Pheochromocytoma in detail as I'm 3rd year pg medicine student appearing fir exam
pheochromocytoma diagnosis management
Pheochromocytoma - Comprehensive PG Medicine Notes
Definition & Overview
- Can cause fatal hypertensive crises despite standard treatment
-
10% are malignant at diagnosis
- Specific therapy is curative
- 40% are familial - affects family members
The Classic "Rule of 10s" (Robbins)
| Feature | ~10% |
|---|---|
| Extra-adrenal (paragangliomas) | 10% |
| Bilateral | 10% (up to 50% in familial syndromes) |
| Malignant | 10% (higher in extra-adrenal: up to 20%) |
| Not associated with hypertension | 10% |
| In children | 10% |
| Familial | Actually >40% by modern data |
| Recurrent after surgery | 10% |
Note: The classic "10% rule" now applies mainly to sporadic cases. Familial disease has much higher rates of bilaterality and malignancy. - Robbins & Kumar Basic Pathology
Anatomy & Location
- ~90% in or adjacent to the adrenal medulla
- Extra-adrenal sites: organ of Zuckerkandl (at aortic bifurcation or origin of inferior mesenteric artery), carotid body, urinary bladder, thorax
- Bladder paraganglioma causes classic micturition headache and syncope (episodic symptoms triggered by urination + painless hematuria)
- Campbell Walsh Wein Urology - Most extra-adrenal tumors are in or near the organ of Zuckerkandl
Genetics and Familial Syndromes
Key Syndromes
| Syndrome | Gene | Pheo Frequency | Other Features |
|---|---|---|---|
| MEN2A | RET proto-oncogene | ~50%, usually bilateral | Medullary thyroid carcinoma, parathyroid adenoma, cutaneous lichen amyloidosis |
| MEN2B | RET | Usually bilateral | MTC, submucosal neuromas, hyperplastic corneal nerves, marfanoid habitus, Hirschsprung disease |
| Von Hippel-Lindau Type 2 | VHL (chr 3p25-26) | ~20% | Retinal/cerebellar hemangioblastomas, clear cell RCC, pancreatic NETs |
| Neurofibromatosis Type 1 | NF1 | ~2% | Café-au-lait spots, neurofibromas, Lisch nodules, axillary freckling |
| SDH-related (SDHB, SDHC, SDHD) | Succinate dehydrogenase complex | Variable | SDHB: high malignancy risk; paragangliomas common |
| MAX, TMEM127, HIF2A | Various | Variable | Familial bilateral pheochromocytoma |
- Café-au-lait spots + neurofibromas → NF1
- Retinal hemangiomas → VHL
- Marfanoid habitus + submucosal neuromas → MEN2B
- Port wine stains, subungual fibromas, ash-leaf patches, adenoma sebaceum → Tuberous sclerosis
Pathogenesis
- RET, NF1 - enhance growth factor receptor signaling
- VHL, SDH subunits, EPAS1/HIF2A - increased activity of hypoxia-inducible factors (HIFs)
- Robbins & Kumar Basic Pathology
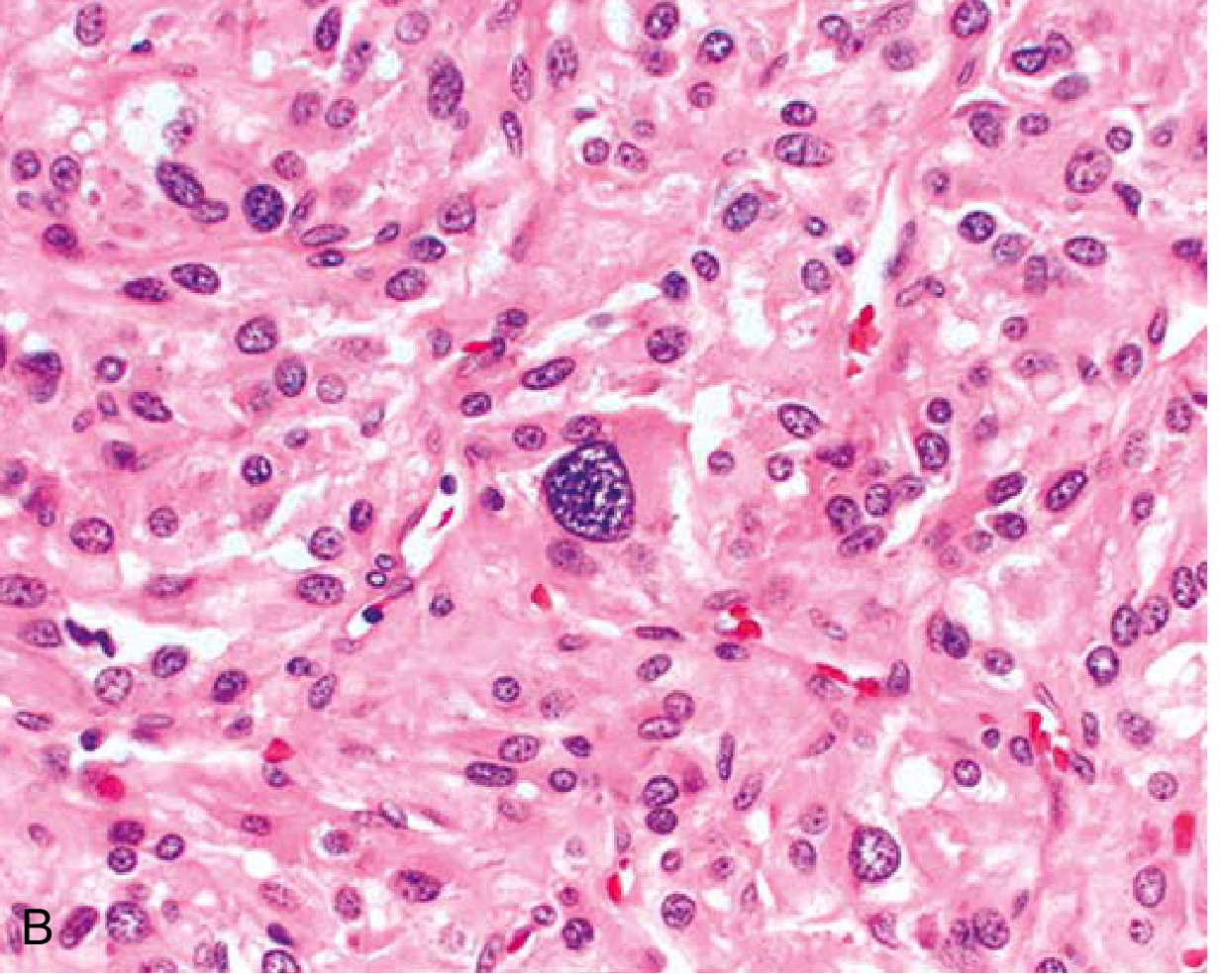
Morphology (Pathology - Robbins)
- Range from small circumscribed lesions to large hemorrhagic masses (several kg)
- Cut surface: yellow-tan, well-defined; compress adjacent adrenal gland
- Larger lesions: hemorrhagic, necrotic, cystic
- Chromaffin reaction: fresh tissue turns dark brown with potassium dichromate - reacts with catecholamines
- Polygonal to spindle-shaped chromaffin cells in small nests ("zellballen pattern") separated by rich vascular network
- Cytoplasm: finely granular (catecholamine granules)
- Granules highlighted by silver stains (Grimelius)
- EM: membrane-bound electron-dense granules containing catecholamines
Clinical Features
Classic Triad (found in ~95% of cases in large series):
- Headache (pulsating, severe)
- Sweating (profuse, generalized)
- Palpitations/Tachycardia
Hypertension Patterns:
- Sustained hypertension - most common
- ~2/3 also have paroxysmal episodes on top of sustained hypertension
- ~10% have purely paroxysmal hypertension
- ~10% are normotensive (often incidentalomas)
Paroxysmal Episodes ("Spells"):
Full Symptom Spectrum (Goldman-Cecil):
| Symptoms | Notes |
|---|---|
| Headache | Most common |
| Diaphoresis | |
| Palpitations | |
| Tremor | |
| Pallor | (NOT flushing - flushing is atypical) |
| Weight loss | |
| Hyperglycemia/DM | Alpha-adrenergic inhibition of insulin release |
| Cold hands and feet | |
| Constipation/megacolon | |
| Orthostatic hypotension | |
| Dilated or hypertrophic cardiomyopathy | Reversible after resection! |
| Erythrocytosis | |
| Livedo reticularis | |
| Painless hematuria | Bladder paraganglioma |
Exam trap: Flushing is NOT typical of pheochromocytoma. Flushing occurs in carcinoid, mastocytosis, menopause.
When to Suspect Pheochromocytoma (Goldman-Cecil Indications):
- Hyperadrenergic spells (nonexertional palpitations, diaphoresis, headache, tremor, pallor)
- Resistant hypertension
- Familial syndrome (MEN2, NF1, VHL) predisposing to PPGL
- Family history of pheochromocytoma
- Hypertension + diabetes
- Pressor response during anesthesia, surgery, or angiography
- Onset of hypertension before age 20 years
- Idiopathic dilated cardiomyopathy
- Incidentally discovered adrenal mass (incidentaloma)
Biochemical Diagnosis
First-Line Test:
Second-Line / Confirmatory:
| Test | Sensitivity | Notes |
|---|---|---|
| Plasma free metanephrines | ~99% | Best to rule OUT |
| 24h urine fractionated metanephrines | >97% | Best overall balance |
| 24h urine VMA | ~80% | Older test, less sensitive |
| Plasma catecholamines | Lower | Less reliable than metanephrines |
Imaging / Localization
CT Scan (First-Line for Localization):
- Sensitivity 90-100%
- Pheochromocytoma on non-contrast CT: HU >10 (commonly 40-50 HU; unlike benign adenomas which are <10 HU due to lipid content)
- Vigorous early contrast enhancement with <60% washout in venous phase
- Appearance: homogeneous (small) or heterogeneous/necrotic/cystic (large)
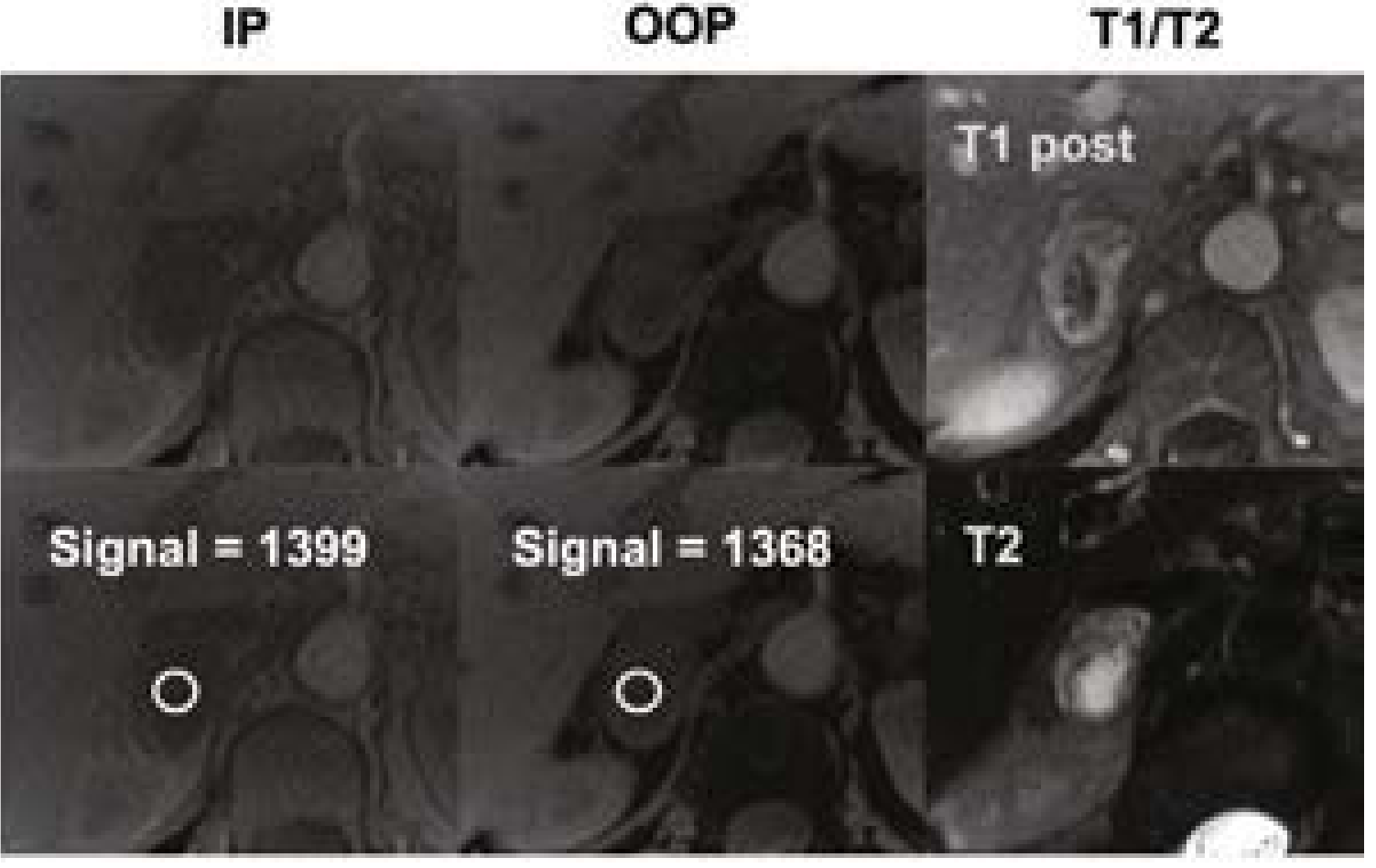
MRI (Preferred in Pregnancy, Children, Contrast Allergy):
- Classic finding: Bright (hyperintense) on T2-weighted images - "light bulb sign" - due to high vascularity and water content
- Higher sensitivity than CT for extra-adrenal paragangliomas
- Not affected by radiation (important in pediatrics and pregnancy)
Functional Imaging (for metastatic/recurrent/extra-adrenal):
- ¹²³I-MIBG (meta-iodobenzylguanidine) scintigraphy - MIBG is taken up by chromaffin cells; whole-body scan for metastatic disease. Also used therapeutically with ¹³¹I-MIBG.
- ¹⁸F-FDG-PET - for SDHB-related and malignant disease
- ¹⁸F-DOPA PET - high sensitivity
- ¹⁸F-Fluorodopamine PET - high sensitivity for adrenal lesions
Adrenal Venous Sampling: NOT useful for pheochromocytoma (unlike primary hyperaldosteronism).
Management
Preoperative Preparation (Critical!)
Beta-blocker alone before alpha-blockade = unopposed alpha-adrenergic stimulation = hypertensive crisis and peripheral ischemia (dangerous)
Step-by-Step:
-
Alpha-blockade x 7-10 days preoperatively
- Phenoxybenzamine (drug of choice) - irreversible, non-selective alpha-blocker
- Start 10 mg once or twice daily, increase by 10-20 mg every 2-3 days
- Final dose: typically 20-100 mg/day
- Alternatives: selective alpha-1 blockers - doxazosin (start 1 mg at bedtime), prazosin, terazosin
- Target BP: <120/80 seated; systolic >90 standing
- Phenoxybenzamine (drug of choice) - irreversible, non-selective alpha-blocker
-
High-sodium diet (≥5000 mg/day) from day 2-3 of alpha-blockade - to expand catecholamine-contracted blood volume
-
Beta-blockade - add only after adequate alpha-blockade, only if HR >80 bpm
- Use propranolol or atenolol
-
Calcium channel blockers - useful adjunct; also as alternative in patients who cannot tolerate alpha-blockers
-
Volume expansion before surgery
Target parameters preoperatively:
- Seated BP <120/80 mmHg
- Standing systolic BP >90 mmHg
- HR 60-80 bpm seated, 70-80 bpm standing
- No ST changes on ECG for 1 week preop
- No more than 1 paroxysm per week
Surgical Treatment: Definitive Cure
- Open adrenalectomy for large (>6 cm), locally invasive, or suspected malignant tumors
- Partial adrenalectomy possible in familial bilateral cases to preserve adrenal cortical function
- Hypertensive episodes: IV nitroprusside, phentolamine, nitroglycerin, nicardipine (rapid onset, short half-life)
- Tachyarrhythmias: IV labetalol or esmolol
- After tumor removal: aggressive fluid resuscitation (sudden loss of vasomotor tone → hypotension)
- Monitor for hypotension - use phenylephrine + aggressive fluids
- Correct electrolyte abnormalities and hypoglycemia
- Some patients remain hypertensive postoperatively (essential or renovascular HTN)
- Persistent hypoglycemia can occur (rebound hyperinsulinism)
Malignant Pheochromocytoma
- Defined by presence of metastases, not histology
- Metastatic sites: lymph nodes, liver, lung, bone
- More common in extra-adrenal tumors (up to 20%), SDHB mutations (high risk)
- Treatment options for malignant/metastatic disease:
- ¹³¹I-MIBG therapy (if MIBG-avid tumor)
- Chemotherapy: CVD regimen (cyclophosphamide + vincristine + dacarbazine)
- Sunitinib (tyrosine kinase inhibitor) - recent evidence
- External beam radiotherapy (for bone metastases)
- Stereotactic radiosurgery for paragangliomas
Differential Diagnosis
| Condition | Differentiating Feature |
|---|---|
| Essential/secondary hypertension | No hyperadrenergic spells, normal metanephrines |
| Anxiety/panic attacks | Normal catecholamines; clonidine suppresses |
| Hyperthyroidism | TFTs abnormal |
| Carcinoid syndrome | Flushing (not pallor), elevated 5-HIAA |
| Cocaine/amphetamine use | Drug history, urine toxicology |
| Renovascular hypertension | Renal artery Doppler, elevated renin |
| Heart failure | Can be precipitated BY pheochromocytoma |
| Neuroblastoma (in children) | Elevated HVA>VMA, abdominal mass, calcification |
Follow-Up
- Lifelong annual biochemical follow-up (even after apparently complete resection)
- Biochemistry (plasma/urine metanephrines) 2-6 weeks postoperatively as baseline, then annually
- Recurrence rate: ~10% after 5 years; up to 17% at 10 years
- Genetic counseling and cascade testing of first-degree relatives
High-Yield Exam Points Summary
| Topic | Key Fact |
|---|---|
| Best biochemical test | Plasma free fractionated metanephrines |
| Drug of choice preoperatively | Phenoxybenzamine (alpha-blockade first!) |
| Never give beta-blocker first | Risk of unopposed alpha = hypertensive crisis |
| T2 MRI appearance | Hyperintense ("light bulb sign") |
| Chromaffin reaction (gross) | Dark brown with potassium dichromate |
| Malignancy criterion | Presence of metastases (not histology) |
| Most common location | Adrenal medulla (90%) |
| Organ of Zuckerkandl | Aortic bifurcation - commonest extra-adrenal site |
| Flushing | NOT typical - think carcinoid instead |
| Cardiomyopathy from pheo | Dilated or hypertrophic; REVERSIBLE after resection |
| MEN2A pheo rate | ~50%, usually bilateral |
| MEN2B gene | RET; marfanoid + neuromas |
| VHL disease chromosome | 3p25-26 |
| SDHB significance | Highest malignancy risk among hereditary pheo |
| Bladder paraganglioma | Micturition headache + painless hematuria |
| Histology zellballen | Nests of cells separated by vascular stroma |
| Preop Na diet | ≥5000 mg/day to expand blood volume |
| MIBG | Nuclear scan for metastatic disease; ¹³¹I-MIBG is therapeutic |
Recent evidence note: A 2025 meta-analysis (PMID 40214691) on partial adrenalectomy for pheochromocytoma showed favorable surgical outcomes, supporting its use in bilateral/familial cases to preserve cortical function. Core diagnostic and management principles remain consistent with Endocrine Society guidelines.
Generate infographics of same for easy revision
Medical education infographic titled "PHEOCHROMOCYTOMA - Overview & Rule of 10s" for PG medicine exam revision. Dark blue and orange color scheme. Include: - Top banner: "PHEOCHROMOCYTOMA" with subtitle "Catecholamine-secreting tumor of chromaffin cells of adrenal medulla" - Central adrenal gland diagram showing location - "RULE OF 10s" box with 7 bullet points: 10% Extra-adrenal, 10% Bilateral (50% in familial), 10% Malignant (20% extra-adrenal), 10% in Children, 10% Normotensive, 10% Recurrent, >40% Familial (modern data) - Classic Triad box: Headache + Sweating + Palpitations - Key stats: Incidence 2-8/million/year, Found in 0.2-0.6% of hypertensives - Bottom note: "Malignancy = METASTASES (not histology)" Clean, professional, easy to read, high contrast text, suitable for medical students
Medical education infographic titled "PHEOCHROMOCYTOMA - Familial Syndromes & Genetics" for PG medicine exam revision. Dark purple and gold color scheme. Include a well-organized table/cards layout with 5 syndrome cards: 1. MEN2A: Gene=RET, Pheo ~50% bilateral, + Medullary thyroid Ca + Parathyroid adenoma + Cutaneous lichen amyloidosis 2. MEN2B: Gene=RET, Pheo bilateral, + MTC + Submucosal neuromas + Marfanoid habitus + Hirschsprung 3. Von Hippel-Lindau Type 2: Gene=VHL (chr 3p25-26), Pheo ~20%, + Hemangioblastomas + Clear cell RCC + Pancreatic NETs 4. Neurofibromatosis Type 1: Gene=NF1, Pheo ~2%, + Cafe-au-lait spots + Neurofibromas + Lisch nodules 5. SDH-related (SDHB/C/D): High malignancy risk especially SDHB, paragangliomas common Bottom section: "Physical Clues" - Cafe-au-lait=NF1, Retinal hemangiomas=VHL, Marfanoid+neuromas=MEN2B Clean medical infographic, easy to memorize, bold headings, color coded cards
Medical education infographic titled "PHEOCHROMOCYTOMA - Clinical Features & Diagnosis" for PG medicine exam revision. Teal and red color scheme. Left column - "SYMPTOMS" with icons: - Classic Triad: Headache, Sweating, Palpitations (in bold box) - Hypertension: Sustained (most common) + Paroxysmal episodes in 2/3 - Pallor (NOT flushing - exam trap! flushing = carcinoid) - Tremor, Weight loss, Hyperglycemia/DM - Dilated/Hypertrophic Cardiomyopathy (REVERSIBLE after resection!) - Bladder paraganglioma: micturition headache + painless hematuria - Orthostatic hypotension Right column - "WHEN TO SUSPECT": - Resistant hypertension - Hyperadrenergic spells - Familial syndrome (MEN2/NF1/VHL) - Hypertension before age 20 - HTN + Diabetes - Pressor response during anesthesia/surgery - Idiopathic dilated cardiomyopathy - Adrenal incidentaloma Bottom - Red alert box: "EXAM TRAP: Flushing is NOT typical of Pheo! Flushing = Carcinoid/Mastocytosis" Professional medical infographic style, clear hierarchy
Medical education infographic titled "PHEOCHROMOCYTOMA - Biochemical Diagnosis & Imaging" for PG medicine exam revision. Navy blue and yellow color scheme. Top section - "BIOCHEMICAL TESTS" comparison table: - BEST TEST (highlighted in gold): Plasma Free Fractionated Metanephrines - Sensitivity ~99% - "WHY? Metanephrines continuously elevated even between spells" - 24h Urine Fractionated Metanephrines - Sensitivity >97%, Specificity ~91% - 24h Urine VMA - Sensitivity ~80% - older test - Clonidine Suppression Test: Suppresses neurogenic causes but NOT pheo Middle section - "IMAGING" CT scan findings: HU >10 on non-contrast (adenoma <10 HU), vigorous enhancement, <60% washout MRI: T2 HYPERINTENSE = "Light Bulb Sign" - choice in pregnancy/children MIBG scan: for metastatic disease, 131I-MIBG also therapeutic Rule: Biochemical diagnosis FIRST, then imaging Bottom section - "FALSE POSITIVES": Tricyclics, MAOIs, levodopa, methyldopa, cocaine, amphetamines, phenoxybenzamine Color coded, bold key numbers, exam-ready layout for medical students
Medical education infographic titled "PHEOCHROMOCYTOMA - Management & Treatment Algorithm" for PG medicine exam revision. Green and dark red color scheme with clear flowchart. LARGE RED WARNING BOX at top: "NEVER give Beta-blocker FIRST! → Unopposed Alpha stimulation → Hypertensive crisis + Peripheral ischemia" Pre-operative preparation flowchart (numbered steps): STEP 1: ALPHA BLOCKADE FIRST (7-10 days preop) - Phenoxybenzamine (DRUG OF CHOICE) - irreversible non-selective alpha blocker - Start 10mg OD/BD → increase by 10-20mg every 2-3 days - Final dose 20-100mg/day - Target BP: <120/80 seated; systolic >90 standing - Alternative: Doxazosin, Prazosin STEP 2: HIGH SODIUM DIET (≥5000mg/day from day 2-3) → expand blood volume STEP 3: BETA BLOCKER (only if HR >80 after adequate alpha blockade) → Propranolol/Atenolol SURGERY: Laparoscopic adrenalectomy (standard) / Open for large or malignant INTRA-OP: Nitroprusside, Phentolamine, Nicardipine for HTN crises POST-OP: Fluids + Vasopressors for hypotension; monitor glucose Bottom: Malignant Pheo treatment: 131I-MIBG therapy, CVD chemotherapy, Sunitinib Professional medical infographic, clear decision flow, bold warnings
429 Too Many Requests. {'message': '{\n "error": {\n "code": 429,\n "message": "Resource exhausted. Please try again later. Please refer to https://cloud.google.com/vertex-ai/generative-ai/docs/error-code-429 for more details.",\n "status": "RESOURCE_EXHAUSTED"\n }\n}\n', 'status': 'Too Many Requests'}
We encountered an error while processing your request. Please try again or reach out to us for help.