Wrist drop case sheet orthopaedics
Reading File
Finding Sources
Finding Sources
Searching the Web
wrist drop case sheet orthopaedics radial nerve palsy clinical examination
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Finding Sources
Here is a comprehensive Wrist Drop — Orthopaedic Case Sheet compiled from authoritative textbooks.
Wrist Drop (Radial Nerve Palsy) — Orthopaedic Case Sheet
1. Definition
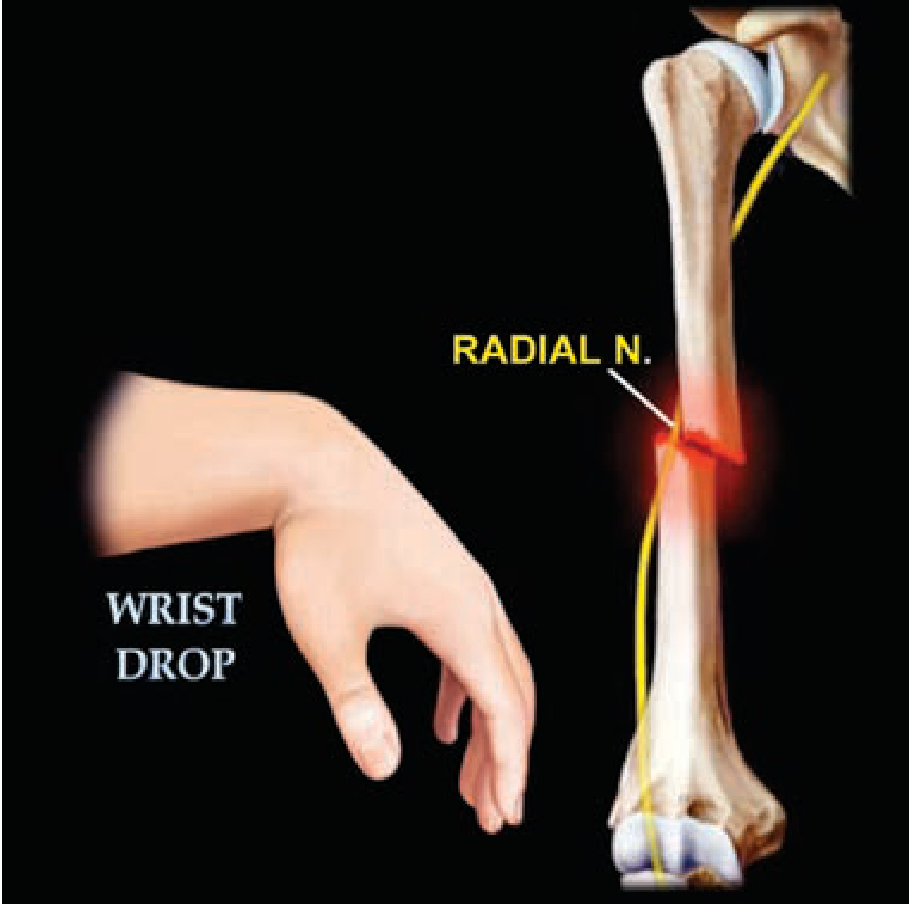
Wrist drop is the inability to actively extend the hand at the wrist joint, resulting from paralysis of the wrist extensor muscles innervated by the radial nerve (C5–C8, T1).
2. Anatomy Relevant to the Case
| Level | Branch / Segment | Key Structures Supplied |
|---|---|---|
| Axilla | Radial nerve proper | Triceps brachii (all heads), anconeus |
| Spiral (radial) groove | Posterior to humerus | Brachioradialis, ECRL, ECRB |
| Lateral intermuscular septum / radial tunnel | Before entering forearm | Extensor carpi radialis brevis |
| Supinator canal (arcade of Frohse) | Deep branch → Posterior Interosseous Nerve (PIN) | Extensor digitorum, extensor carpi ulnaris, extensor digiti minimi, APL, EPL, EPB, EIP |
| Distal forearm | Superficial radial nerve (sensory only) | Dorsal radial skin — 1st web space (exclusive territory) |
3. Common Causes by Level
High (Axillary) Radial Nerve Palsy
- Prolonged crutch use ("crutch palsy")
- Fracture/dislocation of proximal humerus
- Features: Wrist drop + Triceps weakness + Loss of triceps jerk
Mid-level (Spiral Groove) Radial Nerve Palsy ← Most common
- Humeral shaft fracture — especially distal 1/3 spiral fractures (Holstein-Lewis fracture)
- Saturday night palsy / Park bench palsy — compression during sleep with arm draped over edge
- Bridegroom's palsy / Honeymooner's palsy — compression by partner's head on arm
- Features: Wrist drop, finger/thumb drop; triceps spared (branches leave before spiral groove); sensory loss dorsum of hand
Distal (Posterior Interosseous Nerve) Palsy
- Supinator syndrome / Arcade of Frohse compression
- Radial head fracture/dislocation
- Features: No wrist drop (ECRL and ECRB spared — branch off proximal); finger/thumb drop only; no sensory loss
4. Clinical Presentation
Symptoms
- Inability to raise/extend the wrist and fingers
- Weak grip (because grip strength depends on a stable, extended wrist)
- Numbness/tingling over dorsum of hand (radial 3.5 digits) and 1st web space
- History of relevant trauma, prolonged pressure, or humeral fracture
Classic Sign
Wrist drop — wrist hangs in flexion; patient cannot dorsiflex the wrist against gravity or resistance
5. Physical Examination
Inspection
- Wrist in flexion/pronation ("dropped" position)
- Wasting of forearm extensors (chronic cases)
Motor Testing
| Muscle | Action to Test | Root |
|---|---|---|
| Triceps brachii | Elbow extension against resistance | C7 |
| Brachioradialis | Forearm flexion at 90° with neutral rotation | C5–C6 |
| ECRL / ECRB | Wrist dorsiflexion (radial deviation) | C6–C7 |
| Extensor digitorum | Finger extension at MCP joints | C7–C8 |
| Extensor pollicis longus | Thumb extension (hitchhiker test) | C7–C8 |
| Abductor pollicis longus | Thumb abduction | C7–C8 |
Sensory Testing
- Test dorsum of 1st web space (exclusive radial territory)
- Test dorsolateral forearm (posterior cutaneous nerve of forearm — branches proximal to groove, often spared)
Reflexes
- Brachioradialis reflex (supinator jerk) — diminished or absent
- Triceps jerk — absent only in high axillary lesions
Special Tests
- Tendodesis effect: Passive wrist extension causes finger flexion — useful to demonstrate to patient
- Wrist extension against resistance — test for partial palsy recovery
6. Grading of Nerve Injury (Seddon's Classification)
| Grade | Description | Prognosis |
|---|---|---|
| Neuropraxia | Conduction block; axon intact | Full recovery; weeks to months |
| Axonotmesis | Axon disrupted; endoneurium intact | Good recovery; regrowth ~1 mm/day |
| Neurotmesis | Complete nerve division | Needs surgical repair; poor prognosis |
Most radial nerve injuries from humeral shaft fractures are neuropraxias — function typically returns within 3–4 months. — Schwartz's Principles of Surgery, 11th Ed.
7. Investigations
| Investigation | Purpose |
|---|---|
| X-ray (AP + lateral humerus) | Identify humeral shaft fracture, callus, exostosis |
| EMG / Nerve conduction studies | Confirm site, extent, and severity of lesion; baseline before surgery; assess reinnervation |
| MRI | Nerve compression by mass, ganglion, tumour |
| Ultrasound | Nerve continuity, neuroma, dynamic compression |
EMG/NCS should be done at 3–4 weeks after injury (earlier studies may be falsely normal due to Wallerian degeneration timeline).
8. Differential Diagnosis
| Condition | Differentiating Feature |
|---|---|
| C7 radiculopathy | Triceps weakness + neck pain + reflexes; no isolated sensory loss in radial territory |
| Posterior cord brachial plexus lesion | Deltoid weakness (axillary nerve) also present |
| Central lesion (stroke, cortical) | UMN signs (spasticity, hyperreflexia); no isolated nerve territory sensory loss |
| PIN syndrome | No wrist drop; no sensory loss |
| Lead neuropathy | Bilateral; exposure history; mainly motor |
9. Classic Hand Postures — Nerve Palsy Comparison
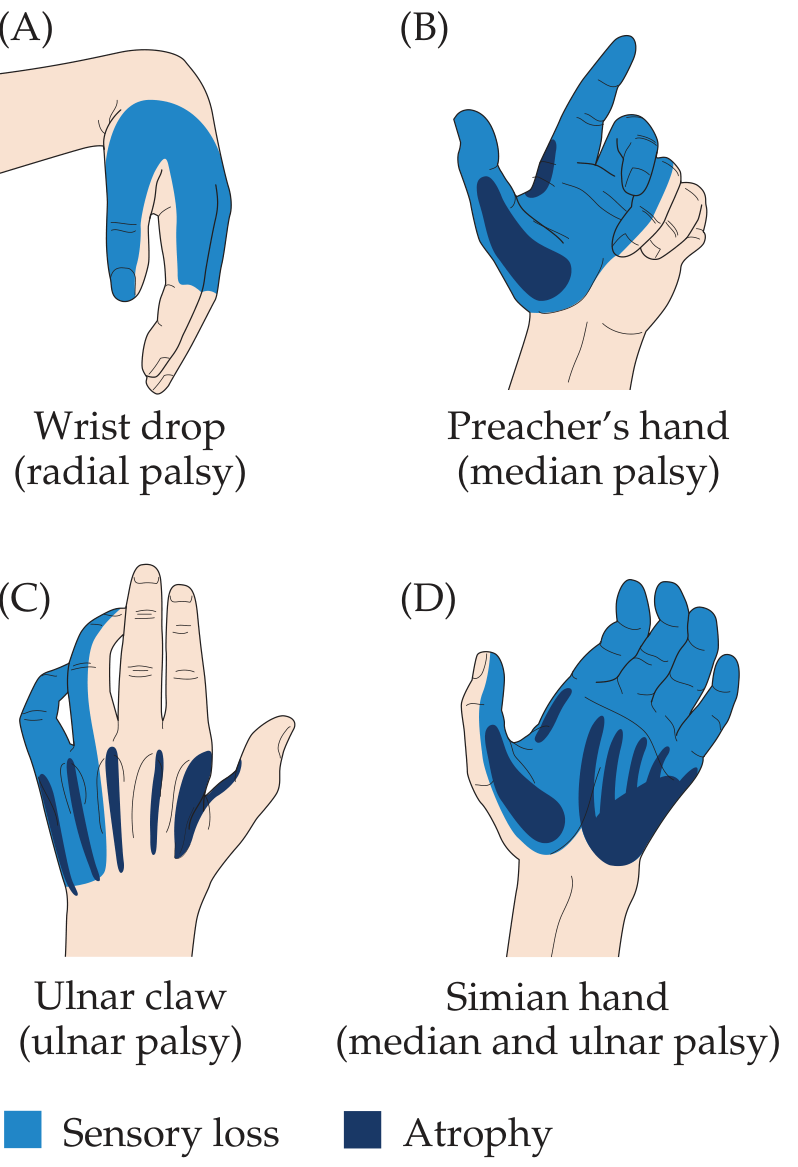
(A) Wrist drop — radial nerve
(B) Preacher's hand — proximal median nerve
(C) Ulnar claw — ulnar nerve
(D) Simian hand — combined median + ulnar nerve
(B) Preacher's hand — proximal median nerve
(C) Ulnar claw — ulnar nerve
(D) Simian hand — combined median + ulnar nerve
10. Management
Conservative (First-line for most cases)
- Treat the underlying cause — reduce/immobilize humeral fracture
- Cock-up wrist splint — maintains wrist in ~30–40° dorsiflexion to prevent contracture, improve grip
- Physiotherapy:
- Passive ROM exercises to prevent joint stiffness
- Muscle re-education as recovery begins
- Electrical stimulation to denervated muscles (controversial)
- Analgesia — NSAIDs/neuropathic agents (gabapentin, amitriptyline) for pain/paresthesias
- Watchful waiting with serial neurological assessment and EMG at 3–4 months
Surgical Indications
| Indication | Procedure |
|---|---|
| Open fracture with nerve division | Primary/delayed nerve repair or grafting |
| No recovery by 3–4 months + EMG showing no reinnervation | Nerve exploration ± repair |
| PIN compression (Arcade of Frohse) | Surgical decompression |
| Irreversible paralysis (late presentation) | Tendon transfer |
Tendon Transfers for Irreversible Wrist Drop
| Recipient (lost function) | Donor tendon |
|---|---|
| Wrist extensors (ECRL/ECRB) | FCU or FCR |
| Extensor digitorum communis | FCU |
| Extensor pollicis longus | PL or FDS |
11. Prognosis
- Neuropraxia (Saturday night palsy, most humeral shaft fractures): complete recovery expected in 6–12 weeks
- Axonotmesis: Recovery rate ~1 mm/day; time = distance from injury to first motor endplate
- Holstein-Lewis fracture with nerve injury: monitor 3–4 months before surgical exploration
- Poor prognostic signs: complete EMG silence at 4 months, laceration, high-energy injury
12. Key Eponyms & Mnemonics
| Eponym | Scenario |
|---|---|
| Saturday night palsy | Arm over bench/chair back during intoxicated sleep |
| Park bench palsy | Arm over park bench back |
| Bridegroom's / Honeymooner's palsy | Compression by partner's head resting on arm |
| Holstein-Lewis fracture | Spiral fracture of distal 1/3 humerus + radial nerve injury |
| Crutch palsy | Axillary radial nerve — triceps involved |
Mnemonic — Muscles of Radial Nerve (proximal to distal):
"Try A Beer, Round Bottles, Bring Down Ell"
Triceps → Anconeus → Brachioradialis → ECRL → ECRB → (via PIN) Brachialis-sharing / EDC → Ext digiti minimi → ECU → APL → EPB → EPL → EIP
"Try A Beer, Round Bottles, Bring Down Ell"
Triceps → Anconeus → Brachioradialis → ECRL → ECRB → (via PIN) Brachialis-sharing / EDC → Ext digiti minimi → ECU → APL → EPB → EPL → EIP
Sources: General Anatomy and Musculoskeletal System — THIEME Atlas of Anatomy; Schwartz's Principles of Surgery, 11th Ed.; Neuroanatomy through Clinical Cases, 3rd Ed.; Bradley and Daroff's Neurology in Clinical Practice
This is a shared conversation. Sign in to Orris to start your own chat.