 min | - |
| Duration | 3-6 hours | - |
Continuous Infusion (Alternative)
| Details | |
|---|---|
| Rate | 0.5-2 mg/min IV infusion |
| Titrate to BP response | - |
| Transition to oral | When supine DBP begins to rise → start oral 200 mg, then 200-400 mg in 6-12 hours |
"Because the half-life of labetalol is 5-8 hours, intermittent IV bolus dosing may be preferable to IV infusion."
- Washington Manual of Medical Therapeutics
Pediatric IV Dosing (for reference)
| Dose | |
|---|---|
| Bolus | 0.2-1 mg/kg (max 40 mg) |
| Infusion | 0.25-1 mg/kg/hr (max dose per protocol) |
- Harriet Lane Handbook, 23rd Ed.
Comparison with Other Agents for Hypertensive Urgency
| Drug | Route | Onset | Dose | Notes |
|---|---|---|---|---|
| Labetalol | Oral | 20-120 min | 200 mg, repeat 200-400 mg in 6-12 h | No reflex tachycardia; avoid in asthma/COPD, HF |
| Amlodipine | Oral | 30-60 min | 5-10 mg | Long-acting; useful for gradual reduction |
| Clonidine | Oral | 30-60 min | 0.1-0.2 mg; repeat q1h (max 0.6 mg) | Rebound hypertension if stopped abruptly |
| Captopril | Oral/SL | 15-30 min | 25 mg | Avoid in bilateral RAS, pregnancy |
| Nifedipine (IR) | Oral | 15-30 min | 10 mg | Avoid sublingual - unpredictable drop, stroke risk |
Special Indications Where Labetalol is Drug of Choice
| Situation | Why Labetalol |
|---|---|
| Pregnancy / preeclampsia | Safe in pregnancy; drug of choice for IV route |
| Pheochromocytoma | Dual α+β block prevents paradoxical hypertension (give only after alpha blockade established) |
| Aortic dissection | Reduces rate-pressure product; can combine with nitroprusside |
| Post-cardiac surgery hypertension | Effective for adrenergic excess |
| Clonidine withdrawal | Manages rebound adrenergic surge |
| Cocaine-induced hypertension | Controversial (non-selective β-block may leave α-receptors unopposed) - many experts prefer phentolamine |
Contraindications
| Contraindication | Reason |
|---|---|
| Bronchial asthma / COPD | Non-selective β-block → bronchospasm |
| Decompensated heart failure | Negative inotropy + chronotropy worsens failure |
| 2nd/3rd degree AV block | Additive conduction depression |
| Severe bradycardia | β-blockade reduces heart rate further |
| Cardiogenic shock | Reduces cardiac output |
| Severe aortic stenosis | Cannot compensate for reduced SVR |
| Patients already on α- or β-blockers | May be ineffective or cause additive toxicity |
Key Adverse Effects
| Effect | Notes |
|---|---|
| Postural hypotension | Especially with IV; treat patients supine |
| Bradycardia / heart block | Monitor ECG |
| Bronchospasm | Avoid in asthma |
| Nausea, vomiting, scalp tingling | Common with IV bolus |
| Fatigue, dizziness | With chronic oral use |
Summary: Dosing at a Glance
HYPERTENSIVE URGENCY (Oral):
→ Labetalol 200 mg PO
→ Repeat 200-400 mg PO after 6-12 hours if BP not controlled
→ Goal: Gradual reduction over 24-48 hours
HYPERTENSIVE EMERGENCY (IV):
→ Labetalol 20-80 mg IV bolus q5-10 min (max 300 mg total)
→ OR Infusion: 0.5-2 mg/min
→ Transition to oral 200 mg when stable
- The Washington Manual of Medical Therapeutics, p. 87-89
- Katzung's Basic and Clinical Pharmacology, 16th Ed., p. 3474-3478
- Swanson's Family Medicine Review
- Textbook of Family Medicine, 9th Ed.
- Harriet Lane Handbook, 23rd Ed.
Urticaria pictures and management
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Loading Image
Loading Image
Reading File
I now have all I need - 4 clinical images and comprehensive management data from multiple authoritative sources. Here is the complete answer:
Urticaria - Pictures and Management
Definition and Key Features
Urticaria (hives) is one of the most common cutaneous reaction patterns, affecting 15-20% of the population at some point in their lifetime. It is characterized by:
- Wheals - transient, edematous, blanching papules or plaques
- Pruritus - invariably present and often severe
- Wheal and flare - pale center with surrounding erythematous border
- Transient - individual lesions last < 24 hours, though new lesions may continuously appear
- Can be annular, serpiginous, or confluent in pattern
Clinical Photographs
Adult Urticaria - Characteristic wheals on arm

Urticaria - Large confluent wheals (adult)

Pediatric Urticaria - Oval wheals covering torso and arms

Classification
| Type | Duration | Key Features |
|---|---|---|
| Acute urticaria | < 6 weeks | Often IgE-mediated; identifiable trigger common; more in children |
| Chronic urticaria | ≥ 6 weeks | Trigger often unknown; more in women, 3rd-4th decade; 50% last >5 years |
| Physical urticaria | Triggered by physical stimuli | Cold, heat, pressure, solar, cholinergic, aquagenic |
| Urticarial vasculitis | Persistent >24h | Antihistamine-resistant; skin biopsy required |
Causes / Triggers
| Category | Examples |
|---|---|
| Drugs | Penicillin (most common), aspirin/NSAIDs, opioids, contrast dye |
| Foods | Seafood, tree nuts, peanuts, eggs, strawberries, lobster (histamine-releasing) |
| Infections | Rhinovirus, rotavirus, hepatitis, EBV, Coxsackievirus; occult bacterial/fungal/parasitic |
| Contact | Latex, animal dander/saliva, plants, cosmetics, topical medications |
| Physical | Cold, heat, pressure, exercise (cholinergic), sunlight (solar), water (aquagenic) |
| Autoimmune | Functional IgE autoantibodies against FcεRI or IgE; thyroid autoimmunity |
| Idiopathic | Chronic spontaneous urticaria - most common category |
Aspirin and NSAIDs cause urticaria by a non-immunologic mechanism and the effect can persist for weeks after ingestion.
Pathophysiology
Local degranulation of mast cells in the dermis releases:
- Histamine (primary mediator)
- Bradykinin, kallikrein, acetylcholine
- Slow-reacting substance of anaphylaxis (leukotrienes)
→ Vasodilation + increased vascular permeability → dermal edema → wheal formation
Mechanisms:
- IgE-mediated (Type I hypersensitivity) - allergen cross-links IgE on mast cells
- Non-IgE mediated - direct mast cell degranulation (drugs, foods)
- Autoimmune - anti-FcεRI or anti-IgE autoantibodies
Management
Step 1 - Acute Urticaria (Immediate Management)
| Priority | Action |
|---|---|
| Anaphylaxis? | If urticaria + hypotension/bronchospasm → IM Epinephrine 0.3-0.5 mg (1:1000) immediately |
| Remove trigger | Stop offending drug, food, or physical stimulus |
| First-line | H1 antihistamine |
Step-Up Treatment Algorithm for Chronic Urticaria
(EAACI/GALEN/EDF/WAO and AAAAI/ACAAI Guidelines)
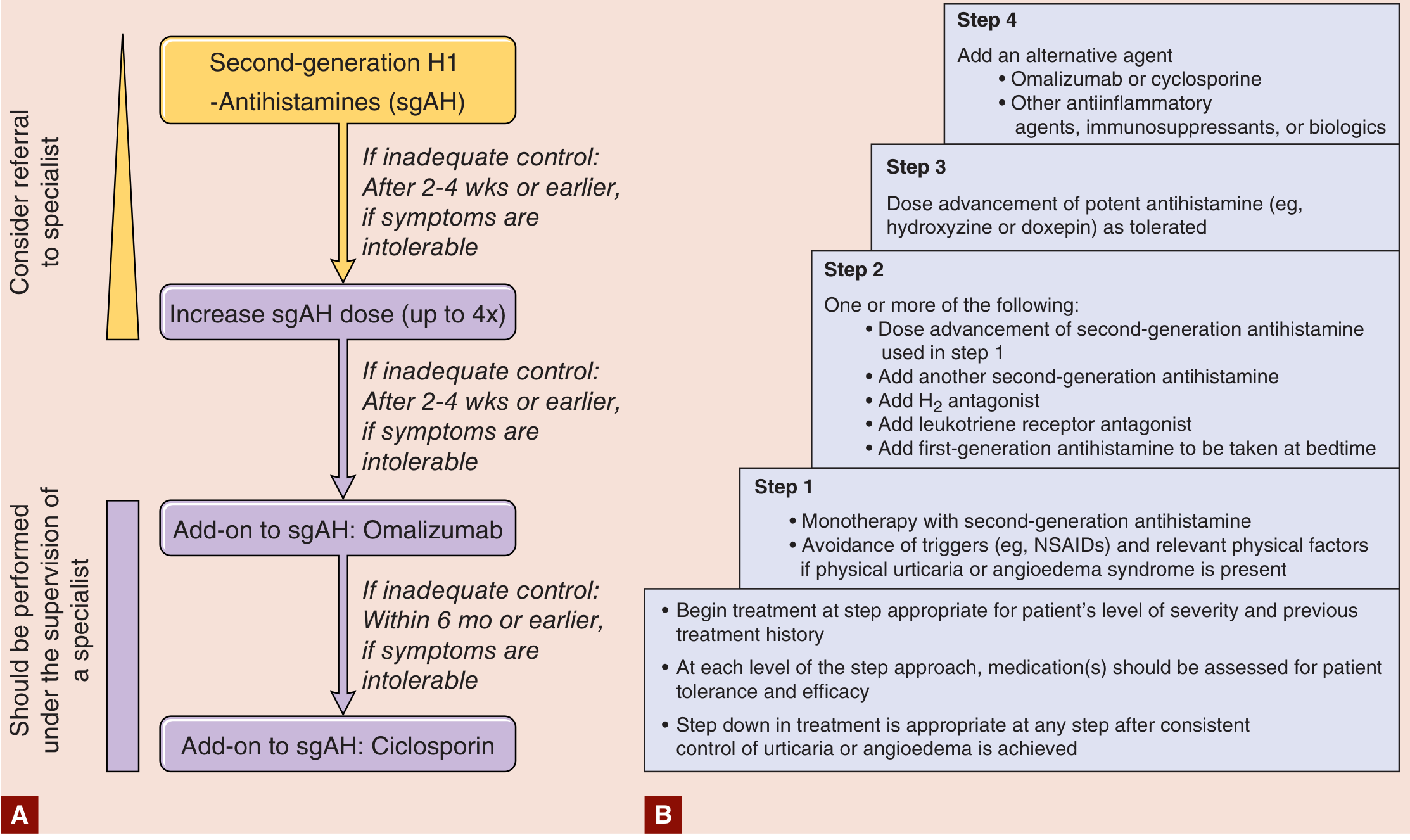
Pharmacological Treatment by Step
Step 1 - Second-Generation (Non-Sedating) H1 Antihistamines - First Line
| Drug | Dose | Notes |
|---|---|---|
| Cetirizine | 10-20 mg/day | Mild sedation; fast onset |
| Fexofenadine | 180 mg/day | Non-sedating; preferred daytime |
| Loratadine | 10-20 mg/day | Non-sedating; once daily |
| Levocetirizine | 5 mg/day | Most potent of this class |
| Bilastine / Rupatadine | 20 mg/day | Newer agents; used in Europe |
Step 2 - If Inadequate Control after 2-4 Weeks
- Increase sgAH dose up to 4× standard dose (e.g., cetirizine 40 mg/day)
- Add H2 blocker (ranitidine, famotidine) - adjunct to H1, not monotherapy
- Add leukotriene receptor antagonist (montelukast) - especially if NSAID-induced
- Add first-generation antihistamine at bedtime (hydroxyzine, diphenhydramine) for nocturnal pruritus
- Doxepin 10-25 mg at night - has both H1 and H2 blocking effects
Step 3 (Specialist Supervision) - Omalizumab
- Omalizumab 150-300 mg SC every 4 weeks
- Anti-IgE monoclonal antibody
- Highly effective in chronic spontaneous urticaria refractory to antihistamines
- Approved for chronic urticaria; significant evidence base
Step 4 - Ciclosporin (Cyclosporine)
- Ciclosporin 3-5 mg/kg/day
- For antihistamine + omalizumab-refractory cases
- Requires specialist supervision; monitor BP and renal function
Corticosteroids
| Use | Dose | Duration |
|---|---|---|
| Widespread acute urticaria / angioedema | Prednisone 40-60 mg/day | 5-7 days |
| Moderate-severe urticaria | Prednisone 1 mg/kg/day (up to 60 mg) | Short course with taper |
| Chronic urticaria maintenance | Not recommended | Avoid long-term use |
Note: A randomized ED trial of 100 adults showed no additional benefit of adding prednisone to levocetirizine for acute urticaria of <24 hours duration.
- Tintinalli's Emergency Medicine
Refractory / Special Cases
| Situation | Agent |
|---|---|
| Cholinergic urticaria | Nonsedating antihistamines; avoid triggers |
| Cold urticaria | Antihistamine 30-60 min before cold exposure; cyproheptadine |
| Solar urticaria | Antihistamines; phototherapy for tolerance induction |
| Pressure urticaria | Often antihistamine-resistant; low-dose systemic steroids |
| Urticarial vasculitis | Systemic steroids; immunosuppressants (not antihistamines alone) |
| Hereditary angioedema (HAE) | Icatibant, ecallantide, C1-INH concentrate (NOT antihistamines) |
| ACE-inhibitor angioedema | Stop ACE inhibitor; icatibant may help |
Summary Algorithm
Urticaria
↓
Anaphylaxis? → YES → IM Epinephrine immediately
↓ NO
Remove trigger + Start 2nd-gen H1 antihistamine
↓ Inadequate at 2-4 weeks
↑ Dose up to 4× + Add H2 blocker / montelukast / bedtime sedating AH
↓ Still inadequate
Add Omalizumab (specialist)
↓ Still inadequate
Add Ciclosporin (specialist)
↓
Short course steroids for severe flares (not chronic use)
Chronic urticaria almost always resolves with time. Reassure patients - 50% resolve within 1 year, 80-90% within 5 years. Trigger avoidance and antihistamine control are the cornerstones of treatment.
- Fitzpatrick's Dermatology, Vols 1-2
- Tintinalli's Emergency Medicine, p. 1686-1687
- Rosen's Emergency Medicine, p. 1831-1850
- Goldman-Cecil Medicine, p. 4592-4598
PMOS DIAGNOSIS AND MANAGEMENT
Asking for Preferences
This is a shared conversation. Sign in to Orris to start your own chat.