How to learn ecg
Reading File
Finding Sources
Searching the Web
how to learn ECG interpretation step by step guide 2025
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Searching Images
normal ECG waveform P wave QRS complex T wave labeled diagram
Reading File
Now I have enough material to give a comprehensive, well-structured answer. Let me compile it.
How to Learn ECG Interpretation
Learning ECGs is a skill built in layers — understand the basics first, then apply a systematic method every time, then pattern-recognize through repetition. Here's the full roadmap:
1. Understand What the ECG is Measuring
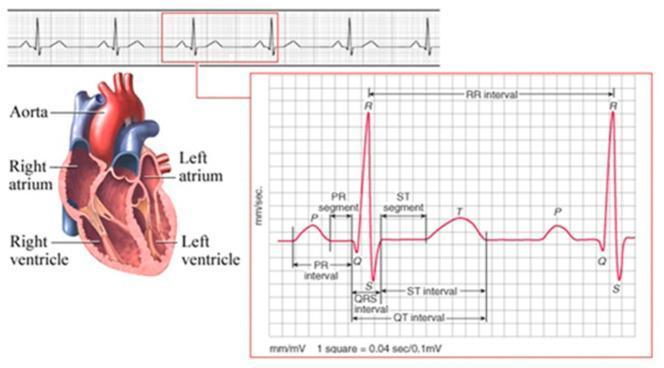
The ECG records the heart's electrical activity as waves on paper. Each component reflects a specific electrical event:
| Wave/Segment | Electrical Event |
|---|---|
| P wave | Atrial depolarization (SA node → atrial muscle) |
| PR interval | AV nodal delay |
| QRS complex | Ventricular depolarization |
| ST segment | Ventricular plateau (early repolarization) |
| T wave | Ventricular repolarization |
| U wave | (Purkinje repolarization — often not visible) |
The normal P wave is positive in lead II and negative in aVR because atrial depolarization spreads from the SA node downward and to the left — pointing toward lead II's positive pole. — Harrison's Principles of Internal Medicine 22E, p. 1913
2. Master the Paper and Calibration
Paper speed: 25 mm/sec
- 1 small box = 1 mm = 0.04 seconds
- 1 large box = 5 mm = 0.2 seconds
- Amplitude: 10 mm = 1 mV
Heart rate calculation:
- Regular rhythm: 300 ÷ number of large boxes between R waves
- 1 box = 300 bpm, 2 boxes = 150, 3 = 100, 4 = 75, 5 = 60, 6 = 50
- Irregular rhythm: Count complexes in the 10-second rhythm strip × 6
3. Use a Systematic Approach — Every Time
The Harriet Lane Handbook and Harrison's both emphasize a fixed sequence. Never skip steps:
Step 1 — Rate
Calculate using the 300-rule above.
Step 2 — Rhythm
- Is every QRS preceded by a P wave?
- Is the P wave axis normal? (Upright in I and aVF = sinus rhythm)
- Is the R-R interval regular?
Step 3 — Axis
Look at leads I and aVF:
- Both positive → Normal axis (−30° to +90°)
- I positive, aVF negative → Left axis deviation
- I negative, aVF positive → Right axis deviation
- Both negative → Extreme axis
Step 4 — Intervals
| Interval | Normal Value |
|---|---|
| PR interval | 0.12–0.20 sec (<1 large box) |
| QRS duration | <0.12 sec (<3 small boxes) |
| QTc (Bazett) | ≤0.44–0.46 sec |
QTc = QT (sec) / √R-R interval (sec) — Harriet Lane Handbook, 23rd ed.
Step 5 — P Waves
- Normal P: duration <0.09 sec in children, amplitude <3 mm
- Right atrial enlargement: tall peaked P in II (>2.5 mm), biphasic P in V1
- Left atrial enlargement: wide P in II (≥3 small boxes), notched ("P mitrale")
Step 6 — QRS Complex
- Septal depolarization: left → right, produces small r in V1 and small q in V6
- R wave progression: R grows from V1 to V5/V6; S dominates right precordials
- Bundle branch blocks: QRS ≥0.12 sec; use "WiLLiaM MaRRoW" mnemonic
- LBBB: W in V1, M in V6
- RBBB: M in V1, W in V6
- Check for Q waves (pathological = >1/3 QRS height OR >1 small box wide)
Step 7 — ST Segments & T Waves
- ST elevation → transmural ischemia/injury (or pericarditis, early repolarization)
- ST depression → subendocardial ischemia
- Hyperacute T waves → earliest sign of STEMI
- T wave inversions → ischemia, strain patterns, right/left heart disease
Localizing ischemia by lead:
| Territory | Leads showing changes |
|---|---|
| Anterior wall | V1–V6, I, aVL |
| Inferior wall | II, III, aVF |
| Posterior wall | Reciprocal ST depression V1–V3 |
| Right ventricle | Right-sided leads (V3R, V4R) |
— Harrison's Principles of Internal Medicine 22E, p. 1916
4. Learn the Core Patterns (Build Your Pattern Library)
After the basics, focus on these high-yield diagnoses:
- Arrhythmias: sinus tach/brady, AF, flutter, SVT, VT, AV blocks (1st/2nd/3rd degree)
- Bundle branch blocks: RBBB, LBBB
- ACS: STEMI (with territory), NSTEMI pattern, Wellens' syndrome
- Chamber enlargement: RAE, LAE, RVH, LVH
- Electrolyte abnormalities: peaked T waves (hyperkalemia), prolonged QT (hypokalemia/hypocalcemia)
- Special patterns: WPW (delta waves), Brugada, long QT syndrome, pericarditis (saddle-shaped ST elevation)
5. Practice Resources (Structured Progression)
Books (in order of accessibility)
- "ECG Made Easy" – John Hampton — ideal starting point
- "Goldberger's Clinical Electrocardiography: A Simplified Approach" (referenced in Harrison's) — intermediate
- Braunwald's Heart Disease / Harrison's — advanced reference for pathophysiology
Free Online Resources
- ECGwaves.com — systematic tutorials with examples
- Litfl.com (Life in the Fast Lane) — extensive ECG library with clinical context
- 123sonography ECG course — structured video curriculum
- YouTube – Dr. Smith's ECG Blog, Dirty Medicine, Armando Hasudungan — visual learners
Practice Platforms
- ECG.Academy — spaced repetition of real ECGs
- Cardioserv — board-style ECG interpretation
- AHA/ACLS practice strips — arrhythmia-focused
6. The Key to Getting Good: Volume + Feedback
- Aim for 500+ ECGs before feeling truly confident. This is not negotiable.
- Review ECGs with clinical context — knowing the patient's presentation is how patterns become meaningful.
- Use spaced repetition: revisit difficult patterns regularly.
- When you misread an ECG, understand why — trace the systematic steps back to where you went wrong.
Summary path:
Paper basics → Normal waveforms → Systematic 7-step method → Core pathology patterns → High-volume practice with feedback
The systematic approach is what separates reliable from unreliable interpreters. Pick one method and use it identically on every single ECG, even when the answer seems obvious.
This is a shared conversation. Sign in to Orris to start your own chat.