Approach to acute dysphagia in a 60year old female, with complaint of vomiting on taking food
Reading File
search_medical_text
acute dysphagia causes differential diagnosis elderly female
search_medical_text
dysphagia evaluation history examination investigations endoscopy
search_medical_image
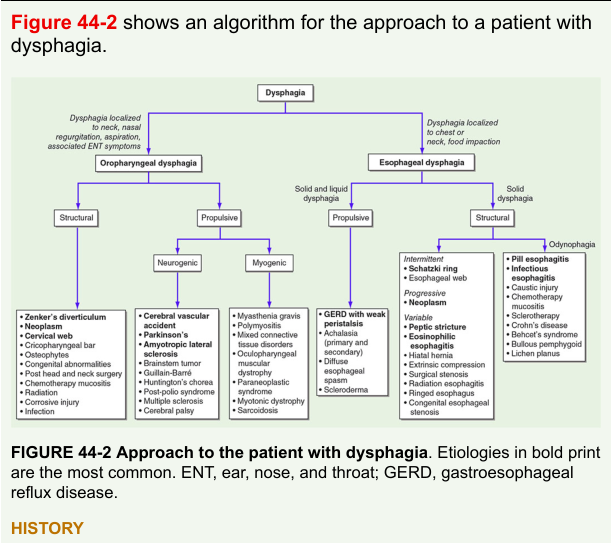
dysphagia approach algorithm flowchart
GradeResponse
GradeResponse
GradeResponse
search_medical_text
esophageal dysphagia oropharyngeal dysphagia clinical features differentiation regurgitation
Good — I have strong retrieval from Harrison's. Here is a comprehensive, structured clinical approach.
Acute Dysphagia in a 60-Year-Old Female with Regurgitation of Food
Diagnostic Algorithm
Step 1 — Localize the Dysphagia
The first and most critical step is to determine whether dysphagia is oropharyngeal or esophageal, as the workup and management differ entirely.
| Feature | Oropharyngeal | Esophageal |
|---|---|---|
| Site of complaint | Throat, neck, "can't initiate swallow" | Chest, "food sticks in chest/mid-sternum" |
| Timing | Immediately on swallowing (<1 sec) | 2–5 seconds after swallowing |
| Regurgitation | Undigested food, nasal, immediate | Hours later, digested or undigested |
| Cough/aspiration | Common (nasal regurgitation, choking) | Less common |
| Neurological signs | Often present (CVA, Parkinson's) | Absent |
| Voice change/hoarseness | May be present | Absent |
In this patient: "Vomiting on taking food" most likely represents regurgitation (not true vomiting, which implies gastric content). Immediate regurgitation of undigested food points to oropharyngeal or proximal esophageal cause; delayed regurgitation suggests esophageal dysmotility or obstruction.
Step 2 — Detailed History
Character of Dysphagia
- Solids only → Mechanical obstruction (stricture, ring, neoplasm)
- Solids + liquids from onset → Motility disorder (achalasia, diffuse esophageal spasm)
- Solids then progressing to liquids → Progressive mechanical obstruction (malignancy)
- Intermittent vs. progressive → Intermittent + solid = Schatzki ring; Progressive = malignancy, stricture
Associated Symptoms
- Weight loss + progressive solid dysphagia → Esophageal/gastric carcinoma (red flag)
- Heartburn, acid reflux → Peptic stricture, eosinophilic esophagitis
- Halitosis + gurgling noise + food regurgitated hours later → Zenker's diverticulum (classic in elderly)
- Chest pain → Diffuse esophageal spasm, achalasia
- Odynophagia (painful swallowing) → Infectious esophagitis (candida, HSV), pill esophagitis, malignancy
- Nasal regurgitation, choking, aspiration pneumonia → Oropharyngeal cause
- Neurological symptoms (diplopia, dysarthria) → Bulbar palsy, myasthenia gravis
Relevant History
- Medication history — bisphosphonates, NSAIDs, tetracycline (pill-induced esophagitis)
- History of GERD, Barrett's esophagus
- Prior head/neck surgery, radiation, chemotherapy
- Autoimmune disease (scleroderma → esophageal dysmotility; Sjögren's)
- Smoking, alcohol use (squamous cell carcinoma risk)
Step 3 — Differential Diagnosis
Oropharyngeal Causes (Structural)
(Harrison's, p. 1204)
| Condition | Key Feature |
|---|---|
| Zenker's Diverticulum | Elderly patient, regurgitation of undigested food, halitosis, gurgling; due to cricopharyngeal dysfunction (Killian's dehiscence) |
| Cricopharyngeal bar | Common, often asymptomatic; related to Zenker's |
| Head/neck neoplasm | Progressive, weight loss, hoarseness |
| Cervical osteophytes | Elderly, bony compression |
| Cervical web (Plummer-Vinson) | Iron-deficiency anemia + dysphagia in females |
| Post-radiation/corrosive injury | History |
Oropharyngeal Causes (Propulsive/Neurogenic)
| Condition | Key Feature |
|---|---|
| Stroke (CVA) | Sudden onset, focal neurological signs |
| Parkinson's disease | Tremor, rigidity, bradykinesia |
| Bulbar/pseudobulbar palsy | UMN/LMN signs |
| Myasthenia gravis | Fatigable weakness, ptosis, diplopia |
| ALS | Wasting, fasciculations |
Esophageal Causes (Structural)
| Condition | Key Feature |
|---|---|
| Carcinoma of esophagus | Progressive solid → liquid, weight loss; squamous or adenocarcinoma |
| Peptic stricture | Long-standing GERD, solid food dysphagia |
| Schatzki ring | Intermittent solid food dysphagia |
| Eosinophilic esophagitis | Young adult, atopy, food impaction |
| Foreign body | Sudden, history |
| Extrinsic compression | Lymphoma, lung cancer, vascular (dysphagia lusoria) |
Esophageal Causes (Motility)
| Condition | Key Feature |
|---|---|
| Achalasia | Solids + liquids, regurgitation, chest pain, weight loss; "bird-beak" on barium |
| Diffuse esophageal spasm | Intermittent, chest pain, corkscrew esophagus |
| Scleroderma | Raynaud's, skin changes, GERD |
Step 4 — Physical Examination
- General: Nutritional status, weight loss, pallor (iron deficiency)
- Head & Neck: Lymphadenopathy, thyroid enlargement, neck mass, oral cavity inspection
- Neurological: Cranial nerves (V, VII, IX, X, XII), gag reflex, speech, tongue fasciculations, tremor
- Skin: Telangiectasias, sclerodactyly (scleroderma), Raynaud's
- Abdominal: Epigastric mass, hepatomegaly (metastasis)
- Listen: Gurgling sound in neck on swallowing → Zenker's diverticulum
Step 5 — Investigations
First-Line
(Harrison's, p. 1209)
| Investigation | Indication |
|---|---|
| Upper GI Endoscopy (OGD) | Most useful single test for esophageal dysphagia; visualizes mucosa, allows biopsy |
| Barium swallow (fluoroscopy) | Oropharyngeal dysphagia (fluoroscopic swallow study with speech therapist); Zenker's diverticulum; motility |
| Video fluoroscopic swallow study | Oropharyngeal dysphagia — procedure of choice |
| Blood tests | CBC (anemia), ESR/CRP, LFTs, TFTs, blood glucose |
| Chest X-ray | Mediastinal widening, air-fluid level (achalasia), aspiration pneumonia |
Second-Line (Based on Findings)
| Investigation | Indication |
|---|---|
| CT chest/abdomen/pelvis | Staging if malignancy suspected |
| Esophageal manometry | Motility disorders (achalasia, DES, scleroderma) |
| Ambulatory pH monitoring | GERD-related stricture |
| ENT/Laryngoscopy | Oropharyngeal structural pathology |
| MRI brain/brainstem | Neurological cause (CVA, tumor) |
| AChR antibodies | Myasthenia gravis |
Step 6 — Red Flag Features (Urgent Referral)
Warrant urgent (2-week wait) endoscopy:
- Progressive dysphagia
- Significant weight loss (>5% in 3 months)
- Age >55 with new dysphagia
- Odynophagia
- Hematemesis or melena
- Iron-deficiency anemia
- Persistent vomiting
This 60-year-old female with acute dysphagia and food regurgitation has multiple red flag features and requires urgent upper GI endoscopy.
Summary Algorithm
Dysphagia + Regurgitation of food
│
▼
Is it oropharyngeal or esophageal?
│
┌──────┴──────┐
│ │
Oro- Esophageal
pharyngeal │
│ ├─ Structural → OGD (malignancy, stricture, ring)
├─ Structural ├─ Motility → Manometry (achalasia, DES)
│ → Barium └─ Extrinsic → CT chest
│ swallow
│ (Zenker's,
│ web, tumor)
│
└─ Propulsive
→ Neurology
workup
(MRI, EMG)
Key Point for This Patient
Given 60-year-old female + acute dysphagia + food regurgitation, the top priorities are:
- Rule out esophageal/gastric malignancy — urgent OGD with biopsy
- Zenker's diverticulum — especially if regurgitation is of undigested food, with halitosis or gurgling (Harrison's, p. 1204)
- Achalasia — if both solids and liquids affected
- Peptic stricture — if prior GERD history
- Neurological cause — if oropharyngeal features dominate
Sources: Harrison's Principles of Internal Medicine, 21st Edition, pp. 1204, 1206, 1209
For the same patient gag reflex is present while she complaints that whenever food touches hard palate she’s puking and there’s a 5mm black coloured raised lesion present on hard palate laterally
search_medical_text
black pigmented lesion hard palate oral cavity melanoma melanotic macule
search_medical_image
black lesion hard palate oral melanoma pigmented
GradeResponse
GradeResponse
This is a critical finding. The new information significantly redirects the diagnosis. Here is the updated clinical approach:
Updated Approach — New Critical Finding
Clinical Reassessment
The new information changes the entire diagnostic picture:
| Finding | Interpretation |
|---|---|
| Gag reflex present | Central/peripheral neurological cause excluded; brainstem and CN IX/X intact |
| Food touching hard palate → immediate vomiting | Hypersensitive/exaggerated palatal reflex — local lesion triggering reflex arc |
| 5mm black, raised lesion on lateral hard palate | High suspicion for Oral Mucosal Malignant Melanoma (OMMM) or other pigmented oral pathology |
The dysphagia and regurgitation in this patient are NOT esophageal or neurological in origin. The lesion on the hard palate is mechanically and reflexively triggering vomiting each time food contacts it.
The Lesion — Differential Diagnosis
A 5mm black, raised (exophytic) lesion on the lateral hard palate in a 60-year-old female narrows the differential significantly:
Priority 1 — Oral Mucosal Malignant Melanoma (OMMM) ⚠️

- The hard palate and maxillary alveolus are the most common sites of OMMM
- Typically presents as a black/brown pigmented, raised, irregular lesion
- Can be preceded by a flat melanotic patch (radial growth phase) before becoming nodular/exophytic (vertical growth phase)
- Satellite macules may be present around the main lesion
- Rare but highly aggressive — 5-year survival <20%
- Often asymptomatic until late, which is why dysphagia/regurgitation here is a key presenting complaint
Differential Diagnosis of Black Raised Lesion on Hard Palate
| Diagnosis | Features | Likelihood |
|---|---|---|
| Oral Malignant Melanoma | Black/brown, raised, irregular border, hard palate, elderly | High — must exclude first |
| Amalgam tattoo | Blue-grey, flat, near dental restorations, no raised component | Less likely (raised lesion) |
| Melanotic macule (oral focal melanosis) | Flat, well-defined, benign, no raised component | Less likely (raised) |
| Melanocytic nevus | Brown-black, raised, well-circumscribed; rare on palate | Possible |
| Kaposi's sarcoma | Violaceous/black plaque, hard palate; associated with HIV/immunosuppression | Consider if immunocompromised |
| Black hairy tongue / fungal deposit | Dorsal tongue; not palatal | Unlikely |
| Thrombosed hemangioma / vascular lesion | Bluish-black, blanches on pressure (diascopy) | Possible |
| Pigmented squamous cell carcinoma | Rare, usually ulcerated, indurated | Less common |
| Metastatic deposit | Hard palate metastases from renal, lung, breast cancer | Consider in elderly |
Immediate Clinical Steps
1. Examine the Lesion Carefully
Apply the ABCDE criteria (adapted for oral lesions):
| Criterion | Assessment |
|---|---|
| A — Asymmetry | Irregular shape? |
| B — Border | Irregular, ill-defined borders? |
| C — Color | Variegated black, brown, grey? Multiple shades? |
| D — Diameter | >6mm is concerning; this is 5mm but raised |
| E — Evolution | Any rapid growth? Change in size/color? |
- Perform diascopy (press glass slide on lesion): vascular lesions blanch, melanoma/melanotic lesions do not
2. Assess the Palate and Oral Cavity Fully
- Look for satellite macules around the main lesion (suggests OMMM spread)
- Inspect entire oral mucosa, gingiva, buccal mucosa
- Palpate for cervical lymphadenopathy (submandibular, jugulodigastric nodes) — indicates regional metastasis
3. Assess Gag Reflex Hypersensitivity
- The lesion, by occupying real estate on the hard palate, may be directly stimulating mechanoreceptors causing an exaggerated palatal reflex
- This is a functional consequence of the lesion, not a primary neurological problem
Investigations
Urgent
| Investigation | Purpose |
|---|---|
| Incisional biopsy (preferred over excisional for suspected melanoma) | Histopathology — definitive diagnosis; assess depth (Breslow thickness), Clark level, mitotic index |
| Immunohistochemistry | S-100, HMB-45, MelanA/MART-1, SOX10 — confirm melanocytic origin |
| OPG / Dental X-ray | Bone invasion from underlying lesion |
Staging (if melanoma confirmed)
| Investigation | Purpose |
|---|---|
| CT Head, Neck, Chest, Abdomen, Pelvis | Regional and distant metastases |
| MRI head and neck | Local extent, bone invasion, perineural spread |
| PET-CT | Gold standard for staging OMMM |
| Sentinel lymph node biopsy | Regional nodal status (controversial in OMMM) |
Baseline
- Full blood count, LFTs, LDH (elevated in melanoma = poor prognosis), S-creatinine
- HIV serology (if Kaposi's suspected)
Management Outline (Pending Histology)
If OMMM Confirmed:
- Surgery — Wide local excision with clear margins (1–2 cm); may require partial maxillectomy if bone involved
- Reconstruction — Palatal prosthesis or flap repair
- Neck dissection — If lymph nodes positive
- Adjuvant therapy — Radiotherapy (radiosensitive) ± immunotherapy (anti-PD1: pembrolizumab/nivolumab) or targeted therapy (BRAF/MEK inhibitors if BRAF V600E mutated)
- Multidisciplinary team — Oral maxillofacial surgery, ENT, oncology, prosthodontics
Immediate Symptomatic Relief:
- Soft/liquid diet to avoid contact with lesion and prevent vomiting
- Nutritional support if oral intake compromised
- Topical analgesia if odynophagia develops
Summary
In this 60-year-old female, the dysphagia and food-contact vomiting are directly attributable to a 5mm raised black lesion on the lateral hard palate triggering an exaggerated palatal reflex. The intact gag reflex excludes neurological disease. The lesion's morphology — black, raised, hard palate location in an elderly female — is highly suspicious for Oral Mucosal Malignant Melanoma until proven otherwise, and warrants urgent incisional biopsy and staging workup.
Sources: Bailey & Love's Short Practice of Surgery, 28th Edition, p. 834; Harrison's Principles of Internal Medicine, 21st Edition, pp. 1204–1209
This is a shared conversation. Sign in to Orris to start your own chat.