What is edema. Causes and treatment of edema
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
I now have rich, authoritative content from multiple textbooks. Let me compile the comprehensive answer.
Edema
Definition
Edema is an abnormal accumulation of interstitial fluid within tissues. About 60% of lean body weight is water; two-thirds is intracellular and most of the remainder is interstitial fluid. When interstitial fluid accumulates beyond normal, edema results.
Fluid can also collect in body cavities:
-
Hydrothorax - pleural cavity
-
Hydropericardium - pericardial cavity
-
Hydroperitoneum (ascites) - peritoneal cavity
-
Anasarca - severe generalized edema with profound subcutaneous swelling and fluid in body cavities
-
Robbins & Kumar Basic Pathology, p. 78-79
Pathophysiology
Fluid movement across capillary walls is governed by two opposing forces:
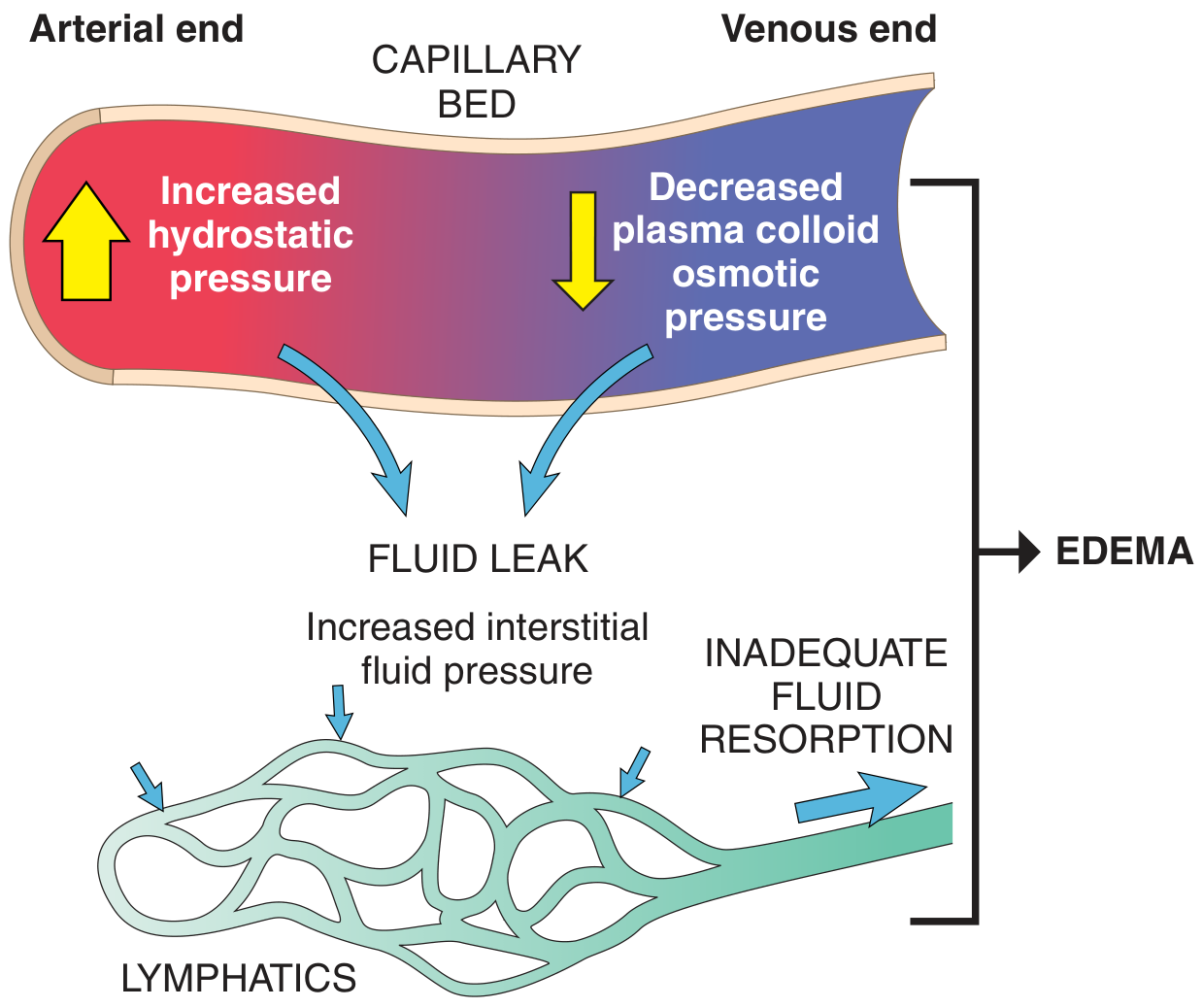
- Vascular hydrostatic pressure - pushes fluid OUT of capillaries into the interstitium
- Plasma colloid osmotic (oncotic) pressure - pulls fluid BACK into capillaries
Normally these are balanced, and the small net outflow into the interstitium is drained by lymphatics back to the circulation. Edema occurs when:
- Hydrostatic pressure increases, OR
- Colloid osmotic pressure decreases, OR
- Lymphatic drainage is blocked, OR
- Vascular permeability increases (inflammation)
Transudate (protein-poor fluid) = high hydrostatic or low oncotic pressure
Exudate (protein-rich fluid) = increased vascular permeability (inflammation)
Causes of Edema
Here is a summary diagram of peripheral edema causes:
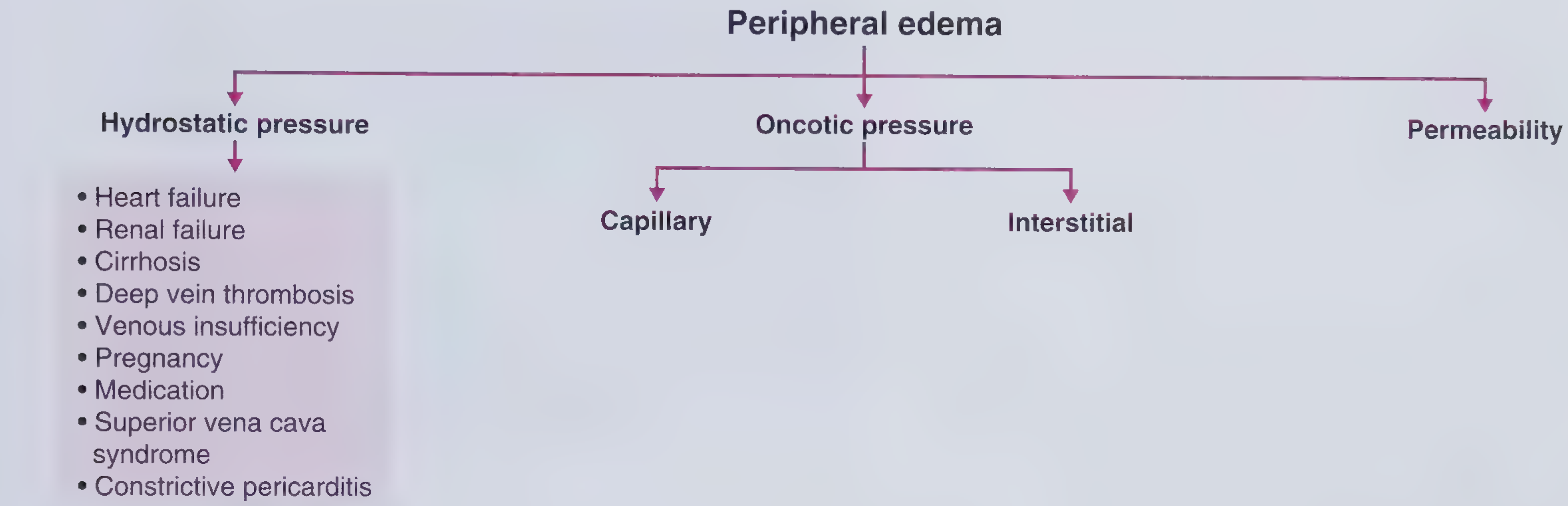
1. Increased Hydrostatic Pressure
Caused mainly by disorders that impair venous return:
| Cause | Mechanism |
|---|---|
| Congestive heart failure | Reduced cardiac output → venous pooling + renal sodium/water retention via RAAS |
| Deep vein thrombosis (DVT) | Local venous obstruction → unilateral leg edema |
| Renal failure | Sodium and water retention → increased intravascular volume |
| Liver cirrhosis | Portal hypertension → ascites and lower limb edema |
| Constrictive pericarditis | Impaired cardiac filling → elevated venous pressure |
| Venous insufficiency | Incompetent valves → chronic venous hypertension |
| Superior vena cava (SVC) syndrome | Obstruction of the SVC → face, neck, upper limb edema |
| Pregnancy | Inferior vena cava compression by gravid uterus |
| Prolonged limb dependency / inactivity | Reduced venous pump |
In congestive heart failure, a vicious cycle develops: reduced cardiac output → renal hypoperfusion → RAAS activation → Na+/water retention → increased venous pressure → worsening edema. This responds to salt restriction, diuretics, and aldosterone antagonists. - Robbins & Kumar Basic Pathology, p. 80
2. Reduced Plasma Osmotic (Oncotic) Pressure
Caused by hypoalbuminemia (plasma albumin < 2 g/dL is associated with edema):
| Cause | Mechanism |
|---|---|
| Nephrotic syndrome | Glomerular damage → albumin lost in urine |
| Liver disease (cirrhosis) | Decreased albumin synthesis |
| Malnutrition / kwashiorkor | Inadequate protein intake |
| Protein-losing enteropathy | GI losses of protein |
Low albumin leads to edema, reduced intravascular volume, renal hypoperfusion, and secondary hyperaldosteronism - which worsens edema because the primary defect (low protein) persists. - Robbins & Kumar Basic Pathology, p. 80
3. Lymphatic Obstruction (Lymphedema)
Impaired lymphatic drainage prevents resorption of interstitial fluid:
| Cause | Example |
|---|---|
| Parasitic infection | Filariasis - causes elephantiasis (massive lower limb edema) |
| Malignancy | Lymphoma obstructing lymphatics; breast cancer causing peau d'orange |
| Post-surgical / irradiation | Axillary node dissection in breast cancer → arm lymphedema |
| Iatrogenic | Radiation treatment disrupting lymphatics |
- Robbins & Kumar Basic Pathology, p. 80
4. Increased Vascular Permeability (Inflammatory Edema)
In inflammation, mediators such as histamine, bradykinin, leukotrienes, and cytokines increase capillary permeability, allowing protein-rich fluid to leak out. This produces an exudate. Examples:
- Allergic reactions / anaphylaxis
- Burns
- Sepsis / ARDS
- Infections
5. Sodium and Water Retention
Excessive salt retention increases hydrostatic pressure and dilutes plasma proteins:
- Renal failure
- Primary hyperaldosteronism
- Drugs (corticosteroids, NSAIDs, some antihypertensives)
6. Medications (Iatrogenic Edema)
Common culprits include:
- Calcium channel blockers (amlodipine)
- NSAIDs
- Corticosteroids
- Thiazolidinediones (e.g., pioglitazone)
- Hormonal therapy (estrogens)
Clinical Features
| Type | Characteristics |
|---|---|
| Heart failure | Bilateral, symmetric, dependent, pitting; gradual onset; legs primarily; may have ascites/pleural effusions |
| Renal failure | Similar to right heart failure; generalized |
| Cirrhosis | Bilateral, pitting, dependent; mainly lower limbs; ascites prominent |
| DVT | Unilateral, dependent, pitting; acute onset; associated with pain and erythema |
| SVC syndrome | Face, neck, bilateral arms |
| Lymphedema | Non-pitting (in chronic stage); involves limb; may be unilateral |
| Nephrotic syndrome | Periorbital edema (morning), then generalized; associated with proteinuria |
- Frameworks for Internal Medicine, p. 308-309
Treatment of Edema
Treatment is directed at the underlying cause plus symptomatic fluid removal:
1. Treat the Underlying Cause
- Heart failure: ACE inhibitors, ARBs, beta-blockers, cardiac resynchronization
- Renal failure: Hemodialysis or peritoneal dialysis to maintain fluid balance
- Nephrotic syndrome: Treat underlying glomerular disease; RAAS blockade; corticosteroids (where indicated)
- Cirrhosis: Treat liver disease; reduce portal hypertension
- DVT: Anticoagulation (heparin, then warfarin or DOACs)
- SVC syndrome: Treat underlying malignancy (chemotherapy, radiation, stenting)
- Lymphedema: Treat underlying infection or malignancy
2. Dietary Sodium and Fluid Restriction
- Sodium restriction is a cornerstone of edema management in heart failure, cirrhosis, and renal failure
- Diuretics work better when combined with low-sodium diet
3. Diuretics
The most widely used pharmacological treatment:
| Diuretic Class | Examples | Used in |
|---|---|---|
| Loop diuretics | Furosemide, bumetanide | Heart failure, renal failure, pulmonary edema |
| Thiazide diuretics | Hydrochlorothiazide | Mild edema, hypertension-related |
| Aldosterone antagonists | Spironolactone, eplerenone | Heart failure, cirrhosis (reduces secondary hyperaldosteronism) |
| Osmotic diuretics | Mannitol | Cerebral edema |
Note: In severe heart failure, bowel wall edema can impair oral diuretic absorption - parenteral (IV) administration is required. - Frameworks for Internal Medicine, p. 308
4. Mechanical / Physical Measures
- Leg elevation - reduces dependent edema by promoting venous return
- Compression stockings - chronic venous insufficiency, DVT prevention, lymphedema
- Compression bandaging - lymphedema management
- Manual lymphatic drainage - physiotherapy for lymphedema
5. Dialysis / Ultrafiltration
- For renal failure with hypervolemia: hemodialysis or peritoneal dialysis
- Plasma ultrafiltration can remove several liters per day in severe pulmonary edema
- Frameworks for Internal Medicine, p. 308
6. Albumin Infusion
- Used in hypoalbuminemia (nephrotic syndrome, cirrhosis) to temporarily restore oncotic pressure
- Combined with diuretics for best effect in cirrhotic ascites
7. Specific Interventions
- Paracentesis - large-volume drainage of ascites in cirrhosis
- Thoracentesis - drainage of large pleural effusions (hydrothorax)
- Surgical/endovascular - venous stenting in SVC syndrome; lymphovenous anastomosis in lymphedema
Summary Table
| Mechanism | Key Causes | Treatment Focus |
|---|---|---|
| ↑ Hydrostatic pressure | Heart failure, DVT, renal failure, cirrhosis | Diuretics, Na restriction, treat primary disease |
| ↓ Oncotic pressure | Nephrotic syndrome, cirrhosis, malnutrition | Treat underlying disease, albumin, diuretics |
| Lymphatic obstruction | Filariasis, malignancy, post-surgical | Compression, physiotherapy, treat cause |
| ↑ Vascular permeability | Inflammation, burns, sepsis, allergy | Anti-inflammatory, treat infection, manage ARDS |
| Na/H2O retention | Renal failure, aldosteronism, drugs | Dietary restriction, diuretics, dialysis |
Sources:
- Robbins & Kumar Basic Pathology (Robbins Pathology), pp. 78-80
- Frameworks for Internal Medicine, pp. 307-310
- Goldman-Cecil Medicine International Edition
- Harrison's Principles of Internal Medicine 22E
This is a shared conversation. Sign in to Orris to start your own chat.