anaemia
Reading File
Finding Sources
Searching PubMed
"anaemia" OR "anemia"[MeSH Terms] AND "classification"
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Here is a thorough overview of anaemia drawn from Harrison's Principles of Internal Medicine (22nd ed.), Robbins & Kumar Pathologic Basis of Disease, Frameworks for Internal Medicine, and Bailey & Love's Short Practice of Surgery.
Anaemia
Definition
Anaemia is defined as blood counts (haemoglobin/haematocrit) below the normal for a given population. In practice, common WHO thresholds are:
- Adult men: Hb < 13 g/dL
- Adult women: Hb < 12 g/dL
- Pregnant women: Hb < 11 g/dL
It results in reduced oxygen delivery to tissues, triggering compensatory haemodynamic responses.
Classification
There are two major approaches to classifying anaemia:
1. By Red Cell Size (MCV-based) - Harrison's 22E

| Category | MCV | Key Causes |
|---|---|---|
| Microcytic | < 80 fL | Iron deficiency, thalassaemia, anaemia of chronic disease (sometimes), sideroblastic anaemia |
| Normocytic | 80-100 fL | Aplastic anaemia, renal disease, haemolysis (acute), endocrinopathies, marrow infiltration, myeloma |
| Macrocytic | > 100 fL | B12/folate deficiency, hypothyroidism, liver disease, alcohol use, myelodysplasia, medications |
Peripheral blood smear comparison of microcytic vs macrocytic RBCs:
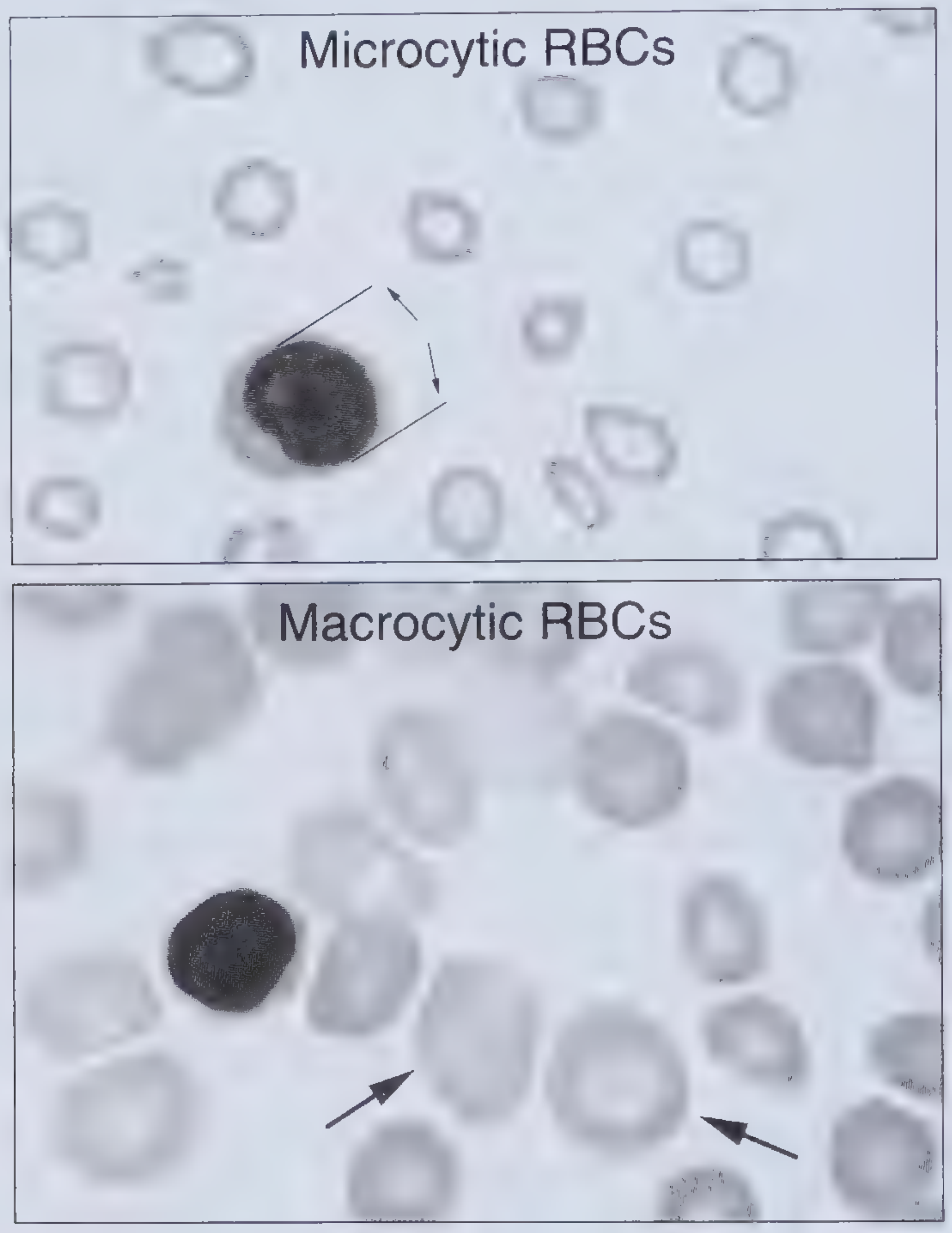
(Top: microcytic RBCs - note small size and large central pallor compared to lymphocyte nucleus. Bottom: macrocytic RBCs - note large, oval cells)
2. By Mechanism (Pathophysiologic Classification) - Robbins & Kumar
| Mechanism | Examples |
|---|---|
| Blood Loss | Acute (trauma), Chronic (GI lesion, menorrhagia) |
| Increased Destruction (Haemolysis) | |
| - Intrinsic/inherited | Hereditary spherocytosis, G6PD deficiency, pyruvate kinase deficiency, sickle cell disease, thalassaemia |
| - Acquired/extrinsic | Autoimmune haemolytic anaemia, microangiopathic (TTP, HUS, DIC), PNH, drug-induced, malaria |
| Decreased Production | |
| - Nutritional deficiency | Iron, B12, folate, copper deficiency |
| - Erythropoietin deficiency | Chronic kidney disease |
| - Marrow failure | Aplastic anaemia, Fanconi anaemia |
| - Marrow replacement | Metastatic tumour, granulomatous disease |
| - Inflammation | Anaemia of chronic disease (hepcidin-mediated iron sequestration) |
The reticulocyte count is the key first step to distinguish mechanism:
- Elevated reticulocytes → blood loss or haemolysis (hyperproductive response)
- Low/normal reticulocytes → underproduction (bone marrow problem)
Clinical Features
The severity of symptoms depends on chronicity and rate of onset. Even severe anaemia may be well tolerated if it develops gradually.
Symptoms:
- Fatigue, loss of stamina
- Dyspnoea on exertion
- Palpitations
- Dizziness, headache
Physical signs:
- Pallor (mucous membranes, palmar creases, nail beds, conjunctivae)
- Tachycardia, wide pulse pressure, bounding pulses
- Forceful heartbeat, systolic flow murmur
- In severe cases: cardiac decompensation
Key Anaemia Types in Detail
Iron Deficiency Anaemia (most common worldwide)
- Affects ~10% in high-income countries; 25-50% in low-income countries (Robbins & Kumar Basic Pathology)
- Causes: poor intake, chronic blood loss (GI, menstrual), malabsorption
- Labs: low serum ferritin (best initial test), low serum iron, high TIBC (300-350 µg/dL normal), transferrin saturation ~33% normal
- Smear: hypochromic, microcytic RBCs with increased central pallor
Megaloblastic Anaemia (B12 / Folate Deficiency)
- Mechanism: impaired DNA synthesis → nuclear-cytoplasmic asynchrony → ineffective haematopoiesis
- Often presents with pancytopenia (anaemia + thrombocytopenia + granulocytopenia)
- Earliest smear finding: hypersegmented neutrophils (5+ lobes)
- MCV typically > 110 fL; macro-ovalocytes on smear
- B12 deficiency also causes subacute combined degeneration of the spinal cord
Anaemia of Chronic Disease / Inflammation
- Mediated by hepcidin (released by liver in response to IL-6)
- Hepcidin degrades ferroportin → blocks iron release from macrophages → iron-restricted erythropoiesis
- Labs: low serum iron, low TIBC (unlike IDA), elevated ferritin
- Often normocytic, can be microcytic in long-standing cases
Hereditary Spherocytosis
- Defect in RBC membrane skeleton proteins (ankyrin, spectrin, band 3)
- Spherocytes trapped and destroyed in the spleen
- Triad: anaemia + splenomegaly + jaundice
- Coombs test negative (distinguishes from autoimmune haemolytic anaemia)
- Splenectomy corrects the anaemia
Investigations / Diagnostic Approach
- FBC with RBC indices (MCV, MCH, MCHC)
- Reticulocyte count - key to mechanism (high vs. low)
- Peripheral blood smear - morphology
- Iron studies: serum iron, ferritin, TIBC
- B12 and folate levels
- Renal function (CKD-related)
- LFTs, TFTs as indicated
- Direct Coombs test if haemolysis suspected
- Bone marrow biopsy if aplasia or infiltration suspected
Treatment Principles (Surgical Context)
From Bailey & Love's / Pye's Surgical Handicraft:
- A Hb of ≥ 10 g/dL without myocardial disease is generally acceptable for surgery, as increased cardiac output can compensate
- Below this threshold, urgency of the procedure determines whether iron supplementation or blood transfusion is used
- Stored red cells are poor oxygen transporters immediately post-transfusion; transfusion restores volume but not immediate O2 delivery
- In bowel surgery, blood transfusion increases wound infection risk and may worsen prognosis
Sources: Harrison's Principles of Internal Medicine 22E, p. 492 | Robbins & Kumar Basic Pathology | Frameworks for Internal Medicine, p. 330 | Bailey and Love's Short Practice of Surgery 28E | Pye's Surgical Handicraft 22E
This is a shared conversation. Sign in to Orris to start your own chat.