Pathophysiology of persistent pulmonary hypertension in paediatrics and newborn. Its management course
Reading File
Finding Sources
Finding Sources
Searching PubMed
"persistent pulmonary hypertension" newborn pathophysiology management
Reading File
Reading File
Reading File
Searching PubMed
"persistent pulmonary hypertension" newborn PPHN treatment
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from multiple authoritative sources. Let me compile the full answer.
Persistent Pulmonary Hypertension of the Newborn (PPHN)
Overview
PPHN (also called "persistent fetal circulation") is one of the main causes of neonatal morbidity and mortality, with an incidence of approximately 2 per 1,000 live births in term and late preterm infants. It results from failure of the normal cardiopulmonary transition at birth, with persistence of high pulmonary vascular resistance (PVR) leading to right-to-left shunting and severe hypoxemia.
- Creasy & Resnik's Maternal-Fetal Medicine, p. 1790
- Harriet Lane Handbook, 23rd ed., p. 651
Normal Fetal-to-Neonatal Transition (Background)
In fetal life, the pulmonary circulation carries only ~8-10% of cardiac output. Pulmonary vascular resistance is kept high (and intentionally so) by:
- Low fetal PaO2 (hypoxic pulmonary vasoconstriction)
- High circulating vasoconstrictors (endothelin-1, thromboxane)
- Anatomic factors (thick-walled, reactive pulmonary arterioles)
At birth, a coordinated cascade normally reduces PVR 8- to 10-fold:
- Lung expansion increases alveolar and arterial oxygen tension - a potent vasodilatory stimulus
- Ventilation increases pH, reducing acidosis-driven vasoconstriction
- Nitric oxide (NO) and prostacyclin are released from vascular endothelium, causing smooth muscle relaxation
- Rising left atrial pressure functionally closes the foramen ovale
- Rising arterial oxygen tension and local mediators (bradykinin, acetylcholine, prostaglandins) cause the ductus arteriosus to contract and close
Failure at any step leads to PPHN.
- Morgan & Mikhail's Clinical Anesthesiology, 7th ed., p. 1596
- Miller's Anesthesia, 10th ed., p. 11309
Pathophysiology
The Core Cycle
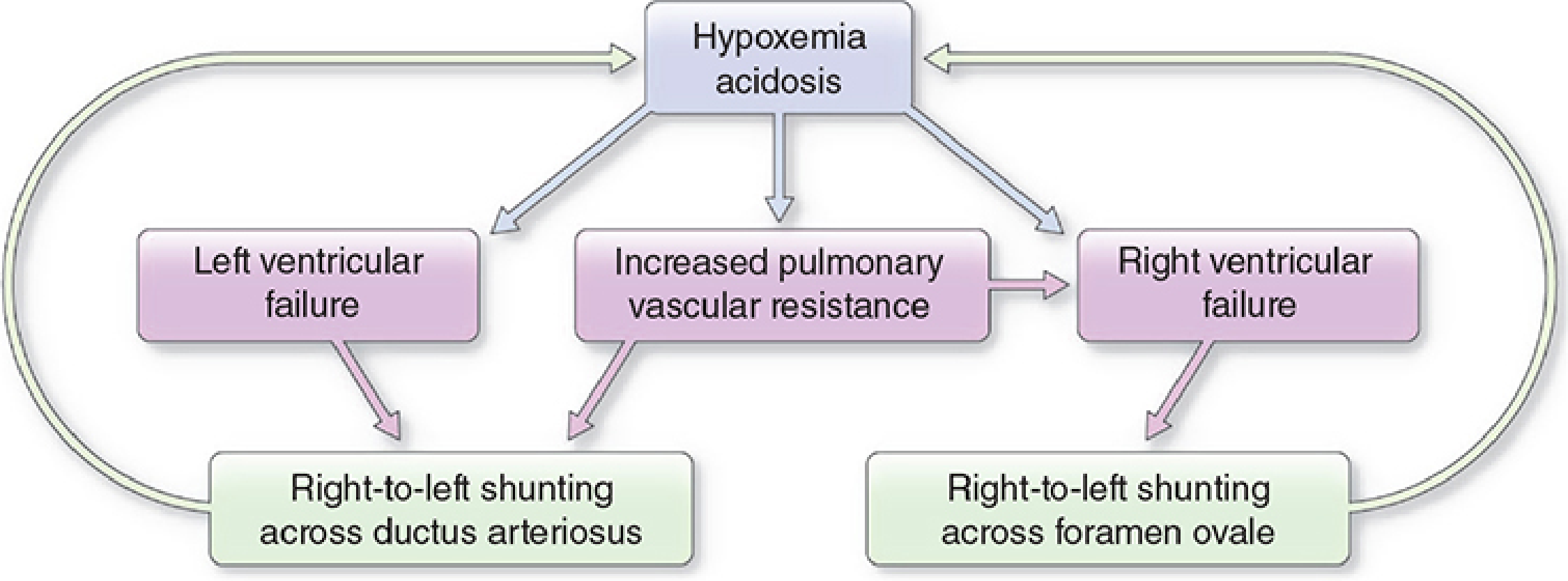
Figure: Pathophysiology of PPHN (persistent fetal circulation). Hypoxemia and acidosis drive increased PVR, causing both right and left ventricular failure, which leads to right-to-left shunting across the ductus arteriosus and foramen ovale - feeding more hypoxemia and acidosis in a vicious cycle. - Morgan & Mikhail, p. 1596
When PVR remains elevated or rises postnatally:
- Right ventricular afterload increases - RV pressure can equal or exceed left ventricular pressure
- The foramen ovale and ductus arteriosus remain open (or reopen), permitting right-to-left shunting
- Deoxygenated blood bypasses the pulmonary circulation entirely
- Hypoxemia and acidosis worsen, further driving pulmonary vasoconstriction - a self-reinforcing cycle
Two Underlying Mechanisms
- Pulmonary arteriolar vasoconstriction - functional, reactive, and potentially reversible
- Vascular structural remodeling - muscular hypertrophy of arteriolar walls; less reversible acutely
Etiologic Classification (Four Categories)
| Category | Examples |
|---|---|
| Idiopathic | Abnormally remodeled pulmonary vasculature (no identifiable cause) |
| Lung parenchymal disease | Meconium aspiration syndrome (MAS), pneumonia/sepsis |
| Abnormal birth transition | Transient tachypnea (TTN), RDS, perinatal asphyxia |
| Congenital lung malformation | Congenital diaphragmatic hernia (CDH), pulmonary hypoplasia |
- Creasy & Resnik, p. 1790
Molecular/Mediator Mechanisms
The pulmonary circulation is exquisitely sensitive to:
-
Oxygen - hypoxia causes vasoconstriction via smooth muscle depolarization
-
pH - acidosis amplifies hypoxic vasoconstriction
-
Nitric oxide (NO) - endogenous vasodilator; impaired NO signaling is central to PPHN
-
Endothelin-1 - potent vasoconstrictor, upregulated in PPHN
-
Prostaglandins and prostacyclin - vasodilatory; reduced in PPHN
-
cGMP/cAMP pathways - downstream mediators of pulmonary vasodilation; targeted by pharmacotherapy
-
Barash Clinical Anesthesia, 9th ed., p. 3578
Risk Factors
PPHN is most common in term and post-term newborns, but also affects preterm infants. Risk factors include:
-
Cesarean delivery (no "vaginal squeeze" to clear lung fluid)
-
Fetal distress and low APGAR scores
-
Hypoxemia and acidosis
-
MAS - meconium particles trigger inflammatory vasoconstriction
-
Sepsis/pneumonia - inflammatory mediators
-
CDH or renal agenesis - structural pulmonary hypoplasia
-
Polycythemia/hyperviscosity
-
Maternal SSRI or NSAID use in late pregnancy (NSAIDs cause in utero ductal constriction)
-
Maternal diabetes, maternal asthma, maternal smoking
-
Harriet Lane, p. 651-652; Barash, p. 3578
Diagnosis
PPHN typically presents within 12-24 hours of birth.
Key features:
- Severe hypoxemia (PaO2 <35-45 mmHg in 100% O2) that is disproportionate to radiologic changes
- Pre/postductal oxygenation gradient ≥7-15 mmHg (right hand vs. lower limb SpO2) - confirms right-to-left ductal shunting
- Structurally normal heart on echocardiogram, with R-to-L shunt at foramen ovale and/or ductus arteriosus
- Normal or elevated PaCO2 (unlike primary parenchymal disease)
Critical differential: Cyanotic congenital heart disease must be excluded. If little improvement with 100% O2 (hyperoxia test), perform detailed cardiac exam and echocardiogram.
- Harriet Lane, p. 651
Management
Management is stepwise and targets multiple mechanisms simultaneously.
1. Treat the Underlying Etiology
- Antibiotics for sepsis/pneumonia
- Surfactant for RDS
- Surgical correction for CDH (when stable)
- Correct polycythemia, hypoglycemia
2. Optimize Oxygenation and Ventilation
- Supplemental oxygen to achieve preductal SpO2 91-95% (focus on preductal rather than postductal saturations to reduce lung injury risk)
- Conventional mechanical ventilation targeting:
- PaO2 60-100 mmHg
- Normocapnia (avoid severe hyperventilation - PaCO2 <30 mmHg causes myocardial ischemia and decreased cerebral blood flow, and risks barotrauma)
- High-frequency oscillatory ventilation (HFOV) - considered when conventional ventilation fails; reduces barotrauma
- Optimize oxygen-carrying capacity - blood transfusions if anemia
3. Minimize Pulmonary Vasoconstriction
- Minimal handling; avoid painful/noxious stimuli
- Sedation (morphine, fentanyl, midazolam) - reduces catecholamine surges
- Neuromuscular blockade in ventilated neonates if severe agitation
4. Hemodynamic Support
Maintaining systemic blood pressure is critical - it reverses the R-to-L shunt by raising SVR relative to PVR:
-
Volume expansion (normal saline, packed red cells)
-
Inotropes/vasopressors: dopamine, norepinephrine, vasopressin
-
Dobutamine - provides inotropy and reduces SVR; used cautiously in normotensive patients (risk of worsening R-to-L shunt)
-
Maintenance of right ventricular function is paramount to survival
-
Barash, p. 3579
5. Pulmonary Vasodilator Therapy
| Drug | Mechanism | Notes |
|---|---|---|
| Inhaled NO (iNO) | Activates soluble guanylate cyclase → ↑cGMP → smooth muscle relaxation | FDA-approved for PPHN; start at 20 ppm; lower doses (10 ppm) may suffice in preterms; no added benefit >40 ppm; monitor methemoglobin (reduce if >4%) and NO2 (reduce if >1-2 ppm) |
| Sildenafil | PDE-5 inhibitor → ↑cGMP | Used when iNO unavailable or as adjunct; oral/IV |
| Bosentan | Endothelin receptor antagonist | Used beyond neonatal period into infancy |
| Prostacyclin (epoprostenol) | ↑cAMP → smooth muscle relaxation | Pulmonary vasodilator; inhaled or IV |
| Milrinone | PDE-3 inhibitor → ↑cAMP | Provides inotropy + pulmonary vasodilation; useful for RV support |
-
The OI (Oxygen Index) guides initiation of iNO: OI ≥ 15 is the threshold
- OI = (Mean Airway Pressure × FiO2 × 100) / PaO2
-
iNO has not been shown to reduce ECMO need in CDH
-
Harriet Lane, p. 652; Barash, p. 3578-3579; Goodman & Gilman, p. 1606
6. Exogenous Surfactant
- Indicated particularly in MAS and RDS-associated PPHN
- Reduces ventilation-perfusion mismatch and may reduce need for ECMO
7. Extracorporeal Membrane Oxygenation (ECMO)
Reserved for refractory PPHN. Indications:
- OI >40 for >3 hours, OR
- Alveolar-arterial O2 gradient (A-aO2) ≥610 for 8 hours
- Severe cardiovascular instability unresponsive to maximal therapy
Eligibility criteria:
-
Birth weight >2,000 g
-
Gestational age >34 weeks
-
Obtain head ultrasound and consider EEG before initiating (risk of intracranial hemorrhage)
-
Harriet Lane, p. 652
Prognosis
-
Prognosis is directly tied to ability to reduce PVR and correction of the underlying cause
-
Key adverse prognostic factor: associated hypoxic-ischemic encephalopathy (HIE)
-
Survival and outcomes have markedly improved with iNO and ECMO availability
-
Novel therapies targeting PPHN pathophysiology (based on animal model insights) are in active clinical trials
-
Barash, p. 3579; Creasy & Resnik, p. 1790
Recent Evidence (PubMed, 2024)
- A 2024 network meta-analysis (Fei et al., Crit Care Med, PMID 38363176) compared different PPHN treatments - currently the highest-evidence comparative study available
- A 2024 RCT (Kallimath et al., BMC Pediatr, PMID 39487423) compared oral sildenafil versus bosentan for PPHN - both showed efficacy
- A 2024 review (Cookson & Kinsella, Clin Perinatol, PMID 38325949) provides updated guidance on inhaled NO in neonatal pulmonary hypertension
Key Summary Table
| Domain | Key Points |
|---|---|
| Incidence | ~2/1,000 live term births |
| Core mechanism | Failed PVR reduction at birth → R-to-L shunting via DA and FO |
| Main triggers | MAS, asphyxia, CDH, sepsis, idiopathic |
| Hallmark sign | Pre/postductal SpO2 gradient + hypoxia out of proportion to CXR |
| First-line Rx | Optimize ventilation + iNO 20 ppm |
| ECMO threshold | OI >40 for >3h or A-aO2 ≥610 for 8h |
| Adjuncts | Sildenafil, bosentan, milrinone, prostacyclin |
Morphine mechanism of action, uses, adverse effects, dosage calculation
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I have everything needed for a comprehensive, well-cited answer. Here it is:
Morphine: Mechanism of Action, Uses, Adverse Effects, and Dosage
1. Mechanism of Action
Morphine is the prototypical full mu (μ) opioid receptor agonist. It produces analgesia by binding stereospecifically to G protein-coupled opioid receptors (GPCRs) located throughout the CNS, spinal cord, and peripheral sensory nerve endings.
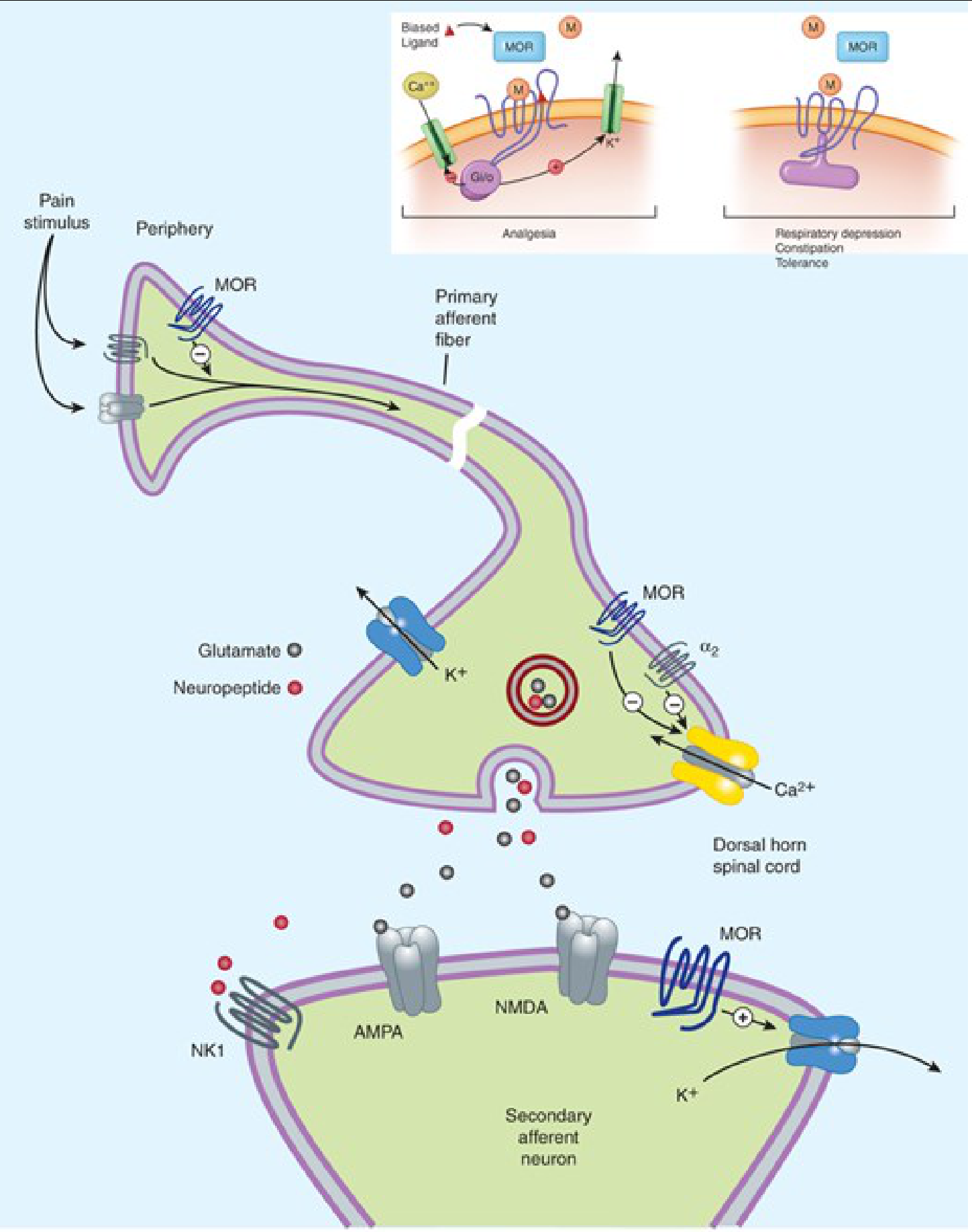
Figure: Morphine (M) acts at μ-opioid receptors (MOR) at peripheral nerve endings, presynaptic terminals in the dorsal horn, and postsynaptic neurons. Inset: G-protein coupling mediates analgesia; β-arrestin coupling mediates side effects (respiratory depression, constipation, tolerance). - Katzung's Basic and Clinical Pharmacology, 16th ed.
Receptor Types
Three major opioid receptor classes exist - all GPCRs:
| Receptor | Symbol | Primary Effects |
|---|---|---|
| Mu | μ (MOR) | Analgesia, euphoria, respiratory depression, constipation, miosis, physical dependence |
| Kappa | κ | Analgesia, sedation, dysphoria, miosis |
| Delta | δ | Analgesia, mood modulation |
Morphine is primarily selective for μ receptors, with some affinity for κ and δ receptors.
Cellular Mechanism
When morphine binds the MOR and activates Gi/o proteins, two key ion channel effects occur:
- Closes voltage-gated Ca²⁺ channels on presynaptic nerve terminals → reduces release of excitatory neurotransmitters (glutamate, substance P) into the dorsal horn
- Opens K⁺ channels on postsynaptic neurons → hyperpolarization → reduced neuronal firing
The net result is inhibition of pain signal transmission at multiple levels:
- Periphery (inflamed tissue)
- Spinal cord dorsal horn (presynaptic and postsynaptic)
- Supraspinal CNS (thalamus, periaqueductal gray, limbic system)
Pain is attenuated both by raising the pain threshold at the spinal cord level and by altering the brain's perception of pain.
The Two-Pathway Model (Biased Agonism)
- G-protein pathway (Gi/o) → analgesia
- β-arrestin pathway → respiratory depression, constipation, tolerance
This distinction is driving research into "biased ligands" that selectively activate the G-protein arm while sparing β-arrestin-mediated side effects.
- Katzung's Basic and Clinical Pharmacology, 16th ed., pp. 873-875
- Lippincott Illustrated Reviews Pharmacology, p. 706
2. Pharmacokinetics
| Property | Detail |
|---|---|
| Oral bioavailability | ~25-35% (high first-pass hepatic metabolism) |
| Onset (IV) | 5-10 min |
| Onset (oral) | 30-60 min |
| Duration of action | 4-5 hours (systemic); longer epidurally due to low lipophilicity |
| Lipophilicity | Least lipophilic of common opioids (vs fentanyl, methadone) → slower CNS penetration |
| Plasma protein binding | ~35% |
| Metabolism | Hepatic glucuronidation (does not rely primarily on CYP450) → two active metabolites: M6G and M3G |
| Active metabolites | M6G (morphine-6-glucuronide): potent analgesic, accumulates in renal failure; M3G (morphine-3-glucuronide): no analgesia, causes neuroexcitatory/antianalgesic effects |
| Elimination | Renal excretion of glucuronide conjugates |
Caution in renal impairment: M6G and M3G accumulate, risking prolonged sedation, respiratory depression, and neuroexcitation. Use with caution or avoid.
- Lippincott Illustrated Reviews Pharmacology, pp. 706-707
3. Clinical Uses
| Indication | Notes |
|---|---|
| Severe acute pain | Trauma, postoperative, cancer pain - prototype opioid agonist for moderate-severe pain |
| Chronic pain | Extended-release formulations (MS Contin, Kadian) for cancer and non-cancer pain |
| Acute pulmonary edema | IV morphine dramatically relieves dyspnea from left ventricular failure via venodilation and reduced preload/afterload; also reduces anxiety |
| Myocardial infarction/ACS | 2-4 mg IV (up to 0.1 mg/kg) for pain and anxiety unresponsive to nitrates; reduces O₂ demand |
| Antitussive | Suppresses medullary cough reflex (codeine/dextromethorphan more commonly used) |
| Antidiarrheal | Decreases GI motility, increases intestinal tone (loperamide/diphenoxylate used clinically) |
| Anesthesia | Pre-anesthetic medication, intraoperative analgesia, postoperative pain control; neuraxial (epidural/intrathecal) analgesia |
| Palliative care | Dyspnea relief and pain control in terminal illness |
- Lippincott Illustrated Reviews Pharmacology, p. 707; Rosen's Emergency Medicine, p. 758
4. Adverse Effects
Figure: Major adverse effects of opioids including morphine. - Lippincott Illustrated Reviews Pharmacology
Organized by System
CNS:
- Sedation, drowsiness
- Euphoria / dysphoria
- Miosis (pinpoint pupils - μ and κ mediated; little tolerance develops; diagnostically important - other causes of coma cause mydriasis)
- Increased intracranial pressure via CO₂ retention → cerebral vasodilation; contraindicated in head trauma/severe TBI
- Opioid-induced hyperalgesia (OIH) with prolonged use
Respiratory:
- Respiratory depression - most serious and life-threatening adverse effect
- Reduces responsiveness of medullary respiratory center neurons to CO₂
- Can occur at therapeutic doses in opioid-naive patients
- Most common cause of death in acute opioid overdose
- Use with extreme caution in: COPD, obstructive sleep apnea, cor pulmonale
Cardiovascular:
- Minimal effect at low doses
- Hypotension and bradycardia at higher doses
- Histamine release from mast cells → urticaria, sweating, bronchoconstriction, vasodilation/hypotension; avoid or use with caution in asthma
Gastrointestinal:
- Constipation - most common; tolerance rarely develops; start prophylactic stimulant laxative (senna)
- Nausea and vomiting (stimulates chemoreceptor trigger zone in area postrema)
- Increased biliary tract pressure (contracts gallbladder, constricts biliary sphincter)
Genitourinary:
- Urinary retention - inhibits voiding reflex, increases sphincter tone; may require catheterization
Endocrine (chronic use):
- Opioid-induced androgen deficiency (OPIAD) - suppresses hypothalamic-pituitary-gonadal axis → decreased testosterone → fatigue, decreased libido, osteoporosis, depression
Reproductive:
- Prolongs second stage of labor (transient decrease in uterine contractions)
- Crosses placenta → neonatal respiratory depression and neonatal abstinence syndrome
Tolerance vs. No Tolerance
| Develops Tolerance | No/Minimal Tolerance |
|---|---|
| Analgesia | Constipation |
| Respiratory depression | Miosis |
| Euphoria | |
| Sedation | |
| Emesis | |
| Urinary retention |
- Lippincott Illustrated Reviews Pharmacology, pp. 706-716
5. Drug Interactions
| Interacting Drug/Class | Effect |
|---|---|
| Benzodiazepines | Synergistic CNS and respiratory depression; boxed warning against co-prescribing |
| MAOIs | Serious / life-threatening reactions (serotonin syndrome, hypertensive crisis) |
| Phenothiazines / antipsychotics | Enhanced CNS depression |
| CNS depressants (alcohol, barbiturates, antihistamines) | Additive respiratory and CNS depression |
| Gabapentinoids | Increased respiratory depression risk |
Morphine does not significantly rely on CYP450 enzymes (unlike fentanyl, methadone, oxycodone), so it has a lower drug interaction profile via this pathway.
- Lippincott Illustrated Reviews Pharmacology, p. 716
6. Dosage Calculations
Standard Doses
| Route | Standard Dose | Onset | Duration |
|---|---|---|---|
| IV / IM / SC | 0.1 mg/kg (adults: typically 2-4 mg IV q2-4h) | 5-10 min (IV) | 3-4 h |
| Oral (immediate release) | 15-30 mg q4h | 30-60 min | 4-5 h |
| Oral (extended release) | 15-200 mg q8-12h (titrated) | 1-4 h | 8-24 h |
| Epidural | 2-5 mg (surgical); 0.05-0.1 mg/kg per dose | Slow (low lipophilicity) | 12-24 h |
| Intrathecal | 0.1-0.3 mg | Minutes | 8-24 h |
Pediatric IV dosing: 0.05-0.1 mg/kg IV q2-4h (titrated to effect)
Equianalgesic Dose Table (Standard Reference)
When switching opioids, use these equianalgesic conversions (all equal to 30 mg oral morphine):
| Drug | Oral/Rectal | Parenteral | Notes |
|---|---|---|---|
| Morphine | 30 mg | 10 mg | Parenteral is 3x more potent than oral |
| Oxycodone | 20 mg | N/A | ~1-1.5x more potent than oral morphine |
| Hydrocodone | 20 mg | N/A | ~1-1.5x more potent than oral morphine |
| Hydromorphone | 7 mg | 1.5 mg | Oral: 4-7x more potent; Parenteral: ~20x more potent |
| Fentanyl | N/A | 15 μg/hr (TD) | ~80x more potent than morphine transdermally |
| Meperidine | 300 mg | 75 mg | Avoid in palliative/chronic settings |
- Sleisenger & Fordtran's GI and Liver Disease, Table 132.2, p. 2721
- Rosen's Emergency Medicine, p. 758
Morphine Dose Conversion Example
Convert 60 mg oral morphine/day to IV morphine:
- Oral:parenteral ratio = 3:1
- 60 mg oral ÷ 3 = 20 mg IV morphine/day
- Divided q4h = 20 ÷ 6 = ~3.3 mg IV q4h
Convert 60 mg oral morphine/day to oral hydromorphone:
- 60 mg oral morphine ÷ 7 (oral hydromorphone is ~7x more potent) = ~8.5 mg oral hydromorphone/day (titrate cautiously)
7. Contraindications and Precautions
| Contraindication | Reason |
|---|---|
| Head trauma / raised ICP | CO₂ retention worsens cerebral vasodilation |
| Severe respiratory depression | Additive effect |
| Acute asthma attack | Histamine release + respiratory depression |
| Bowel obstruction / ileus | Reduces GI motility |
| MAOIs (concurrent or within 14 days) | Risk of severe interaction |
| Renal failure | M6G and M3G accumulation |
| Labor analgesia | Neonatal respiratory depression |
8. Overdose / Reversal
Classic opioid toxidrome:
- Miosis (pinpoint pupils)
- Respiratory depression / apnea
- Decreased consciousness / coma
Reversal agent: Naloxone (Narcan)
- Competitive opioid receptor antagonist
- 0.4-2 mg IV/IM/SC/intranasal; repeat q2-3 min PRN
- Titrate to restore adequate respiration (avoid precipitating acute withdrawal)
- Short half-life (~60-90 min) - may need repeat dosing or infusion for long-acting opioids
Summary Table
| Parameter | Key Points |
|---|---|
| Primary receptor | μ (MOR) >> κ, δ |
| Cellular mechanism | ↓ Ca²⁺ presynaptically + ↑ K⁺ postsynaptically → neuronal inhibition |
| Key uses | Severe pain, ACS, pulmonary edema, anesthesia, palliative care |
| Lethal adverse effect | Respiratory depression |
| Most common adverse effect | Constipation |
| No tolerance to | Constipation, miosis |
| Equianalgesic oral:IV ratio | 3:1 (30 mg oral = 10 mg IV) |
| Reversal | Naloxone |
| Caution in | Renal failure (M6G accumulation), COPD, head trauma |
Enlighten me about beta arrestin pathway that is responsible for respiratory depression
Finding Sources
Finding Sources
Searching PubMed
"beta-arrestin" opioid receptor "respiratory depression" biased agonism
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.