Hello
See iam a third year mbbs students appearing for final exams in following 28 days So when ever I ask question and mention marks give answers in such a way that i can get good marks For spm - refer park and cia with diagrams tabular forms wherever necessary Fmt- Narayan Reddy and mudabbir
- Primary reference: Park's Textbook of PSM + CIA (Community & Investigative approaches)
- Answers will include:
- Diagrams wherever relevant
- Tabular comparisons
- Definitions, classifications, and exam-ready points
- Mnemonics when helpful
- Primary reference: Narayan Reddy + Mudabbir
- Answers will include:
- Medicolegal points highlighted
- Important definitions
- Diagrams (wound patterns, instruments, etc.)
- High-yield exam points
- Structure answers with headings and subheadings
- Lead with a definition when applicable
- Use tables for comparisons and classifications
- Add diagrams/flowcharts in text form where visual aids help
- Highlight high-yield exam points
Define balanced diet Proximal principles of nutrition Enumerate the major nutritional problems in india What are the components of nutritional assessment Describe how will you conduct nutritional assessment in a community 20 marks long note
NUTRITION - BALANCED DIET, PROXIMATE PRINCIPLES, NUTRITIONAL PROBLEMS & ASSESSMENT
(20 Marks | Ref: Park's Textbook of PSM)
I. DEFINITION OF BALANCED DIET
"One which contains a variety of foods in such quantities and proportions that the need for energy, amino acids, vitamins, minerals, fats, carbohydrates and other nutrients is adequately met for maintaining health, vitality and general well-being, and also makes a small provision for extra nutrients to withstand short duration of leanness." - Park
II. PROXIMATE PRINCIPLES OF NUTRITION
A. Macronutrients ("Proximate Principles")
Proteins, fats, and carbohydrates are often called "proximate principles" because they form the main bulk of food.
| Proximate Principle | Contribution to Daily Energy Intake (Indian Dietary) |
|---|---|
| Proteins | 10 - 15% |
| Fats | 15 - 30% |
| Carbohydrates | 50 - 80% |
1. Proteins
- Complex organic nitrogenous compounds (C, H, O, N, S)
- Constitute ~20% of body weight in adults
- Nitrogen content ~16%
- 9 Essential Amino Acids (EAA): Leucine, Isoleucine, Lysine, Methionine, Phenylalanine, Threonine, Valine, Tryptophan, Histidine
- Mnemonic: "PVT TIM HaLL" - Phenylalanine, Valine, Threonine, Tryptophan, Isoleucine, Methionine, Histidine, Leucine, Lysine
- A protein is "biologically complete" if it contains all EAA (e.g., animal proteins)
2. Fats
- Most concentrated source of energy (9 kcal/g)
- Essential fatty acids (EFA): Linoleic acid, Linolenic acid, Arachidonic acid
- Function: Energy reserve, fat-soluble vitamin carrier (A, D, E, K), cell membrane structure
3. Carbohydrates
- Primary energy source (4 kcal/g)
- Should be rich in natural fibre
- Types: Monosaccharides, Disaccharides, Polysaccharides
B. Micronutrients
- Vitamins (fat-soluble and water-soluble) and Minerals
- Required in small amounts (fraction of mg to several grams)
Principles of Constructing a Balanced Diet:
- First meet protein requirement (10-15% of daily energy)
- Then limit fat to 15-30% of energy
- Carbohydrates rich in natural fibre constitute the remaining energy
- Requirements of micronutrients must be met (as per RDA 2020)
FOOD GUIDE PYRAMID (Park's Fig. 1)
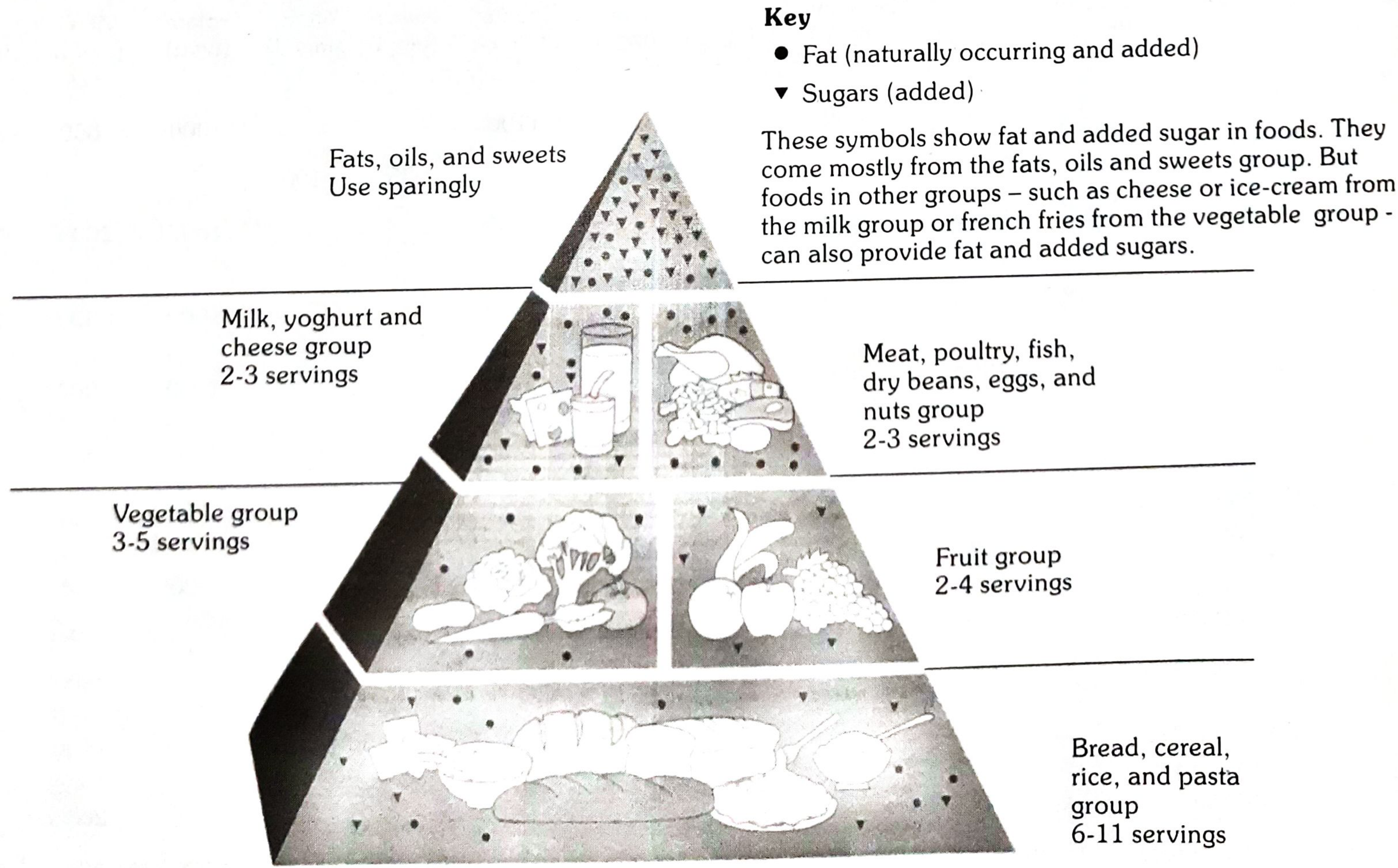
| Level | Food Group | Servings/Day |
|---|---|---|
| Base | Bread, cereal, rice, pasta | 6-11 |
| 2nd | Vegetables | 3-5 |
| 2nd | Fruits | 2-4 |
| 3rd | Milk, yoghurt, cheese | 2-3 |
| 3rd | Meat, poultry, fish, eggs, nuts | 2-3 |
| Apex | Fats, oils, sweets | Use sparingly |
Note: Diet should be adapted to special needs of growth, pregnancy, lactation, physical activity, and medical disorders (e.g., diabetes).
III. MAJOR NUTRITIONAL PROBLEMS IN INDIA
"From the nutritional point of view, the Indian society is a dual society - a small group of well fed and a very large group of undernourished." - Park
| # | Nutritional Problem | Key Facts |
|---|---|---|
| 1 | Protein-Energy Malnutrition (PEM) | "Food gap" is chief cause; 80% are mild-moderate cases; severe cases 1-2% in preschool children; Marasmus > Kwashiorkor |
| 2 | Nutritional Anaemia | India has highest prevalence worldwide; ~50% non-pregnant women + children anaemic; 50.3% pregnant women anaemic; 19% maternal deaths due to anaemia; Iron deficiency is most common cause |
| 3 | Low Birth Weight (LBW) | ~28% of all births in India are LBW (<2.5 kg); caused by maternal malnutrition and anaemia |
| 4 | Xerophthalmia (Nutritional Blindness) | 0.04% of total blindness due to Vitamin A deficiency; Keratomalacia major cause in children 1-3 years |
| 5 | Iodine Deficiency Disorders (IDD) | Endemic in sub-Himalayan regions; 263 out of 324 districts surveyed are endemic (>10% prevalence); >71 million people affected |
| 6 | Others | Lathyrism, endemic fluorosis, widespread food adulteration |
According to NFHS-4: 53.1% women are anaemic; anaemia in children aged 6-59 months is 58.4%
IV. COMPONENTS OF NUTRITIONAL ASSESSMENT
(A) Objectives of Nutritional Assessment:
- Obtain precise information on prevalence and geographic distribution of nutritional problems
- Identify individuals or population groups "at risk"
- Develop health care programmes that meet defined needs
- Evaluate effectiveness of nutrition programmes
(B) Components (Methods) - "CABFVE" mnemonic:
| # | Component | Key Details |
|---|---|---|
| 1 | Clinical Examination | Physical signs of deficiency; standardized survey forms |
| 2 | Anthropometry | Height, weight, skinfold thickness, MUAC, head/chest circumference |
| 3 | Biochemical Evaluation | Hb estimation, serum retinol, urinary iodine, enzyme assays |
| 4 | Functional Assessment | Work capacity, immune function tests |
| 5 | Vital and Health Statistics | Mortality data, morbidity records, infant mortality rate |
| 6 | Ecological Studies | Food balance sheets, socioeconomic factors |
| + | Dietary Intake Assessment | 24-hr recall, food frequency questionnaire, weighed dietary record |
V. CONDUCTING NUTRITIONAL ASSESSMENT IN A COMMUNITY
Step 1: Planning the Survey
- Define objectives clearly
- Decide type of survey: Cross-sectional OR Longitudinal
- Plan sampling: Random and representative sample covering all ages, both sexes, different socio-economic groups
- Seek expert statistical advice
- Decide duration and standardization of measurement techniques
"It is not necessary to examine all persons in a given community." - Park
Step 2: Clinical Examination
- Systematic head-to-toe examination using standardized survey forms (Annexure I schedule)
- Look for physical signs of nutritional deficiency
| Category | Signs |
|---|---|
| Not related to nutrition | Alopecia, pyorrhoea, pterygium |
| Need further investigation | Malar pigmentation, corneal vascularization, geographic tongue |
| Known to be of value | Angular stomatitis, Bitot's spots, calf tenderness, absent knee/ankle jerks (Beri-beri), thyroid enlargement (Goitre) |
- Malnutrition cannot be quantified
- Many deficiencies have no physical signs
- Lack of specificity and subjective nature
Step 3: Anthropometric Measurements
| Measurement | Use |
|---|---|
| Weight & Height | BMI calculation; growth monitoring |
| Skinfold thickness | Body fat estimation |
| Mid-Upper Arm Circumference (MUAC) | PEM screening in children |
| Head circumference | Brain growth in children <2 yrs |
| Chest circumference | Nutritional status in infants |
| BMI (kg/m²) | Category |
|---|---|
| <18.5 | Underweight |
| 18.5-24.9 | Normal |
| 25-29.9 | Overweight |
| ≥30 | Obese |
Step 4: Biochemical/Laboratory Assessment
- Haemoglobin estimation - most important test in nutrition surveys
- RBC count and haematocrit
- Stool examination - for intestinal parasites
- Urine - for albumin, sugar
- Serum retinol (Vitamin A status)
- Serum iron / Serum ferritin (Iron stores)
- Urinary iodine (Iodine status)
- Enzyme assays (e.g., erythrocyte glutathione reductase for Riboflavin)
- These detect preclinical (subclinical) malnutrition before clinical signs appear
Step 5: Assessment of Dietary Intake
| Method | Description |
|---|---|
| 24-hour dietary recall | Subject recalls all food consumed in previous 24 hours |
| Food frequency questionnaire | How often specific foods are consumed |
| Weighed dietary record | Actual weighing of food before and after eating |
| Food balance sheets | National-level food availability data |
Step 6: Vital and Health Statistics
- Infant Mortality Rate (IMR)
- Under-5 mortality rate
- Morbidity data from hospitals/PHCs
- Maternal mortality rate
- Growth monitoring data (ICDS registers)
Step 7: Ecological Studies
- Assessment of socioeconomic factors (income, education, occupation)
- Environmental factors (sanitation, water supply)
- Cultural factors (food taboos, feeding practices)
- Agricultural data (food production, availability)
DIAGRAM: Methods of Nutritional Assessment & Natural History of Disease (Park's Fig. 5)
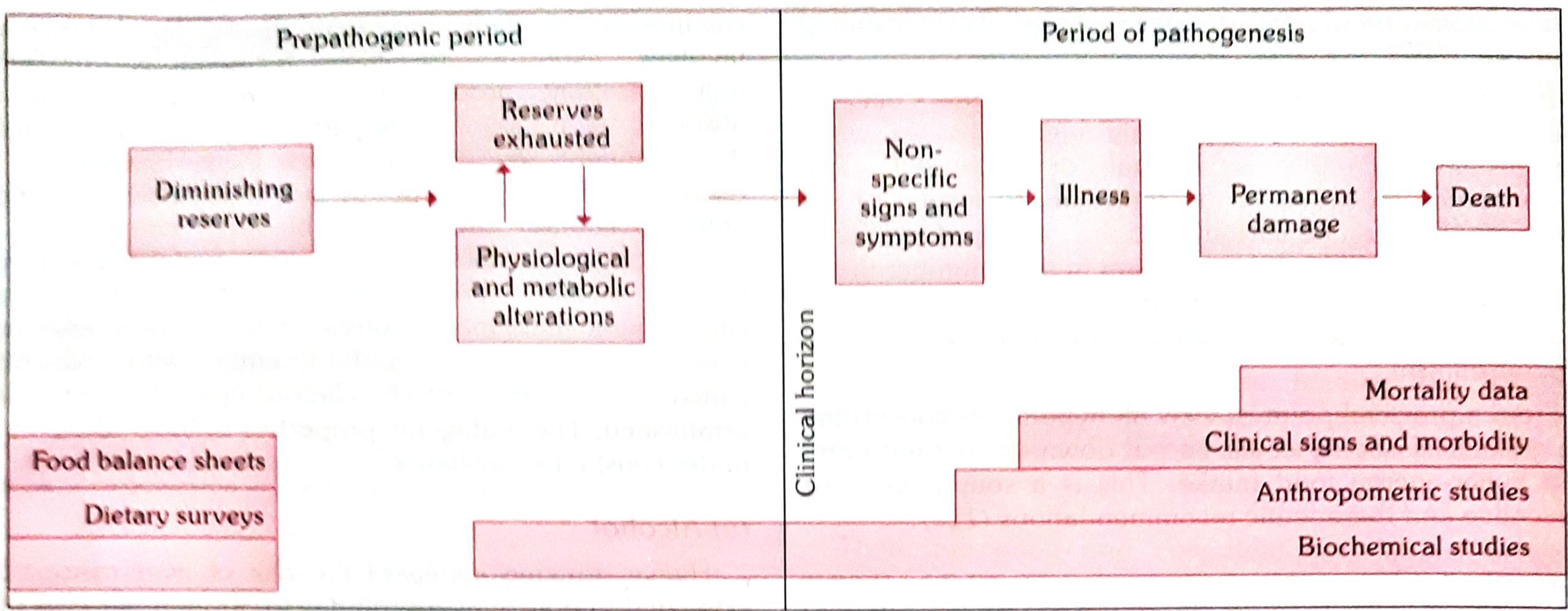
Key concept from diagram: Biochemical studies can detect malnutrition even in the prepathogenic period (before any clinical signs), while clinical signs and mortality data become apparent only after the clinical horizon is crossed.
Summary Flowchart - Community Nutritional Assessment
PLAN SURVEY
(Objectives → Sampling → Statistical design)
↓
CLINICAL EXAMINATION
(Physical signs, standardized schedule)
↓
ANTHROPOMETRY
(Ht, Wt, MUAC, Skinfold, BMI)
↓
BIOCHEMICAL TESTS
(Hb, Serum retinol, Urinary iodine)
↓
DIETARY INTAKE ASSESSMENT
(24-hr recall, FFQ, Weighed record)
↓
VITAL STATISTICS
(IMR, MMR, Morbidity data)
↓
ECOLOGICAL STUDIES
(Socioeconomic, cultural, environmental factors)
↓
ANALYSIS & REPORT
(Identify "at-risk" groups → Plan intervention)
High-Yield Exam Points to Remember:
- Balanced diet = Variety + Adequate quantity + Proportions that meet all nutrient needs + Small provision for lean periods
- Proximate principles = Proteins + Fats + Carbohydrates (macronutrients - main bulk of food)
- Nutritional anaemia = most prevalent nutritional problem in Indian women and children
- Marasmus > Kwashiorkor in India
- Most important lab test in nutrition survey = Haemoglobin estimation
- Biochemical tests detect malnutrition in preclinical stages (before clinical signs)
- "Not all persons need to be examined" - random representative sample is sufficient
Add More points acc to park textbook to nutritional assessment in a community
NUTRITIONAL ASSESSMENT IN A COMMUNITY
(Complete - As per Park's Textbook of PSM)
DEFINITION & OBJECTIVES
- Obtain precise information on prevalence and geographic distribution of nutritional problems
- Identify individuals or population groups "at risk" or in greatest need of assistance
- Formulate policies based on defined problems
- Develop health care programmes that meet assessed needs
- Evaluate effectiveness of ongoing nutrition programmes
PLANNING THE SURVEY
- Duration of the survey
- Type of survey: Cross-sectional OR Longitudinal
- Sampling strategy: Random + representative sample covering:
- All age groups
- Both sexes
- Different socio-economic groups
- Standardization of measurement techniques and survey instruments
- Statistical advice from experts
- Opportunity to conduct an intensive investigation on a sub-sample
"It is not necessary to examine all persons. Examination of a random and representative sample is sufficient to draw valid conclusions." - Park
METHODS OF NUTRITIONAL ASSESSMENT
DIAGRAM: Natural History of Disease & Assessment Methods (Park's Fig. 5)
Key point: Biochemical studies can detect malnutrition even in the prepathogenic period. Clinical signs and mortality data appear only after the clinical horizon is crossed.
1. CLINICAL EXAMINATION
- Systematic head-to-toe examination
- Standardized survey forms/schedules covering all areas of the body (Annexure I)
- Diagnostic significance is greatly enhanced when two or more clinical signs are present simultaneously
| Category | Examples |
|---|---|
| Not related to nutrition | Alopecia, pyorrhoea, pterygium |
| Need further investigation | Malar pigmentation, corneal vascularization, geographic tongue |
| Known to be of value | Angular stomatitis, Bitot's spots, calf tenderness, absent knee/ankle jerks (Beri-beri), thyroid enlargement (Goitre) |
- Malnutrition cannot be quantified by clinical signs
- Many deficiencies are unaccompanied by physical signs
- Lack of specificity and subjective nature of most signs
2. ANTHROPOMETRY
| Measurement | Purpose |
|---|---|
| Height & Weight | BMI; growth monitoring; Gomez/IAP classification of PEM |
| Skinfold thickness | Estimation of body fat |
| Mid-Upper Arm Circumference (MUAC) | Screening for PEM in children; quick field tool |
| Head circumference | Brain growth; children <2 years |
| Chest circumference | Nutritional status in infants |
| Head:Chest circumference ratio | Normal >1 up to 6 months, <1 after 1 year |
Anthropometric data can be collected by non-medical personnel given sufficient training.
| BMI (kg/m²) | Category |
|---|---|
| <18.5 | Underweight |
| 18.5 - 24.9 | Normal |
| 25 - 29.9 | Overweight |
| ≥ 30 | Obese |
3. LABORATORY AND BIOCHEMICAL ASSESSMENT
| Test | Significance |
|---|---|
| Haemoglobin estimation | Most important test in nutrition surveys; index of overall nutrition state |
| RBC count + Haematocrit | Assessment of anaemia |
| Stool examination | Detect intestinal parasites, chronic dysentery |
| Urine examination | Albumin, sugar |
| Nutrient | Test | Normal Value |
|---|---|---|
| Vitamin A | Serum retinol | 20 mcg/dL |
| Thiamine (B1) | TPP stimulation of RBC transketolase | Ratio 1.00-1.23 |
| Riboflavin (B2) | RBC glutathione reductase stimulated by FAD | Ratio 1.0-1.2 |
| Niacin | Urine N-methyl nicotinamide | (not very reliable) |
| Folate | Serum folate / Red cell folate | 6.0 mcg/mL / 160 mcg/mL |
| Vitamin B12 | Serum B12 concentration | 160 mg/L |
| Vitamin C | Leucocyte ascorbic acid | 15 mcg/10⁹ cells |
| Vitamin K | Prothrombin time | 11-16 seconds |
| Protein | Serum albumin | 35 g/L |
| Transferrin | 20 g/L | |
| Thyroid-binding pre-albumin | 250 mg/L | |
| Iron | Serum iron / Serum ferritin | Reflects iron stores |
| Iodine | Urinary iodine | Reflects iodine status |
- Time-consuming and expensive
- Cannot be applied on a large scale to whole community
- Often carried out only on a subsample of the population
- Most biochemical tests reveal only current nutritional status
- If clinical examination raises a question, biochemical tests may be invoked to prove or disprove it
4. FUNCTIONAL INDICATORS
| System | Test | Nutrient Involved |
|---|---|---|
| Structural integrity | Erythrocyte fragility | Vit E, Se |
| Capillary fragility | Vit C | |
| Tensile strength | Copper (Cu) | |
| Host defence (Immunity) | Leucocyte chemotaxis | Protein/Energy, Zn |
| Leucocyte phagocytic capacity | P/E, Fe | |
| Leucocyte bactericidal capacity | P/E, Fe, Se | |
| T cell blastogenesis | P/E, Zn | |
| Delayed cutaneous hypersensitivity (DCH) | P/E, Zn | |
| Haemostasis | Prothrombin time | Vit K |
| Reproduction | Sperm count | Energy, Zn |
| Nerve function | Nerve conduction velocity | P/E, Vit B1, B12 |
| Dark adaptation | Vit A, Zn | |
| EEG | P/E | |
| Work capacity | Heart rate | P/E, Fe |
| Vasopressor response | Vit C |
5. ASSESSMENT OF DIETARY INTAKE
| Method | Description | Use |
|---|---|---|
| Weighment of Raw Foods | Survey team visits households; weighs all food to be cooked + waste; 7-day "dietary cycle" | Widely used in India; fairly accurate |
| Weighment of Cooked Foods | Foods analyzed in state normally consumed | More accurate but not easily acceptable |
| Oral Questionnaire (24-hr recall) | Retrospective inquiry about food eaten in previous 24-48 hours | Large populations; quick |
- Mean intake (grams) of food in terms of cereals, pulses, etc.
- Nutritive value (energy, protein, fat, vitamins, minerals) - using ICMR's "Nutritive Value of Indian Foods" publication
- Comparison with Recommended Dietary Allowances (RDA) to identify dietary inadequacies
- Identifies dietary inadequacies against present standards
- Valuable for planning health education activities
- Helps assess changes needed in agriculture and food production
- Identifies specific foods consumed and intake patterns
6. VITAL STATISTICS
| Vital Statistic | Nutritional Relevance |
|---|---|
| Mortality rate in 1-4 years | Most closely related to malnutrition; in developing countries may be 20x higher than developed |
| Infant Mortality Rate (IMR) | Influenced by nutritional status |
| Second-year mortality rate | Reflects post-weaning malnutrition |
| Rate of Low Birth Weight babies | Reflects maternal nutritional status |
| Life expectancy | Broad index of nutritional wellbeing |
- Protein Energy Malnutrition (PEM)
- Anaemia
- Xerophthalmia, other vitamin deficiencies
- Endemic goitre
- Diarrhoea, measles, parasitic infestations
Limitation: Mortality data alone does NOT provide a satisfactory picture of nutritional status of a population.
7. ASSESSMENT OF ECOLOGICAL FACTORS
- Indirect method of assessing food consumption
- Supplies related to census population → derive per capita food supply
- Refers to country as a whole (conceals regional differences)
- Advantage: Cheaper and simpler than direct methods
- Gives general pattern of food consumption in the country
- Family size, occupation, income, education
- Cultural patterns in relation to feeding practices of children and mothers
- Food habits, customs, beliefs, traditions, food taboos
- Primary health care services
- Feeding programmes (ICDS, mid-day meal)
- Immunization programmes
- Parasitic, bacterial, viral infections → precipitate malnutrition
- Diarrhoea, measles, TB, whooping cough, malaria, intestinal parasites
- Vicious circle: Infection → malnutrition → worse infection
NUTRITIONAL SURVEILLANCE (Park - Important Concept)
- Aid long-term planning in health and development
- Provide input for programme management and evaluation
- Give timely warning and intervention to prevent short-term food consumption crises
SUMMARY TABLE - All Methods at a Glance
| Method | What It Detects | Stage of Disease |
|---|---|---|
| Food balance sheets & dietary surveys | Food gap, inadequacy | Prepathogenic |
| Biochemical tests | Diminishing reserves, subclinical deficiency | Pre-pathogenic / Early pathogenic |
| Anthropometry | Chronic/acute malnutrition (stunting/wasting) | Pathogenic |
| Functional indicators | Immune dysfunction, work capacity loss | Pathogenic |
| Clinical examination | Overt clinical signs | Post-clinical horizon |
| Vital statistics (mortality data) | Deaths due to malnutrition | End stage |
Key Exam Points:
- 7 methods of nutritional assessment: Clinical, Anthropometry, Biochemical, Functional, Dietary, Vital statistics, Ecological
- Most important lab test = Haemoglobin estimation
- Biochemical tests are done on a subsample (too expensive for whole community)
- Dietary survey in India uses weighment of raw foods (most commonly) with 7-day dietary cycle
- Nutritive Value of Indian Foods - ICMR publication used for dietary data analysis
- Mortality in 1-4 year age group is most closely linked to malnutrition in developing countries
- Ecological "ecological diagnosis" must be made before planning prevention/control
See mention the tables which are in the park textbook give that u don't make extra tables u give points wise answer make some tables where they are necessary
- Points/bullets for most content
- Tables only from Park's textbook (Table 33, Table 34, etc.) - reproduced as-is
- No extra self-made tables unless comparing 2-3 things where a table is genuinely necessary
- Clean, exam-ready, point-wise answers
NUTRITIONAL ASSESSMENT IN A COMMUNITY
(As per Park's Textbook of PSM)
DEFINITION
- Nutritional status of an individual is often the result of many interrelated factors
- It is influenced by adequacy of food intake (quantity + quality) and physical health of the individual
- Nutritional status of a community = sum of the nutritional status of all individuals forming that community
OBJECTIVES OF NUTRITIONAL SURVEY
- To obtain precise information on the prevalence and geographic distribution of nutritional problems of a given community
- To identify individuals or population groups "at risk" or in greatest need of assistance
- Without this information, problems cannot be defined and policies cannot be formulated
- To develop a health care programme that meets the needs defined by assessment
- To evaluate the effectiveness of such programmes
PLANNING THE SURVEY
- Examination of a random and representative sample of the population is sufficient (need not examine all persons)
- Sample must cover:
- All age groups
- Both sexes
- Different socio-economic groups
- All surveys should be planned with expert statistical advice
- Decisions to be made in advance:
- Duration of survey
- Type of survey - cross-sectional or longitudinal
- Standardization of measurement techniques and survey instruments
- Opportunity may be taken to conduct an intensive investigation on a sub-sample
ASSESSMENT METHODS
DIAGRAM: Methods of Nutritional Assessment & Natural History of Disease (Park's Fig. 5)
- Clinical examination
- Anthropometry
- Biochemical evaluation
- Functional assessment
- Assessment of dietary intake
- Vital and health statistics
- Ecological studies
1. CLINICAL EXAMINATION
- Essential feature of all nutritional surveys
- Simplest and most practical method of ascertaining nutritional status of a group
- There are a number of physical signs - some specific, many non-specific - known to be associated with malnutrition
- When two or more clinical signs characteristic of a deficiency disease are present simultaneously, their diagnostic significance is greatly enhanced
- (a) Not related to nutrition - e.g., alopecia, pyorrhoea, pterygium
- (b) Need further investigation - e.g., malar pigmentation, corneal vascularization, geographic tongue
- (c) Known to be of value - e.g., angular stomatitis, Bitot's spots, calf tenderness, absence of knee or ankle jerks (beri-beri), enlargement of thyroid gland (endemic goitre)
- (a) Malnutrition cannot be quantified on the basis of clinical signs
- (b) Many deficiencies are unaccompanied by physical signs
- (c) Lack of specificity and subjective nature of most physical signs
- To minimize errors, standard survey forms/schedules covering all areas of the body have been devised (Annexure I - specimen nutrition assessment schedule)
2. ANTHROPOMETRY
- Anthropometric measurements such as height, weight, skinfold thickness and arm circumference are valuable indicators of nutritional status
- In young children, additional measurements such as head and chest circumference are made
- If recorded over a period of time, they reflect patterns of growth and development, and how individuals deviate from the average at various ages in body size, build and nutritional status
- Anthropometric data can be collected by non-medical personnel, given sufficient training
3. LABORATORY AND BIOCHEMICAL ASSESSMENT
- (i) Haemoglobin estimation - most important laboratory test carried out in nutrition surveys; Hb level is a useful index of overall state of nutrition irrespective of its significance in anaemia; RBC count and haematocrit are also valuable
- (ii) Stools and urine - Stools should be examined for intestinal parasites; history of parasitic infestation, chronic dysentery and diarrhoea provides useful background information; Urine should be examined for albumin and sugar
- With increasing knowledge of metabolic functions of vitamins and minerals, assessment has given way to more precise biochemical tests
- Applied to measure:
- Individual nutrient concentration in body fluids (e.g., serum retinol, serum iron)
- Detection of abnormal amounts of metabolites in urine (e.g., urinary iodine) - frequently after a loading dose
- Measurement of enzymes in which the vitamin is a known co-factor (e.g., in riboflavin deficiency)
- Help establish malnutrition in its preclinical stages
- Time-consuming and expensive
- Cannot be applied on a large scale to a whole community
- Often carried out only on a subsample of the population
- Most biochemical tests reveal only current nutritional status
- Useful to quantify mild deficiencies
- If clinical examination has raised a question, biochemical tests may be invoked to prove or disprove it
PARK'S TABLE 33 - Some Biochemical Tests Used in Nutrition Surveys
| Nutrient | Method | Normal Value |
|---|---|---|
| Vitamin A | Serum retinol | 20 mcg/dL |
| Thiamine | TPP stimulation of RBC transketolase activity | 1.00 - 1.23 (ratio) |
| Riboflavin | RBC glutathione reductase stimulated by FAD | 1.0 - 1.2 (ratio) |
| Niacin | Urine N-methyl nicotinamide | (not very reliable) |
| Folate | Serum folate | 6.0 mcg/mL |
| Red cell folate | 160 mcg/mL | |
| Vitamin B12 | Serum vitamin B12 concentration | 160 mg/L |
| Vitamin C | Leucocyte ascorbic acid | 15 mcg/10⁹ cells |
| Vitamin K | Prothrombin time | 11 - 16 seconds |
| Protein | Serum albumin | 35 g/L |
| Transferrin | 20 g/L | |
| Thyroid-binding pre-albumin | 250 mg/L |
4. FUNCTIONAL INDICATORS
- Static indices (biochemical indicators) will continue to play an important role as they are well-established and familiar to practitioners and public health workers
- Functional indices are emerging as an important class of diagnostic tools
PARK'S TABLE 34 - Functional Indices of Nutritional Status
| System | Test | Nutrient |
|---|---|---|
| Structural integrity | Erythrocyte fragility | Vit E, Se |
| Capillary fragility | Vit C | |
| Tensile strength | Cu | |
| Host defence | Leucocyte chemotaxis | P/E, Zn |
| Leucocyte phagocytic capacity | P/E, Fe | |
| Leucocyte bactericidal capacity | P/E, Fe, Se | |
| T cell blastogenesis | P/E, Zn | |
| Delayed cutaneous hypersensitivity | P/E, Zn | |
| Haemostasis | Prothrombin time | Vit K |
| Reproduction | Sperm count | Energy, Zn |
| Nerve function | Nerve conduction | P/E, Vit B1, B12 |
| Dark adaptation | Vit A, Zn | |
| EEG | P/E | |
| Work capacity | Heart rate | P/E, Fe |
| Vasopressor response | Vit C |
5. ASSESSMENT OF DIETARY INTAKE
- Value of nutritional assessment is greatly enhanced when supplemented by assessment of food consumption
- Direct assessment of food consumption involves dietary surveys - household inquiries or individual food consumption surveys
- (i) Weighment of Raw Foods - widely employed in India; survey team visits households and weighs all food going to be cooked and eaten as well as food wasted or discarded; duration may vary from 1 to 21 days, commonly 7 days ("one dietary cycle"); considered fairly accurate
- (ii) Weighment of Cooked Foods - foods analyzed in the state in which they are normally consumed; not easily acceptable among people
- (iii) Oral Questionnaire Method - useful for large numbers of people in a short time; retrospective inquiry about nature and quantity of food eaten in previous 24 or 48 hours; if properly carried out, gives reliable results
- (a) Mean intake (grams) of food in terms of cereals, pulses, etc.
- (b) Nutritive value (energy, proteins, fats, minerals, vitamins) using ICMR's "Nutritive Value of Indian Foods" publication
- Comparison with RDA to assess adequacy
- Provides information about dietary intake patterns, specific foods consumed and estimated nutrient intakes
- Indicates relative dietary inadequacies as judged by present standards
- Valuable for planning health education activities
- Allows assessment of changes needed in agriculture and food production industries
6. VITAL STATISTICS
- Analysis of vital statistics - mortality and morbidity data - will identify groups at high risk and indicate the extent of risk to the community
- Mortality in age group 1 to 4 years is particularly related to malnutrition; in developing countries it may be as much as 20 times that in countries such as Australia, Denmark or France
- Infant mortality rate
- Second-year mortality rate
- Rate of low birth-weight babies
- Life expectancy
- Protein energy malnutrition
- Anaemia
- Xerophthalmia and other vitamin deficiencies
- Endemic goitre
- Diarrhoea, measles, parasitic infestations
Limitation: Mortality data do not provide a satisfactory picture of nutritional status of a population
7. ASSESSMENT OF ECOLOGICAL FACTORS
- Malnutrition is the end result of many interacting ecological factors
- In any nutrition survey it is necessary to collect ecological information of the given community to make the assessment complete
- An "ecological diagnosis" of various factors influencing nutrition in the community must be made before measures for prevention and control can be put into effect
- (a) Food Balance Sheet - indirect method of assessing food consumption; supplies related to census population to derive levels of food consumption in terms of per capita supply availability; refers to country as a whole (conceals differences between regions and economic/age/sex groups); advantage - cheaper and simpler than any direct assessment method; gives indication of general pattern of food consumption in the country
- (b) Socio-economic Factors - food consumption patterns vary among various socio-economic groups; family size, occupation, income, education, customs, cultural patterns in relation to feeding practices of children and mothers - all influence food consumption patterns
- (c) Health and Educational Services - primary health care services, feeding and immunization programmes should also be taken into consideration
- (d) Conditioning Influences - parasitic, bacterial and viral infections which precipitate malnutrition
NUTRITIONAL SURVEILLANCE (Park - Key Concept)
- (a) To aid long-term planning in health and development
- (b) To provide input for programme management and evaluation
- (c) To give timely warning and intervention to prevent short-term food consumption crises
HIGH-YIELD POINTS FOR EXAM
- 7 methods of nutritional assessment - CABFVED (Clinical, Anthropometry, Biochemical, Functional, Vital statistics, Ecological, Dietary)
- Most important lab test in nutrition survey = Haemoglobin estimation
- Biochemical tests are done on a subsample (expensive; cannot do on whole community)
- Dietary survey in India = Weighment of raw foods, duration = 7-day dietary cycle
- Reference for dietary data in India = ICMR "Nutritive Value of Indian Foods"
- Mortality in 1-4 year age group is most closely linked to malnutrition
- Mortality data alone is not satisfactory for assessing nutritional status
- Always make an ecological diagnosis before planning prevention/control
Convert this answer into 6-8 marks
NUTRITIONAL ASSESSMENT IN A COMMUNITY
(6-8 Marks | As per Park's PSM)
DEFINITION
- Nutritional status of a community = sum of the nutritional status of all individuals forming that community
- The main objective of a nutritional survey is to obtain precise information on prevalence and geographic distribution of nutritional problems, identify groups "at risk", and develop/evaluate health care programmes
PLANNING
- Examine a random and representative sample covering all ages, both sexes, different socio-economic groups
- Decide in advance: duration, type (cross-sectional/longitudinal), standardization of techniques
- All surveys planned with expert statistical advice
ASSESSMENT METHODS
1. Clinical Examination
- Simplest and most practical method
- Look for physical signs of nutritional deficiency using standard survey forms (Annexure I)
- WHO classified signs into 3 categories:
- Not related to nutrition - alopecia, pyorrhoea, pterygium
- Need further investigation - malar pigmentation, corneal vascularization
- Known to be of value - angular stomatitis, Bitot's spots, absent knee/ankle jerks (beri-beri), goitre
- Drawbacks: Cannot quantify malnutrition; many deficiencies have no physical signs; lacks specificity
2. Anthropometry
- Height, weight, skinfold thickness, arm circumference
- In young children - head and chest circumference additionally
- Can be collected by non-medical personnel with training
- Reflects patterns of growth and development over time
3. Biochemical Evaluation
- (i) Lab tests - Hb estimation (most important), RBC count, haematocrit; stool for parasites; urine for albumin and sugar
- (ii) Biochemical tests - Serum retinol (Vit A), urinary iodine, serum iron - detect malnutrition in preclinical stages
- Limitations: Time-consuming, expensive; done only on a subsample; reveals only current status
4. Functional Indicators
- Emerging as important diagnostic tools alongside static biochemical indices
- Examples (Park's Table 34): Delayed cutaneous hypersensitivity (P/E, Zn); Dark adaptation (Vit A, Zn); Nerve conduction (Vit B1, B12); Work capacity/Heart rate (P/E, Fe)
5. Assessment of Dietary Intake
- Methods of dietary survey:
- Weighment of raw foods - widely used in India; 7-day dietary cycle; fairly accurate
- Weighment of cooked foods - accurate but not easily acceptable
- Oral questionnaire (24-hr recall) - useful for large populations; quick
- Data translated using ICMR's "Nutritive Value of Indian Foods" and compared with RDA
6. Vital Statistics
- Mortality and morbidity data identify high-risk groups
- Mortality in 1-4 year age group is most related to malnutrition
- Other indicators: IMR, second-year mortality rate, rate of LBW babies, life expectancy
- Limitation: Mortality data alone is not a satisfactory picture of nutritional status
7. Ecological Studies
- Malnutrition is the end result of many interacting ecological factors
- Components:
- (a) Food Balance Sheet - indirect method; per capita food availability; cheaper and simpler than direct methods
- (b) Socio-economic factors - income, occupation, family size, education, food habits
- (c) Health and educational services - PHC, feeding programmes, immunization
- (d) Conditioning influences - infections (diarrhoea, TB, parasites) that precipitate malnutrition
- An "ecological diagnosis" must be made before planning prevention and control
KEY POINTS
- 7 methods - C A B F D V E (Clinical, Anthropometry, Biochemical, Functional, Dietary, Vital statistics, Ecological)
- Most important lab test = Haemoglobin estimation
- Most common dietary survey method in India = Weighment of raw foods (7-day cycle)
- Biochemical tests done on subsample only
Enumerate the major nutritional problems of india Define malnutrition Pem-risk factors and cause -classification - prevention and control to reduce pem in india "Long note "
NUTRITIONAL PROBLEMS OF INDIA, MALNUTRITION & PEM
(Long Note | As per Park's PSM)
I. ENUMERATE MAJOR NUTRITIONAL PROBLEMS OF INDIA
"From the nutritional point of view, the Indian society is a dual society - a small group of well fed and a very large group of undernourished." - Park
- Insufficiency of food - the "food gap" - is the chief cause
- Major health problem particularly in the first years of life
- About 80% are mild and moderate cases
- Incidence of severe cases is 1-2% in preschool age children
- Nutritional marasmus is more frequent than kwashiorkor in India
- India has probably the highest prevalence of nutritional anaemia in women and children
- About one-half of non-pregnant women and young children suffer from anaemia
- 50.3% of pregnant women are anaemic
- 19% of maternal deaths are attributed to anaemia
- According to NFHS-4: 53.1% women are anaemic; anaemia in children aged 6-59 months is 58.4%
- Most common cause: Iron deficiency; less frequently folate and Vitamin B12 deficiency
- About 28% of babies born in India are LBW (<2.5 kg)
- Maternal malnutrition and anaemia are mainly responsible
- According to NFHS-4: 18.5% children are born with LBW
- About 0.04% of total blindness in India attributed to Vitamin A deficiency
- Keratomalacia is the major cause of nutritional blindness in children usually between 1-3 years of age
- Subclinical deficiency of Vitamin A is widespread - associated with increased morbidity and mortality from respiratory and GI infections
- Goitre and IDD highly endemic in sub-Himalayan regions
- Problem is not restricted to the "goitre belt" - also prevalent in other parts of India
- 263 out of 324 districts surveyed in 29 states and all UTs are endemic (prevalence >10%)
- More than 71 million people are suffering from goitre and other IDD
- Lathyrism and endemic fluorosis in certain parts of the country
- Widespread adulteration of foodstuffs
II. DEFINITION OF MALNUTRITION
- The word "malnutrition" literally means "bad nutrition"
- It includes both undernutrition (deficiency of calories, protein, vitamins, minerals) and overnutrition (excess intake)
- WHO definition: "A pathological state resulting from a relative or absolute deficiency or excess of one or more essential nutrients"
- Malnutrition is said to be a "man-made disease" - it is a disease of human societies. It begins quite commonly in the womb and ends in the grave
- (a) Protein-Energy Malnutrition - deficiency of proteins and calories
- (b) Micronutrient malnutrition - deficiency of essential vitamins and minerals such as Vitamin A, calcium, iodine, iron and zinc; estimated ~2 billion people affected worldwide
- (c) Overnutrition - excess intake leading to obesity, diabetes, hypertension, cardiovascular disease
- Stunting - chronic malnutrition (low height-for-age)
- Wasting - acute malnutrition (low weight-for-height)
- Underweight - composite measure (low weight-for-age)
III. PROTEIN ENERGY MALNUTRITION (PEM)
- PEM has been identified as a major health and nutrition problem in India
- It occurs particularly in weaklings and children in the first years of life
- Characterized by: low birth weight (if mother malnourished), poor growth in children, high level of mortality in children between 12 and 24 months
- Estimated to be an underlying cause in 30% of deaths among children under age 5
A. RISK FACTORS AND CAUSES OF PEM
- In the 1970s it was widely held that PEM was due to protein deficiency ("protein gap")
- Over the years, the concept of "protein gap" has given place to "food gap"
- PEM is primarily due to:
- (a) Inadequate intake of food - both in quantity and quality
- (b) Infections - notably diarrhoea, respiratory infections, measles and intestinal worms which:
- Increase requirements for calories, protein and other nutrients
- Decrease their absorption and utilization
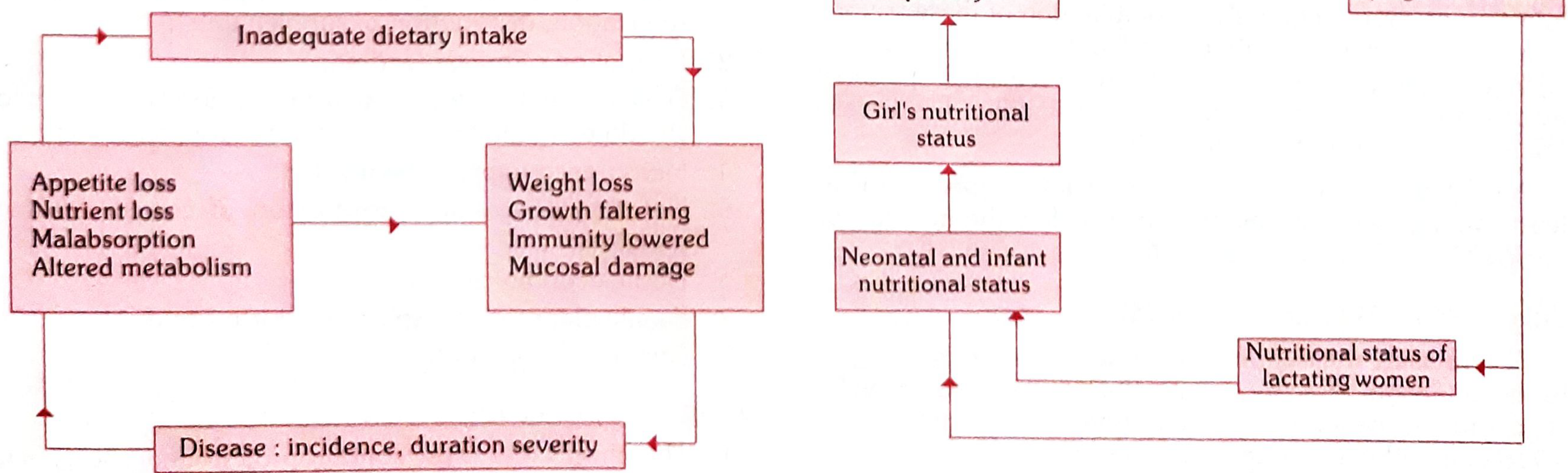
Infection contributes to malnutrition and malnutrition contributes to infection - both acting synergistically
- Poor environmental conditions
- Large family size
- Poor maternal health
- Failure of lactation
- Premature termination of breast-feeding
- Adverse cultural practices relating to child rearing and weaning:
- Use of over-diluted cow's milk
- Discarding cooking water from cereals
- Delayed supplementary feeding
- A child's nutritional status depends on past nutritional history
- This nutritional history is linked to the mother's health and nutritional status
- Which in turn was influenced by her own childhood living conditions and nutritional history
- Thus malnutrition is intergenerational
B. CLASSIFICATION OF PEM
| Condition | Index Used | Definition |
|---|---|---|
| Underweight | Weight-for-Age | WFA Z-score < -2SD below WHO median; composite of stunting + wasting |
| Stunting | Height/Length-for-Age | HFA Z-score < -2SD; reflects chronic malnutrition |
| Wasting | Weight-for-Height | WFH Z-score < -2SD; reflects acute malnutrition |
- Each indicator expressed in Z-scores (SD units) from the median of the reference population
- Further classified as moderate (-2SD to -3SD) or severe (< -3SD)
- Develops in individuals on diets with low protein/energy ratio
- Main symptoms:
- Oedema (pitting)
- Wasting
- Liver enlargement (hepatomegaly)
- Hypoalbuminaemia
- Steatosis (fatty liver)
- Depigmentation of skin and hair (flag sign)
- Caused by inadequate intake of both protein and energy
- Form of severe cachexia with weight loss - wasting in infancy and childhood
- Main symptoms:
- Severe wasting (baggy pants appearance)
- Little or no oedema
- Minimal subcutaneous fat
- Severe muscle wasting
- Non-normal serum albumin levels
In India: Marasmus > Kwashiorkor in frequency
- First indicator of PEM = underweight for age
- Most practical method = Growth charts (can be employed by field health workers)
- Growth charts indicate at a glance whether the child is gaining or losing weight
| MUAC | Interpretation |
|---|---|
| > 13.5 cm | Satisfactory nutritional status |
| 12.5 - 13.5 cm | Mild-moderate malnutrition |
| < 12.5 cm | Severe malnutrition |
- Cannot be used before 1 year of age
- Between ages 1 to 5 years - hardly varies, making it a reliable screening tool
C. PREVENTION AND CONTROL OF PEM IN INDIA
"There is no simple solution to the problem of PEM. Many types of actions are necessary."
- Measures directed to pregnant and lactating women - education, distribution of supplements
- Promotion of breast-feeding
- Development of low cost weaning foods - child should eat more food at frequent intervals
- Measures to improve family diet
- Nutrition education - promotion of correct feeding practices
- Home economics
- Family planning and spacing of births
- Improvement of family environment
- Child's diet must contain protein and energy-rich foods - milk, eggs, fresh fruits should be given if possible
- Immunization - to prevent infections that trigger PEM
- Food fortification
- Periodic surveillance - growth monitoring
- Early diagnosis of any lag in growth
- Early diagnosis and treatment of infections and diarrhoea
- Development of programmes for early rehydration of children with diarrhoea
- Development of supplementary feeding programmes during epidemics
- Deworming of heavily infested children
- Nutritional rehabilitation services (NRC - Nutritional Rehabilitation Centres under NHM)
- Hospital treatment
- Follow-up care
National Programmes Addressing PEM in India:
- ICDS (Integrated Child Development Services) - supplementary nutrition, immunization, health check-up, nutrition education for children <6 years and pregnant/lactating women
- Mid-Day Meal Scheme - school children
- Pradhan Mantri Matru Vandana Yojana - maternity benefit scheme
- National Nutrition Mission (POSHAN Abhiyaan) - launched 2018, target to reduce stunting and undernutrition
- Janani Suraksha Yojana - promoting institutional delivery, addressing LBW
- NRC (Nutritional Rehabilitation Centres) - management of Severe Acute Malnutrition (SAM)
HIGH-YIELD EXAM POINTS:
- PEM = underlying cause in 30% of under-5 deaths
- Concept shifted from "protein gap" to "food gap" - primary cause is inadequate food intake + infections
- Marasmus > Kwashiorkor in India
- First indicator of PEM = underweight for age; detected by growth charts
- MUAC < 12.5 cm = severe malnutrition
- Kwashiorkor = low protein/energy ratio diet; oedema present
- Marasmus = both protein + energy deficient; no oedema, severe wasting
- Prevention follows Leavell & Clark's levels - health promotion, specific protection, early diagnosis, rehabilitation
Add More points to answer acc to park
NUTRITIONAL PROBLEMS OF INDIA, MALNUTRITION & PEM
(Long Note | As per Park's PSM - Updated with More Points)
I. MAJOR NUTRITIONAL PROBLEMS OF INDIA
"There are many nutritional problems which affect vast segments of our population." - Park
- Insufficiency of food - the "food gap" - is the chief cause
- Major health problem particularly in the first years of life
- About 80% are mild and moderate cases
- Incidence of severe cases is 1-2% in preschool age children
- Nutritional marasmus is more frequent than kwashiorkor in India
- PEM is an underlying cause in 30% of deaths among children under age 5
- As many as 27% of children in low income countries have stunting; 17% have low weight for height
- India has probably the highest prevalence of nutritional anaemia in women and children
- About one-half of non-pregnant women and young children suffer from anaemia
- 50.3% of pregnant women are anaemic
- 19% of maternal deaths are attributed to anaemia
- NFHS-4: 53.1% women are anaemic; children aged 6-59 months: 58.4% anaemic
- Most common cause: iron deficiency; less frequently folate and Vitamin B12 deficiency
- Even mild anaemia reduces resistance to fatigue; profound effect on psychological and physical behaviour
- LBW = birth weight less than 2500 g
- According to Rapid Survey Report on Children 2014: 18.6% of babies born in India are LBW
- Compared to only 4% in some developed countries
- In countries with high LBW proportion - majority have foetal growth retardation
- Significant risk factors: maternal malnutrition and anaemia
- Other causes: hard physical labour during pregnancy, infections, short maternal stature, very young age, high parity, smoking, close birth intervals
- Problem is multifactorial - no universal solution; interventions have to be cause-specific
- 0.04% of total blindness in India attributed to Vitamin A deficiency
- Keratomalacia is the major cause of nutritional blindness in children 1-3 years
- Most common in children 1-3 years, often related to weaning; younger the child, more severe the disease
- Often associated with PEM; mortality is high in this age group
- Victims belong to the poorest families
- States badly affected: Andhra Pradesh, Tamil Nadu, Karnataka, Bihar, West Bengal (predominantly rice-eating states; rice is devoid of carotene)
- North Indian states have relatively fewer cases
- Only 21% of children aged 12-35 months receive a Vitamin A dose (coverage is very low)
- An estimated 5.7% children in India suffer from eye signs of VAD
- In 1970, National Programme for Prevention of Nutritional Blindness was initiated; modified in 1992; now part of NRHM/RCH programme
- Highly endemic in sub-Himalayan regions (the "goitre belt")
- Problem is NOT restricted to the goitre belt - also found in other parts of India
- Out of 324 districts surveyed in 29 states and all UTs, 263 districts are endemic (prevalence >10%)
- More than 71 million people suffering from goitre and other IDD
- IDD globally affects 1.5 billion people living in iodine-deficient environments
- At least 30,000 babies are stillborn each year due to iodine deficiency; over 120,000 born mentally retarded, physically stunted, deaf-mute or paralysed
- Lathyrism and endemic fluorosis in certain parts of the country
- Widespread adulteration of foodstuffs
II. DEFINITION OF MALNUTRITION
"A pathological state resulting from a relative or absolute deficiency or excess of one or more essential nutrients"
- Malnutrition literally means "bad nutrition"
- Malnutrition is a "man-made disease" - a disease of human societies; begins commonly in the womb and ends in the grave
- Nutritional deficiencies not only lead to severe illnesses requiring long and costly treatment, but also influence physical development, psychic behaviour and susceptibility to infection
- (a) Protein-Energy Malnutrition - deficiency of proteins and calories
- (b) Micronutrient malnutrition - deficiency of Vitamin A, calcium, iodine, iron, zinc; estimated ~2 billion people affected worldwide
- Vitamin A deficiency - most common cause of preventable childhood blindness worldwide
- Iodine deficiency - causes goitre, cretinism and brain damage
- Anaemia - results from insufficient iron intake
- (c) Overnutrition - excess intake; leads to obesity, diabetes, hypertension, cardiovascular disease, liver and gall bladder disorders (diseases of affluence)
- Stunting - chronic malnutrition (low height-for-age)
- Wasting - acute malnutrition (low weight-for-height)
- Underweight - composite measure (low weight-for-age)
III. PROTEIN ENERGY MALNUTRITION (PEM)
- PEM is a major health and nutrition problem in India
- Occurs particularly in weaklings and children in the first years of life
- Characterized by:
- Low birth weight (if mother is malnourished)
- Poor growth in children
- High level of mortality in children between 12-24 months
- Estimated to be an underlying cause in 30% of deaths among children under age 5
- NFHS-4: 35.7% children are underweight, 38.4% are stunted, 21% are wasted
A. RISK FACTORS AND CAUSES OF PEM
- In the 1970s: PEM was thought to be due to "protein gap" (protein deficiency)
- Over the years: concept of "protein gap" has given place to concept of "food gap"
- PEM is primarily due to:
- (a) Inadequate intake of food - both in quantity and quality (food gap)
- (b) Infections - notably diarrhoea, respiratory infections, measles and intestinal worms, which:
- Increase requirements for calories, protein and other nutrients
- Decrease their absorption and utilization
Infection contributes to malnutrition and malnutrition contributes to infection - both acting synergistically - it is a vicious circle
- Poor environmental conditions
- Large family size
- Poor maternal health
- Failure of lactation
- Premature termination of breast-feeding
- Adverse cultural practices:
- Use of over-diluted cow's milk
- Discarding cooking water from cereals
- Delayed supplementary feeding
- A child's nutritional status at any point of time depends on past nutritional history
- This history is linked to the mother's health and nutritional status
- Which in turn was influenced by her own childhood living conditions and nutritional history
- Thus malnutrition perpetuates from generation to generation (Park's Fig. 3)
B. CLASSIFICATION OF PEM
1. Based on Anthropometric Indices (Z-scores / WHO)
| Condition | Index Used | Definition | Type |
|---|---|---|---|
| Underweight | Weight-for-Age (WFA) | Z-score < -2SD | Composite of stunting + wasting |
| Stunting | Height-for-Age (HFA) | Z-score < -2SD | Chronic malnutrition (past) |
| Wasting | Weight-for-Height (WFH) | Z-score < -2SD | Acute malnutrition (current) |
- Moderate: Z-score between -2SD and -3SD
- Severe: Z-score below -3SD
Key Details on Each Type:
- Recommended indicator to assess changes in magnitude of malnutrition over time
- Can result from either chronic or acute malnutrition, or both
- Even mildly underweight children have increased mortality risk
- Severely underweight children are at even greater risk
- Failure to achieve expected height/length compared to healthy well-nourished children of same age
- Indicator of past growth failure (linear growth retardation)
- Results from: chronic insufficient nutrient intake, frequent infections, sustained inappropriate feeding practices, poverty
- Associated with delayed psycho-social and cognitive development and poor school performance
- Can be exacerbated by recurrent and chronic illness
- Represents a recent (current) failure to receive adequate nutrition
- Very sensitive to - changes in food availability or disease prevalence
- Shows marked seasonal patterns
- Causes: inadequate food intake, incorrect feeding practices, disease, infection - frequently a combination
2. Severe Acute Malnutrition (SAM)
- Very low weight-for-height/length (Z-score below -3SD)
- OR mid-upper arm circumference (MUAC) < 115 mm (< 11.5 cm)
- OR presence of nutritional oedema
- SAM significantly increases risk of death in children under 5 years
- Can indirectly cause death by increasing case fatality rate in children with diarrhoea and pneumonia
- Children who are severely wasted are 9 times likely to die than well-nourished children
3. Clinical Forms of Severe PEM
- Develops on diets with low protein/energy ratio
- Features:
- Oedema (pitting)
- Wasting
- Liver enlargement (hepatomegaly)
- Hypoalbuminaemia
- Steatosis (fatty liver)
- Depigmentation of skin and hair (flag sign)
- Misery and apathy
- Caused by inadequate intake of both protein and energy
- Severe cachexia with weight loss - wasting in infancy and childhood
- Features:
- Severe wasting ("old man" appearance; "baggy pants")
- Little or no oedema
- Minimal subcutaneous fat
- Severe muscle wasting
- Non-normal serum albumin
In India: Marasmus > Kwashiorkor in frequency
4. Early Detection of PEM
- First indicator of PEM = underweight for age
- Most practical method detectable even by field health workers = Growth charts
- Growth charts indicate at a glance whether child is gaining or losing weight
- Arm circumference yields reliable estimation of the body's muscle mass
- Reduction of muscle mass is one of the most striking mechanisms by which the body adjusts to inadequate energy intake
- Cannot be used before 1 year of age
- Between ages 1-5 years - hardly varies (reliable screening tool)
| MUAC | Status |
|---|---|
| > 13.5 cm | Satisfactory nutritional status |
| 12.5 - 13.5 cm | Mild-moderate malnutrition |
| < 12.5 cm | Severe malnutrition |
C. PREVENTION AND CONTROL OF PEM IN INDIA
"There is no simple solution to the problem of PEM. Many types of actions are necessary."
- Measures directed to pregnant and lactating women - education, distribution of supplements
- Promotion of breast-feeding
- Development of low-cost weaning foods - child should eat more food at frequent intervals
- Measures to improve family diet
- Nutrition education - promotion of correct feeding practices
- Home economics
- Family planning and spacing of births
- Improvement of family environment
- Child's diet must contain protein and energy-rich foods - milk, eggs, fresh fruits if possible
- Immunization - to prevent infections that trigger and worsen PEM
- Food fortification
- Periodic surveillance - regular growth monitoring
- Early diagnosis of any lag in growth
- Early diagnosis and treatment of infections and diarrhoea
- Development of programmes for early rehydration of children with diarrhoea
- Development of supplementary feeding programmes during epidemics
- Deworming of heavily infested children
- Nutritional rehabilitation services (NRC)
- Hospital treatment
- Follow-up care
- ICDS - supplementary nutrition, immunization, health check-up, referral services, nutrition education for children <6 years + pregnant/lactating women
- Mid-Day Meal Scheme - school children
- POSHAN Abhiyaan (National Nutrition Mission) - launched 2018; target to reduce stunting, undernutrition, anaemia and LBW
- NRC (Nutritional Rehabilitation Centres) under NHM - management of Severe Acute Malnutrition (SAM)
- Pradhan Mantri Matru Vandana Yojana - maternity benefit
- Janani Suraksha Yojana - institutional delivery, addressing LBW
HIGH-YIELD EXAM POINTS
- Primary cause of PEM = Food gap (not protein gap - concept changed in 1970s)
- PEM = underlying cause of 30% under-5 deaths
- SAM defined by MUAC < 115 mm OR Z-score < -3SD OR nutritional oedema
- Severely wasted children = 9 times more likely to die
- Marasmus > Kwashiorkor in India
- Kwashiorkor = oedema present; Marasmus = no oedema, severe wasting
- MUAC < 12.5 cm = severe malnutrition; only valid 1-5 years of age
- First indicator of PEM = underweight for age, detected by growth charts
- Stunting = past failure; Wasting = current/acute failure
- Malnutrition is intergenerational - perpetuates from mother to child