Anesthetic consideration in siabetic mellitus
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive, authoritative content from Barash's Clinical Anesthesia and Sabiston's Surgery. Let me compile the full answer.
Anesthetic Considerations in Diabetes Mellitus
Diabetes mellitus (DM) is the most common endocrinopathy encountered perioperatively. In the US alone, the incidence is ~11% overall and exceeds 20% in those over 65 years. Diabetic patients are more likely to require surgery due to their disease complications, and the majority have secondary involvement of one or more organ systems that must be assessed before anesthesia.
1. Preoperative Assessment
Cardiovascular
- Diabetics have a significantly elevated risk of coronary artery disease (CAD), hypertension, congestive heart failure, and perioperative myocardial infarction.
- Silent ischemia is more common because autonomic neuropathy blunts anginal symptoms - this is a critical point for anesthetic risk stratification.
- The 2014 ACC/AHA guideline classifies insulin-dependent diabetics at elevated cardiac risk. ECG is mandatory preoperatively.
- β-blockers should be considered if the patient has ≥2 risk factors for adverse cardiac events; they do not worsen glucose intolerance or mask hypoglycemic symptoms.
Renal
- DM is the leading cause of renal failure requiring dialysis.
- Check serum creatinine and electrolytes; renal impairment alters drug dosing and fluid management.
Neurologic
- Autonomic neuropathy may cause hemodynamic instability under anesthesia (exaggerated hypotension with induction) and gastroparesis, which significantly increases aspiration risk.
- Peripheral neuropathy and vascular disease increase susceptibility to positioning injuries - document pre-existing deficits before anesthesia begins.
- Cerebrovascular and peripheral vascular disease are more prevalent.
Airway
- Stiff joint syndrome - due to glycosylation of proteins and abnormal collagen cross-linking - can affect the temporomandibular, atlanto-occipital, and cervical spine joints in longstanding Type 1 diabetics, leading to difficult tracheal intubation.
- A thorough airway examination is mandatory. The "prayer sign" (inability to fully oppose palms with fingers extended) suggests stiff joint involvement at other joints, including those relevant to airway manipulation. Maintain a high index of suspicion for difficult airway.
Laboratory Work-up
- Blood glucose, HbA1c, serum electrolytes, creatinine, urinalysis (ketonuria), and ECG.
- Target HbA1c: <8% for Type 1 and <7% for Type 2 (American Diabetes Association). If above target, elective surgery should be delayed for optimization.
2. Preoperative Optimization
- Schedule the diabetic patient as the first case of the day to minimize fasting duration and glucose variability.
- Have the patient arrive early and check blood glucose on arrival, then hourly if there is a delay.
- If blood glucose is <70 mg/dL on arrival, administer a glucose tablet or clear juice (or IV dextrose if IV is in place).
3. Medication Management on the Day of Surgery
Oral Antidiabetics
- Hold all oral antidiabetic agents on the day of surgery to avoid reactive hypoglycemia.
- Metformin must be stopped due to the risk of perioperative lactic acidosis (especially with renal hypoperfusion or contrast use).
- Non-insulin injectables (GLP-1 agonists, etc.) are also held.
Insulin
| Insulin Type | Day-of-Surgery Management |
|---|---|
| Rapid/short-acting | Hold on morning of surgery (unless hyperglycemia requires correction) |
| Intermediate/long-acting | Give a reduced dose (typically 50-80% of usual basal dose) |
| Insulin pumps | Continue at sleep (basal) rates for short procedures; convert to IV insulin infusion for major/prolonged surgery |
- Type 1 diabetics must continue basal insulin even while NPO to prevent diabetic ketoacidosis (DKA).
- Once insulin is given to an NPO patient, glucose must be provided in IV fluids or blood glucose closely monitored.
4. Perioperative Glucose Targets
Surgical stress triggers release of cortisol and catecholamines, driving perioperative hyperglycemia. Elevated glucose impairs neutrophil function, promotes reactive oxygen species and inflammatory mediators, and causes direct vascular and immune dysfunction.
Target blood glucose recommendations by society:
| Society | Target (mg/dL) |
|---|---|
| Society for Ambulatory Anesthesia (SAMBA) | <180 |
| American Diabetes Association | 140-180 |
| Society of Critical Care Medicine | <150 |
| American College of Physicians | 140-200 |
General consensus: maintain blood glucose <180-200 mg/dL intraoperatively. Hypoglycemia must be equally avoided - it is harder to detect under anesthesia and carries its own morbidity.
5. Intraoperative Management
- Check blood glucose every 1-2 hours intraoperatively (or more frequently if on IV insulin infusion).
- For short/minor procedures in well-controlled diabetics: subcutaneous sliding-scale insulin + 1-2 hourly glucose checks may suffice.
- For major/prolonged surgery: intravenous insulin infusion (regular insulin) is preferred over subcutaneous or pump insulin.
- Administer insulin infusion via a side port into the same IV line as the glucose infusion (for safety).
- Use a separate non-glucose isotonic solution for replacing fluid deficits and intraoperative losses.
- Concurrent separate infusions of insulin and glucose allow easier adjustment and better control than combined glucose/insulin/potassium (GIK) infusions.
- For cardiac surgery patients and the critically ill, tight glycemic control has the most evidence for reducing morbidity and mortality.
Choice of Anesthetic Agents
- No single anesthetic technique has been proven superior in diabetics.
- Autonomic neuropathy increases sensitivity to vasodilatory and myocardial depressant effects of volatile agents and IV induction agents - anticipate and prepare for hemodynamic instability.
- Regional anesthesia may be preferred where appropriate, as it blunts the stress response and avoids issues of gastroparesis/aspiration with general anesthesia. However, peripheral neuropathy must be documented beforehand.
- Gastroparesis mandates aspiration precautions for general anesthesia: RSI (rapid sequence induction), H2 blocker/proton pump inhibitor, and prokinetic agents preoperatively.
6. Postoperative Care
- Prevent and treat postoperative nausea and vomiting (PONV) aggressively - particularly important because vomiting disrupts oral intake and insulin resumption.
- Encourage early resumption of diet to allow return to the patient's home insulin regimen.
- Check blood glucose before discharge.
- Perioperative insulin requirements vary by: body weight, liver disease, steroid use, infection, and whether cardiopulmonary bypass is used.
7. Special Considerations
Diabetic Ketoacidosis (DKA) Risk
- Type 1 diabetics: must never be left without basal insulin, even while NPO. Omitting basal insulin in a stressed surgical patient is a common trigger for DKA.
Hyperosmolar Hyperglycemic State (HHS) Risk
- Type 2 diabetics under severe physiologic stress (sepsis, major surgery) are more prone to non-ketotic HHS - severe dehydration, hyperglycemia, and hyperosmolarity.
Pediatric Patients
- The Society for Pediatric Anesthesia recommends similar perioperative principles, though no consensus HbA1c threshold exists for pediatric patients.
Positioning
- Peripheral neuropathy and vascular disease increase the risk of pressure injuries and nerve damage from positioning - use extra padding and document baseline neurological status.
Sources:
- Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e - Chapters 23 and 15 (Diabetes Mellitus, Perioperative Glucose Management)
- Sabiston Textbook of Surgery, 11e - Chapter 20 (Endocrinology, Metabolism, and Nutrition: Diabetes Mellitus)
Find research on autonomic neuropathy complications in diabetic patients under anesthesia
Finding Sources
Searching PubMed
diabetic autonomic neuropathy anesthesia perioperative complications
Finding Sources
Searching PubMed
diabetic autonomic neuropathy cardiovascular perioperative
Searching PubMed
cardiac autonomic neuropathy diabetes surgery hemodynamic
Reading Article
PMID: 30166651
Reading Article
PMID: 30788010
Reading File
Reading File
Reading File
Searching PubMed
diabetic autonomic neuropathy gastroparesis aspiration anesthesia
Searching PubMed
cardiac autonomic neuropathy intraoperative hypotension sudden death
Reading Article
PMID: 29559406
Reading Article
PMID: 39834981
Finding Sources
Finding Sources
Finding Sources
I have rich data from multiple authoritative sources. Let me now compile the comprehensive research summary.
Diabetic Autonomic Neuropathy (DAN): Complications Under Anesthesia
Overview
Diabetic autonomic neuropathy (DAN) affects the cardiovascular, gastrointestinal, genitourinary, thermoregulatory, and respiratory systems. An estimated 25% of diabetic patients will require surgery, and mortality in diabetic surgical patients is measurably higher than in non-diabetics - with DAN being a major driver of that risk. Moningi et al., Indian J Anaesth, 2018 (PMID 30166651) - a dedicated review on this topic - concludes that "diabetic autonomic neuropathy and its implications may sometimes be disastrous and further increase the incidence of in-hospital morbidity and mortality."
1. Cardiovascular Autonomic Neuropathy (CAN)
Epidemiology
CAN is severely debilitating yet underdiagnosed. Prevalence ranges from 2.5% (in primary prevention Type 1 diabetes cohorts, Diabetes Control and Complications Trial) to as high as 90% of Type 1 diabetics in some studies. - Agashe & Petak, Methodist DeBakey Cardiovasc J, 2018 (PMID 30788010)
Intraoperative Hypotension at Induction
- Autonomic reflex dysfunction in surgical patients is directly associated with hypotension after anesthesia induction. (Latson et al., Anesthesiology. 1994;80(2):326-337 - cited in Barash Clinical Anesthesia, 9e)
- Patients with CAN have impaired baroreceptor reflex and sympathetic vasomotor tone, leaving them unable to compensate for the vasodilation from induction agents.
- Vohra et al. (Br J Anaesth. 1993;71(2):258-261) demonstrated that diabetes mellitus specifically affects cardiovascular responses to induction of anaesthesia and tracheal intubation - blunted tachycardia and impaired pressor response.
- Miller's Anesthesia (10e) notes: autonomic neuropathy causes attenuated hyperadrenergic signs during hypoglycemia under anesthesia, making it difficult to detect low blood glucose on clinical grounds alone.
Silent Myocardial Ischemia
- Silent ischemia is present in 30-50% of Type 2 diabetics - a direct consequence of CAN blunting pain sensation. (Cheisson et al., Anaesth Crit Care Pain Med, 2018 - PMID 29559406, Practice Guideline)
- Patients may sustain perioperative myocardial infarction without classic chest pain, making ECG and troponin monitoring more important in this population.
Sudden Cardiac Death
- Page & Watkins (Lancet. 1978;1:14-16) - a landmark early paper - documented cardiorespiratory arrest as a complication of diabetic autonomic neuropathy under anesthesia. This risk arises from:
- Impaired cardiorespiratory reflexes
- Prolonged QT interval (a recognized feature of CAN)
- Increased susceptibility to arrhythmias
Clinical Implications
- Cheisson et al. (Practice Guideline, 2018) recommend that CAN must be investigated preoperatively because it causes an increased risk of cardiovascular events and sudden death, even when clinically asymptomatic.
- Signs suggestive of CAN mandate close perioperative cardiovascular surveillance.
- Regional/neuraxial anesthesia can worsen hypotension in patients with autonomic insufficiency due to additional sympathetic blockade - Miller's Anesthesia 10e states: "Regional and neuraxial techniques have the advantage of reducing sympathetic stimulation but can become problematic in patients with autonomic insufficiency where hypotension may be exacerbated."
2. Gastroparesis and Aspiration Risk
Mechanism
- DAN directly impairs gastric motility through vagal dysfunction, producing diabetic gastroparesis.
- Barash Clinical Anesthesia (9e) is explicit: "The extent of delayed gastric emptying with diabetes mellitus correlates well with the presence of autonomic neuropathy but not with age, duration of disease, HbA1c, or peripheral neuropathy."
- The difference in gastric emptying times between healthy patients and those with Type 1 diabetes ranges from 30 minutes to 2 hours.
Evidence of Elevated Gastric Volume
A prospective comparative cohort study using point-of-care gastric ultrasonography in 220 patients found:
- Grade 2 antrum (solids/fluid in both supine and lateral positions): 18% of diabetic patients vs. 3% in non-diabetics
- Mean gastric volume was significantly higher in diabetics (34.52 mL vs controls)
- 37.2% of diabetic patients had a high-risk antrum meeting criteria for aspiration precautions
- Risk increased with female gender and older age
- [Velayudhan et al., Cureus, 2024 (PMID 39834981)]
Anesthetic Management
- Cheisson et al. (2018 Practice Guideline, PMID 29559406) recommend rapid sequence induction (RSI) for diabetic patients with gastroparesis undergoing general anesthesia.
- Barash places DM (with peripheral neuropathy) on its "At-Risk for Aspiration" list alongside full stomach, bowel obstruction, and peritonitis.
- Pre-induction pharmacologic measures: H2 blockers (famotidine), PPIs, sodium citrate ± metoclopramide.
- GLP-1 receptor agonists (now widely used in Type 2 diabetes) cause further slowing of gastric emptying - Miller's Anesthesia notes patients held off long-acting GLP-1 agonists for >7 days and fasted for >8 hours may still have residual gastric contents. The ASA recommends stopping injectable GLP-1 agonists for at least 1 week before elective surgery.
3. Blunted Hypoglycemia Detection
- Under general anesthesia, all the adrenergic symptoms of hypoglycemia (tachycardia, diaphoresis, tremor) are absent or attributed to other causes.
- Patients with CAN or on beta-blockers have additionally attenuated hyperadrenergic signs, meaning:
- Hypoglycemia can reach dangerously low levels before being detected
- Clinical diagnosis under anesthesia is essentially impossible
- Miller's Anesthesia mandates: "close monitoring of glucose concentrations intraoperatively (every 1-2 hours in patients receiving insulin perioperatively) either by frequent fingersticks or a continuous glucose monitor."
4. Thermoregulatory Dysfunction
- Kitamura et al. (Anesthesiology. 2000;92(5):1311-1318) demonstrated that patients with diabetic neuropathy are at risk of a greater intraoperative reduction in core temperature due to impaired thermoregulatory responses.
- DAN disrupts sympathetic control of peripheral vasomotion and sweating, reducing the ability to maintain normothermia under anesthesia.
- Perioperative hypothermia independently increases cardiac complications, bleeding risk, and wound infection.
5. Urologic and Genitourinary Autonomic Dysfunction
- DAN causes neurogenic bladder (detrusor hypotonicity/atonicity), which can result in urinary retention postoperatively, especially with neuraxial anesthesia - worsening a pre-existing dysfunctional bladder.
Summary of Key Anesthetic Risks and Management
| Complication | Mechanism | Management |
|---|---|---|
| Induction hypotension | Impaired baroreceptor/sympathetic tone | Reduce induction dose; pre-load; vasopressors on hand |
| Silent MI / cardiac arrest | CAN + blunted angina | Continuous ECG; troponin monitoring; avoid tachycardia |
| Pulmonary aspiration | Gastroparesis from vagal DAN | RSI; H2 blocker/PPI; sodium citrate; NG if needed |
| Undetected hypoglycemia | CAN blunts adrenergic response | 1-2 hourly glucose monitoring; continuous glucose monitor |
| Intraoperative hypothermia | Impaired vasomotor/sweating | Active warming; forced-air blankets |
| Exaggerated neuraxial hypotension | Additive sympathetic blockade | Use cautiously; titrate slowly; vasopressors ready |
| Positioning injury | Peripheral neuropathy + vascular disease | Document pre-op deficits; extra padding |
Key References
-
Moningi S, Nikhar S, Ramachandran G. Autonomic disturbances in diabetes: Assessment and anaesthetic implications. Indian J Anaesth. 2018 Aug. PMID 30166651 - Dedicated review of DAN and all its anaesthetic implications.
-
Cheisson G et al. Perioperative management of adult diabetic patients. Preoperative period. Anaesth Crit Care Pain Med. 2018. PMID 29559406 - Practice Guideline; covers CAN screening and RSI for gastroparesis.
-
Agashe S, Petak S. Cardiac Autonomic Neuropathy in Diabetes Mellitus. Methodist DeBakey Cardiovasc J. 2018. PMID 30788010 - Prevalence 2.5-90%, clinical manifestations from orthostasis to sudden death.
-
Velayudhan S et al. Preoperative Ultrasonographic Assessment of the Gastric Antrum in Diabetic Patients. Cureus. 2024. PMID 39834981 - 37.2% of diabetic patients had high-risk antrum on ultrasound.
Textbook citations:
- Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e - Chapter 23 (Diabetes Mellitus, perioperative glucose management, aspiration risk)
- Miller's Anesthesia, 10e - Intraoperative diabetes management, autonomic neuropathy and hypoglycemia masking, GLP-1 agonist considerations
- Sabiston Textbook of Surgery, 11e - Chapter 20 (Endocrinology, Metabolism)
Eclampsia in details
Reading File
Finding Sources
Finding Sources
Searching PubMed
eclampsia management magnesium sulfate
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading Article
PMID: 37815037
Reading Article
PMID: 34187284
Loading Image
Loading Image
Finding Sources
Excellent - I have outstanding content including the pathology images. Now I have all the material needed to write a comprehensive, detailed answer on eclampsia.
Eclampsia - Detailed Overview
1. Definition
Eclampsia is the development of new-onset generalized tonic-clonic seizures (or coma/encephalopathy) superimposed on pre-existing preeclampsia, occurring in a pregnant or recently delivered woman between 20 weeks of gestation and 4 weeks postpartum. It represents the most severe neurological complication of the hypertensive disorders of pregnancy.
Eclampsia can occasionally present with seizures in the absence of hypertension or proteinuria - making vigilance necessary in any pregnant/postpartum woman with unexplained seizures.
2. Epidemiology
- Hypertensive disorders of pregnancy (including eclampsia) affect approximately 85 per 1,000 deliveries in the United States.
- Seizures complicate approximately 2% of preeclampsia cases in the US.
- Up to one-third of eclampsia occurs postpartum, sometimes days to weeks after delivery - making it a common emergency medicine presentation.
- Internationally, eclampsia remains a leading cause of maternal mortality, especially in low- and middle-income countries.
- 30-50% of eclamptic women have no evidence of severe hypertension preceding their seizure.
3. Risk Factors
| Risk Factor | Relative Risk (vs. reference) |
|---|---|
| Antiphospholipid antibodies | 9.72 (95% CI 4.34-21.75) |
| Previous preeclampsia | 7.19 (5.85-8.83) |
| Preexisting diabetes mellitus | 3.56 (2.54-4.99) |
| Twin pregnancy | 2.93 (2.04-4.21) |
| Nulliparity | 2.91 (1.28-6.61) |
| Maternal age ≥40 (multiparous) | 1.96 (1.34-2.87) |
| Obesity | ~3x increased risk |
| Chronic hypertension | 25% develop superimposed preeclampsia |
| Hydatidiform mole | 70% develop preeclampsia |
| Systemic lupus erythematosus | Elevated, especially with nephropathy |
Data from Duckitt & Harrington, BMJ 2005; Creasy & Resnik's Maternal-Fetal Medicine, 9e
4. Pathophysiology
4a. Placental Origin - The Core Mechanism
The fundamental defect in preeclampsia/eclampsia is inadequate trophoblast invasion and remodeling of spiral arteries:
- In normal pregnancy, trophoblasts invade the muscular walls of spiral arteries, converting them into wide, low-resistance sinusoids that can accommodate increased blood flow.
- In preeclampsia/eclampsia, this remodeling is impaired - the musculoelastic walls are retained, vessels remain narrow (~40% the normal diameter), and uteroplacental perfusion is chronically reduced.
4b. Angiogenic/Antiangiogenic Imbalance
Placental hypoxia and dysfunction trigger the release of:
- Soluble FMS-like tyrosine kinase-1 (sFlt-1) - antiangiogenic, antagonizes VEGF
- Soluble endoglin - antiangiogenic, antagonizes TGF-β
These circulating factors cause widespread maternal endothelial dysfunction, which is the central mechanism of multi-organ injury.
4c. Consequences of Endothelial Dysfunction
| Mechanism | Clinical Effect |
|---|---|
| ↓ Prostacyclin (PGI2) + ↑ Thromboxane A2 | Vasoconstriction → Hypertension |
| ↓ Antithrombotic factors (PGI2) | Hypercoagulability |
| ↑ Procoagulant factors | DIC, thrombocytopenia |
| Endothelial damage, microangiopathy | End-organ failure (kidney, liver, brain) |
| Placental hypoperfusion | Fetal growth restriction, abruption |
4d. Cerebral Pathophysiology - Why Seizures Occur
Two main theories, which may be complementary:
- Vasospasm/Ischemia theory: Cerebral vasospasm causes focal ischemia, triggering seizure activity.
- Hyperperfusion/PRES theory: Severe hypertension exceeds the upper limit of cerebral autoregulation, leading to posterior reversible encephalopathy syndrome (PRES) - vasogenic edema predominantly in the subcortical white matter of the parietooccipital lobes. This is supported by MRI findings in eclamptic women. (Harrison's Internal Medicine, 22e; Rosen's Emergency Medicine)
CT/MRI characteristically shows vasogenic edema in the posterior parieto-occipital regions - explaining the preponderance of visual symptoms (visual changes, cortical blindness) in these patients.
5. Pathological Changes (Organ-Specific)
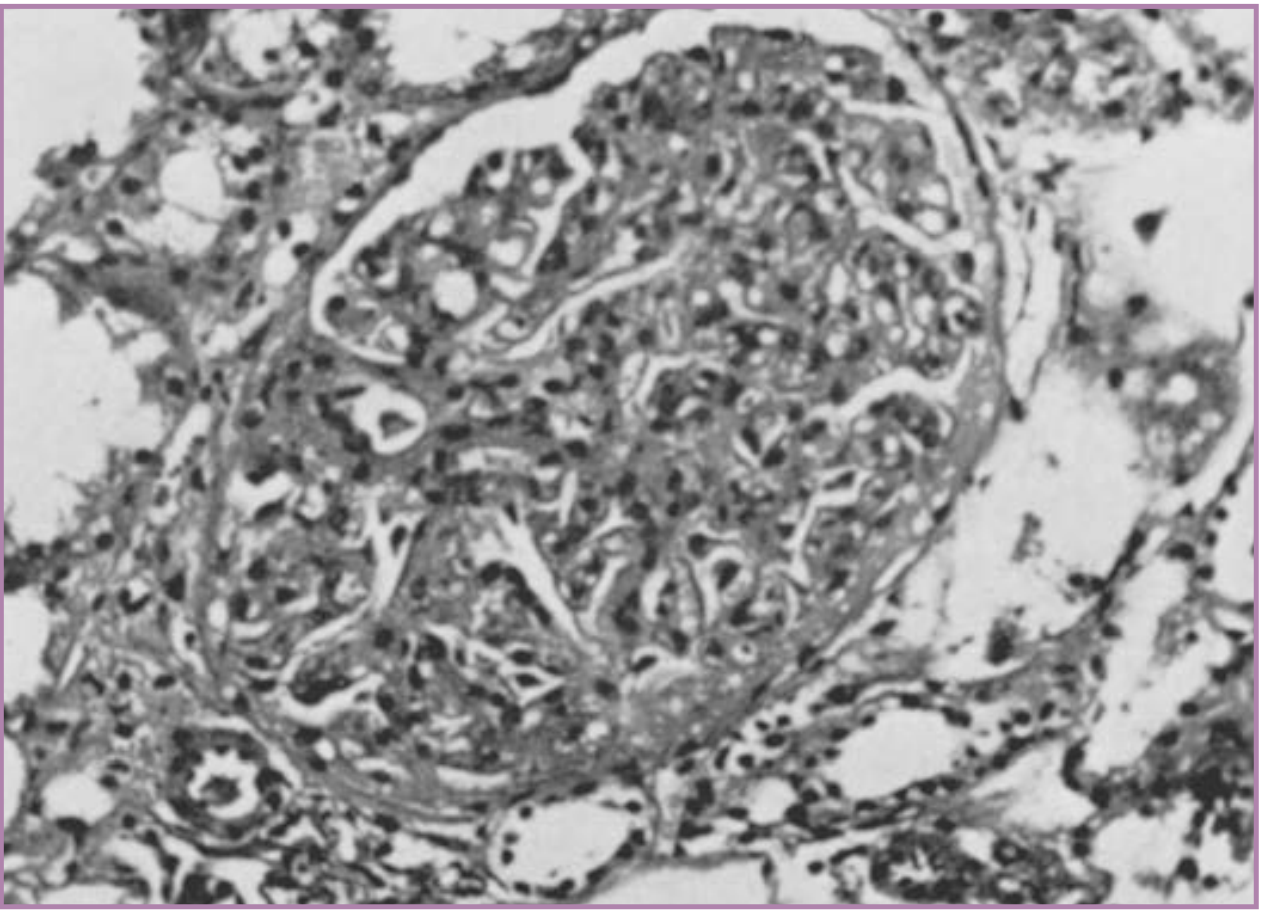
Kidney
- Glomerular capillary endotheliosis (hallmark) - endothelial swelling narrows capillary lumens to near obliteration.
- Enlarged glomeruli completely filling Bowman capsule with vacuolated appearance (shown in image below).
- Occurs in 70% of primiparas vs only 14% of multiparas with preeclampsia.
- These changes resolve within 5-10 weeks after delivery.
Liver
- Intense vasospasm causes hepatic infarction - small to large areas of periportal/sinusoidal necrosis extending toward portal vessels.
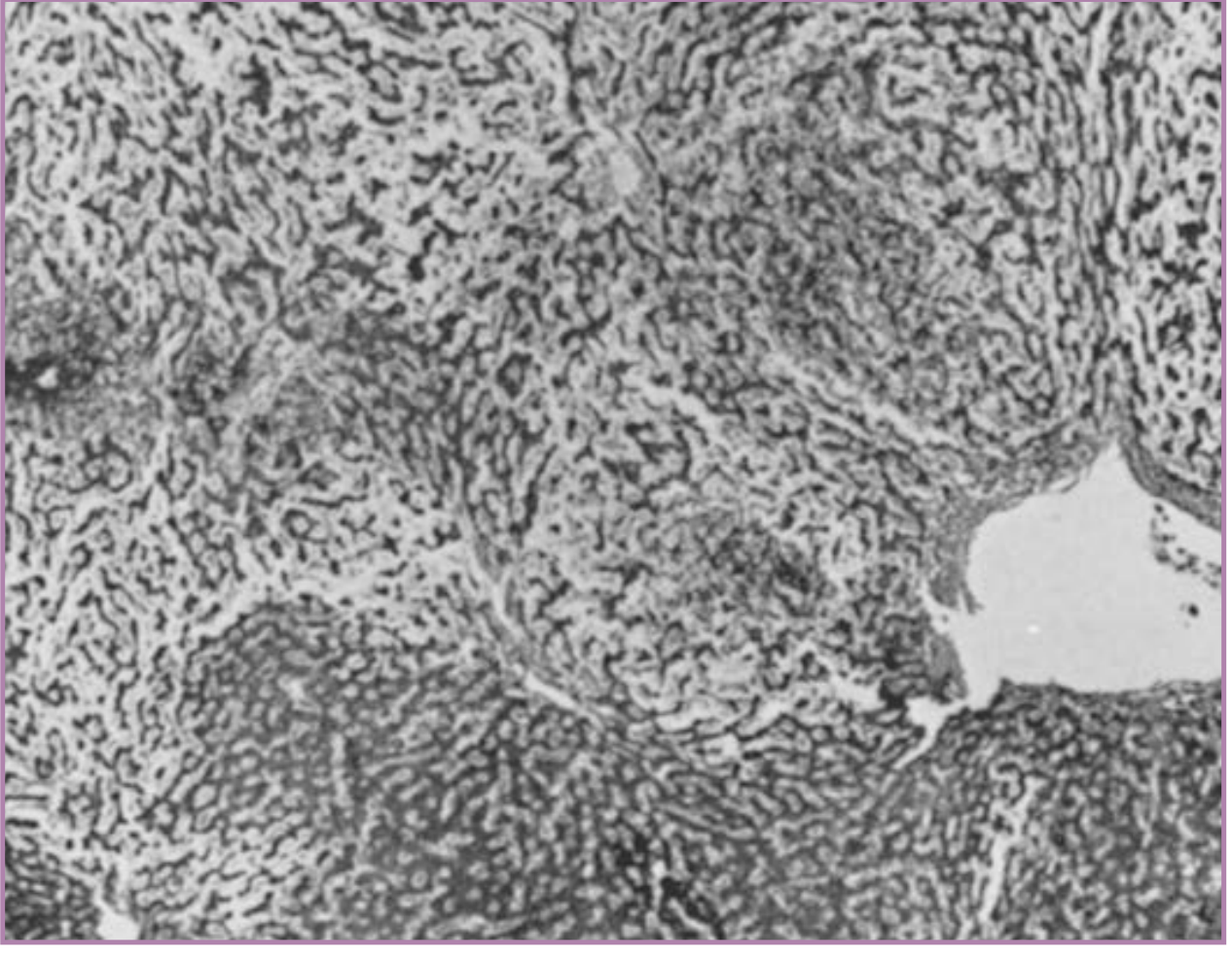
- HELLP syndrome (10% of severe preeclampsia): microangiopathic hemolytic anemia + elevated liver enzymes + low platelets ± DIC.
Placenta
- Multiple infarcts (far more numerous than in normal pregnancy)
- Retroplacental hemorrhage
- Ischemic villous changes (syncytial epithelial knots)
- Acute atherosis of decidual vessels (fibrinoid necrosis + lipid-laden macrophages)
Brain
- Petechial hemorrhages
- Thrombotic microangiopathy
- Vasogenic edema (parietooccipital predominance on imaging)
6. Clinical Features
Signs and Symptoms of Preeclampsia Preceding Eclampsia
Cerebral features (prodromal warning signs):
- Persistent, severe frontal/occipital headache (most important warning sign)
- Visual disturbances (blurred vision, scotomata, diplopia, cortical blindness)
- Dizziness, tinnitus, drowsiness
Renal:
- Oliguria (<500 mL/24 hr)
- Proteinuria (≥300 mg/24 hr or urine protein:creatinine ≥0.3)
- Rising creatinine
Hepatic:
- Epigastric or right upper quadrant pain (due to hepatic capsule stretch/infarction)
- Nausea and vomiting
- Elevated AST/ALT
Hematologic:
- Thrombocytopenia (<100,000/μL in HELLP)
- Microangiopathic hemolytic anemia
Pulmonary:
- Pulmonary edema (complicates 2-3% of severe preeclampsia)
The Eclamptic Seizure Itself
- Typically generalized tonic-clonic
- Usually preceded (seconds to minutes) by a prodrome: facial twitching or staring, followed by tonic phase then clonic phase
- Lasts 60-75 seconds on average
- Postictal confusion/coma follows
- May be followed by recurrent seizures or status eclampsia
- Can occur antepartum (50%), intrapartum (25%), or postpartum (25%)
7. Diagnostic Criteria
ACOG diagnostic criteria for preeclampsia (proteinuria no longer required if other severe features present):
- New onset BP ≥140/90 mmHg after 20 weeks in a previously normotensive woman
- PLUS one of: proteinuria, thrombocytopenia, renal insufficiency, impaired liver function, pulmonary edema, or new-onset headache/visual symptoms
Eclampsia = preeclampsia + new-onset seizures (not attributable to another cause)
Investigations:
- BP monitoring (continuous)
- CBC (thrombocytopenia, hemolysis)
- Liver function tests (AST, ALT, LDH)
- Serum creatinine, uric acid
- Urinalysis/24-hr urine protein or spot PCR ratio
- Fetal assessment (CTG, ultrasound)
- CT or MRI brain: not routinely required when diagnosis is apparent, but shows posterior vasogenic edema in PRES pattern
8. Management
Immediate Priorities (the "A-B-C" approach)
- Airway - lateral decubitus to prevent aspiration; suction; oxygen
- Prevent injury during seizure - padded side rails, do NOT restrain forcefully
- IV access - establish immediately
8a. Seizure Control and Prophylaxis - Magnesium Sulfate
Magnesium sulfate is the drug of choice for both treatment of active eclamptic seizures and prevention of recurrent seizures. It is superior to diazepam and phenytoin (proven in multiple RCTs including the landmark Magpie Trial of >10,000 women).
Standard IV Regimen (Pritchard/modified):
- Loading dose: 4-6 g IV in 100 mL, given over 20-30 minutes
- Maintenance: 2 g/hour IV infusion for at least 24 hours after last seizure or delivery (whichever is later)
IM Regimen (when IV access unavailable - Zuspan/Pritchard):
- Loading dose: 4 g IV + 5 g IM each buttock
- Maintenance: 5 g IM every 4 hours
Monitoring for toxicity (magnesium is renally excreted):
| Serum Mg (mg/dL) | Effect |
|---|---|
| 4-7 | Therapeutic (seizure prophylaxis) |
| 7-10 | Loss of patellar reflexes (early toxicity warning) |
| 10-13 | Respiratory paralysis |
| >15 | Cardiac arrest |
Clinical toxicity monitoring (every 1-2 hrs):
- Patellar reflexes (absent = approaching toxicity)
- Respiratory rate (should remain >12/min)
- Urine output (>25 mL/hr to ensure adequate excretion)
- Serum Mg levels in renal insufficiency
Antidote: Calcium gluconate 1 g IV (10 mL of 10% solution) - given for respiratory depression.
Renal insufficiency: Reduce to 2 g IV bolus and check serum Mg before increasing dose.
Duration of postpartum MgSO4 - Current Evidence:
A 2022 systematic review and meta-analysis (Sullivan et al., PMID 34187284) of 9 RCTs (n=1,369) found no statistically significant difference in eclampsia rates between <24 hr vs ≥24 hr regimens, though the two reported seizure cases occurred in the <24 hr group. Current recommendation: continue for 24 hours postpartum.
A 2023 Cochrane Review (Diaz et al., PMID 37815037) of 16 trials (3,020 women) found insufficient evidence to favor any alternative MgSO4 regimen over the standard, supporting continued use of the established loading + 24-hour maintenance protocol.
8b. Blood Pressure Control
Target: Treat when BP ≥150-160/100-110 mmHg to prevent cerebral hemorrhage.
Caution: Do NOT aggressively lower BP below ~140/90 mmHg - risks fetal distress from uteroplacental insufficiency.
| Agent | Route | Dose | Notes |
|---|---|---|---|
| Labetalol | IV | 20 mg bolus; repeat 20-80 mg q10min; max 300 mg | First-line parenteral; avoid in asthma |
| Hydralazine | IV | 5-10 mg q20min | Classic choice; may cause reflex tachycardia |
| Nifedipine | PO | 10-20 mg q20-30min (immediate release) | Oral; may enhance MgSO4 effect |
| Methyldopa | PO | 250-500 mg q8h | First-line oral; most safety data in pregnancy |
| Nicardipine | IV infusion | 5-15 mg/hr | Useful in severe hypertension |
| Nitroprusside | IV | Last resort | Risk of fetal cyanide toxicity; avoid if possible |
Contraindicated in pregnancy: ACE inhibitors, ARBs (teratogenic)
8c. Definitive Treatment - Delivery
Delivery is the only definitive cure for eclampsia.
Timing:
- <24 weeks: Termination usually recommended due to >80% perinatal mortality and high maternal risk
- 24-34 weeks: Balance fetal benefit of prolonged gestation vs. maternal risk; expectant management with intensive monitoring may be appropriate; corticosteroids for fetal lung maturity
- 34-37 weeks: ACOG recommends delivery
- ≥37 weeks: Immediate delivery indicated
- Eclampsia: Delivery is indicated regardless of gestational age once mother is stabilized
Mode of delivery: No RCT evidence favoring cesarean over induction of labor; mode is dictated by obstetric indications (fetal presentation, cervical status, urgency). Both are acceptable.
8d. Ancillary Management
- Coagulopathy/HELLP: Replace platelets if <50,000 or active bleeding; replace coagulation factors for DIC
- Pulmonary edema: Furosemide; fluid restriction (MgSO4 infusion already adds fluid load)
- Fetal monitoring: Continuous CTG during seizure and post-seizure (transient bradycardia is common)
- Transfer: If obstetric services unavailable, stabilize and transfer to a tertiary center
9. HELLP Syndrome (Severe Variant)
HELLP = Hemolytic anemia + Elevated Liver enzymes + Low Platelets
- Complicates ~10% of severe preeclampsia
- Can occur without proteinuria or significant hypertension
- Diagnostic criteria: Platelets <100,000/μL + LDH >600 U/L + AST/ALT >2x upper normal
- Complications include: eclampsia (6%), placental abruption (10%), acute renal failure (5%), DIC (8%), pulmonary edema (10%), hepatic hemorrhage/rupture (rare but life-threatening)
10. Prognosis and Long-Term Outcomes
- Hypertension and proteinuria typically resolve within 1-2 weeks after delivery
- Glomerular changes resolve within 5-10 weeks postpartum
- Most cases leave no lasting sequelae if managed promptly
- Women who have had eclampsia may have subtle long-term impairment in cognitive function
- Risk of recurrence in subsequent pregnancies: previous preeclampsia is the strongest single risk factor (RR 7.19)
- Long-term cardiovascular risk is elevated (hypertension, CVD later in life)
11. Differential Diagnosis of Seizures in Pregnancy
| Condition | Key Distinguishing Features |
|---|---|
| Epilepsy | Prior seizure history; no hypertension/proteinuria |
| Thrombotic thrombocytopenic purpura (TTP) | Pentad: thrombocytopenia, hemolysis, fever, renal, neuro |
| Hyponatremia | Sodium level <120; no hypertension |
| Cerebral venous thrombosis | MRI/MRV; focal deficits; no hypertensive pattern |
| Intracranial hemorrhage | CT head; sudden onset headache |
| Meningitis/encephalitis | Fever, CSF findings |
Key Sources:
- Creasy & Resnik's Maternal-Fetal Medicine, 9e - Chapters 45 & 48 (Preeclampsia and Eclampsia, comprehensive pathophysiology and management)
- Brenner and Rector's The Kidney - Magnesium and seizure prophylaxis, antihypertensive management
- Robbins & Kumar Basic Pathology - Pathogenesis and morphology (glomerular endotheliosis, hepatic infarction)
- Tintinalli's Emergency Medicine - Clinical management protocol
- Harrison's Principles of Internal Medicine, 22e - PRES and cerebral pathophysiology
- Sullivan M et al. Duration of postpartum MgSO4 for seizure prophylaxis. J Matern Fetal Neonatal Med. 2022. PMID 34187284 - 9 RCTs; supports 24-hour regimen.
- Diaz V et al. Alternative MgSO4 regimens for pre-eclampsia and eclampsia. Cochrane Database Syst Rev. 2023. PMID 37815037 - Standard regimen remains the evidence-based choice.
This is a shared conversation. Sign in to Orris to start your own chat.