A 50-year-old man with: Hemoptysis Chronic cough and dyspnea Previous treated tuberculosis Right upper lobe dullness to percussion with decreased breath sounds
Reading File
Finding Sources
Finding Sources
Searching PubMed
aspergilloma pulmonary post-tuberculosis hemoptysis
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive information to provide a thorough clinical analysis. Here is the full structured response:
Clinical Analysis: 50-Year-Old Man with Hemoptysis and Previous TB
Most Likely Diagnosis: Pulmonary Aspergilloma (Mycetoma)
This presentation is classic for aspergilloma complicating a post-tuberculosis cavity:
- Prior treated TB leaves residual parenchymal cavities
- Hemoptysis is the hallmark symptom
- Right upper lobe involvement - the typical site (TB preferentially destroys apices/upper lobes)
- Dullness to percussion + decreased breath sounds = consolidation or cavity with surrounding fibrosis
Pathophysiology
Aspergilloma is the saprophytic colonization of a pre-existing lung cavity by Aspergillus species (usually A. fumigatus). The fungus proliferates within the cavity without tissue invasion, forming a ball of fungal hyphae, mucus, and cellular debris. - Fishman's Pulmonary Diseases and Disorders, p. 2329
Key epidemiology:
- 11-17% of patients with post-TB cavities develop aspergilloma
- 20% of patients who recover from cavitary TB develop aspergilloma within 3 years
- In developing countries, TB is the predisposing factor in >90% of aspergilloma cases
Differential Diagnosis
| Diagnosis | Supporting Features | Against |
|---|---|---|
| Aspergilloma (top) | Post-TB cavity, hemoptysis, upper lobe, crescent sign on imaging | - |
| TB reactivation | Same site, cough, fever, weight loss | No systemic TB symptoms mentioned |
| Lung carcinoma | Hemoptysis, 50-year-old male, smoker risk | No weight loss/mass described |
| Rasmussen aneurysm | Erosion of pulmonary artery by TB cavity - massive hemoptysis | Rarer; usually catastrophic bleed |
| Chronic pulmonary aspergillosis (CPA) | Overlaps with aspergilloma; includes subacute invasive disease | Immunocompetent host |
| Bronchiectasis | Post-TB sequelae, chronic cough, hemoptysis | No productive purulent sputum history |
| Lung abscess | Cavity, constitutional symptoms | No fever, no odorous sputum |
Radiographic Features
The classic sign is Monod's sign (air crescent sign) - a crescent-shaped patch of air surrounding a solid round fungal ball within the cavity (3-5 cm diameter).
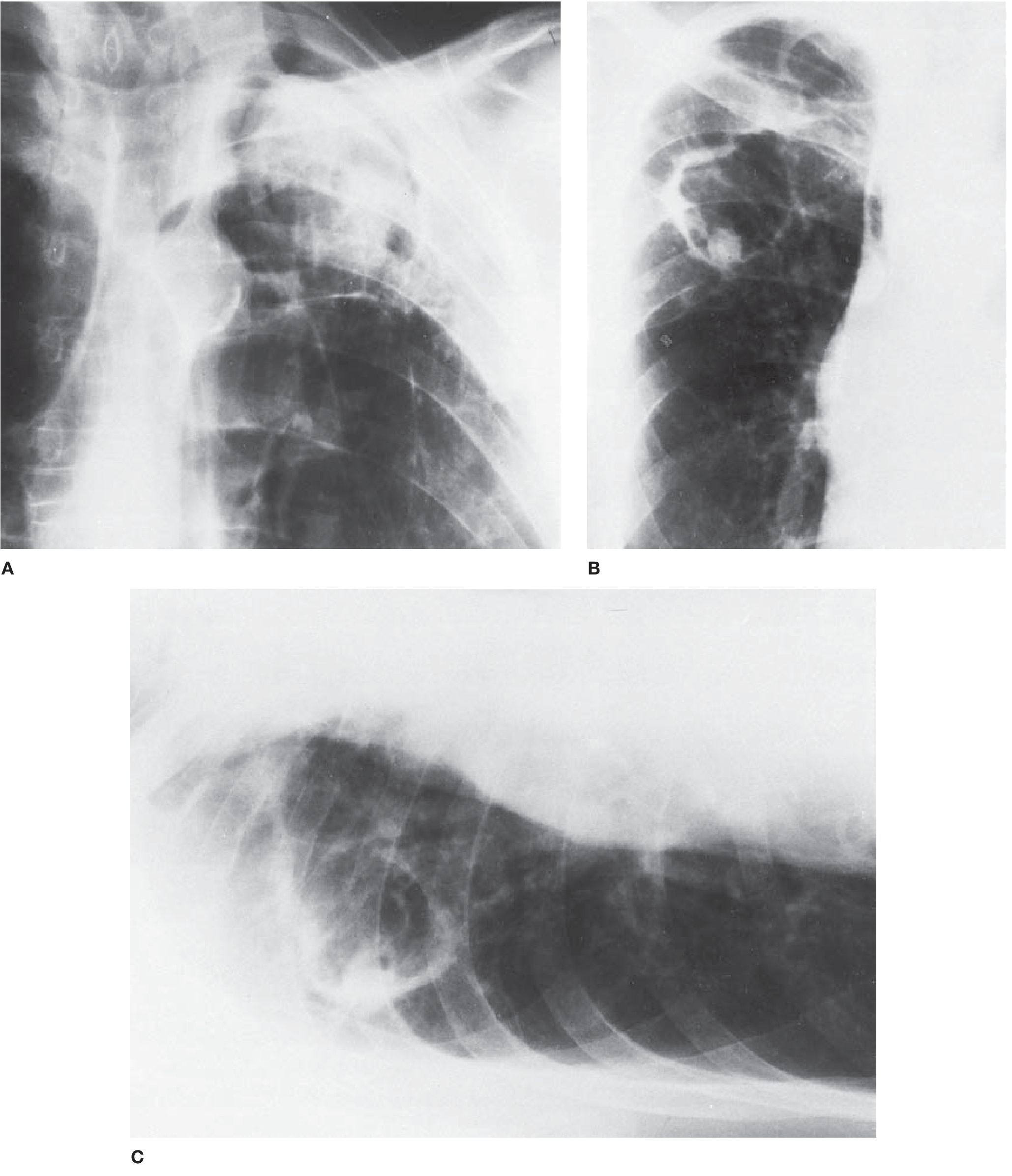
Figure: A 51-year-old man with a history of tuberculosis showing the classic crescent-shaped air patch (Monod's sign). Panel C (decubitus) demonstrates that the fungus ball moves when the patient changes position - pathognomonic. - Fishman's Pulmonary Diseases and Disorders, p. 2329-2330
CT findings:
- Globules of gas within the hyphal mass
- CT angiography may identify hypertrophic bronchial arteries supplying the cavity wall - important for planning bronchial artery embolization (BAE) in hemoptysis
Diagnostic Workup
| Test | Interpretation |
|---|---|
| Chest X-ray / CT chest | Look for Monod's (air crescent) sign; confirm cavity location |
| Aspergillus precipitins (IgG antibodies) | Present in >95% of patients with aspergilloma - most diagnostically helpful single test |
| Sputum culture for Aspergillus | Positive in >50% but lacks specificity |
| Bronchoscopy + BAL | If diagnosis uncertain; rules out endobronchial lesion or malignancy |
| Sputum AFB smear + culture | Exclude TB reactivation |
| Sputum cytology / bronchial washings | Exclude carcinoma |
| IgE, eosinophil count | May be elevated if allergic component (ABPA) co-exists |
| Lung biopsy | Reserved for atypical or ambiguous cases |
Management
General Approach
There is no consensus on treatment because of a lack of controlled trials. Management decisions depend on symptom severity, lung reserve, and surgical risk. - Fishman's Pulmonary Diseases, p. 2330
Step-by-Step:
1. Hemoptysis Control (Immediate Priority)
- Massive hemoptysis (>200-600 mL/24h) is life-threatening
- Bronchial artery embolization (BAE) is first-line for acute hemoptysis control - controls bleeding in 75-90% of patients, allows stabilization before definitive surgery
- Position patient with bleeding lung side DOWN to protect contralateral lung
- If airway compromised: intubate + emergency bronchoscopy
2. Surgical Resection (Definitive)
- Lobectomy or segmental resection is the gold standard for fit patients with single large aspergilloma and recurrent/massive hemoptysis
- Pre- and peri-operative antifungal therapy reduces relapse
- Significant morbidity/mortality risk, especially with underlying TB-damaged lung
3. Medical Therapy (For Inoperable Patients)
- Itraconazole 200-400 mg/day orally for 6-18 months: radiographic + symptomatic improvement in ~two-thirds of patients; recurrence common on stopping
- Voriconazole: used for itraconazole-resistant Aspergillus fumigatus cases; secondary resistance can develop with long-term use
- Jawetz Medical Microbiology: Aspergilloma treated with itraconazole or amphotericin B + surgery
4. Intracavitary Antifungal Instillation
- CT-guided percutaneous instillation of amphotericin B deoxycholate (AMB-D)
- Shown effective in cases of massive hemoptysis with resolution within 5 days
- Also: endobronchial instillation of ketoconazole via fiberoptic bronchoscopy
- Indicated when patient is unfit for surgery with severe pulmonary dysfunction
5. Cavernostomy (last resort for inoperable patients)
- Performed under local anesthesia
- Associated with significant mortality and mediocre outcomes
6. Asymptomatic / Mild Cases
- Careful follow-up with periodic chest X-rays without intervention is often appropriate
Poor Prognostic Predictors
- Progressive increase in aspergilloma size or number
- Severe underlying lung disease (poor reserve from prior TB)
- Immunosuppressive therapy or AIDS
- Rising Aspergillus-specific IgG titer
- Repetitive severe hemoptysis episodes
Summary Algorithm
Post-TB hemoptysis + upper lobe cavity
↓
Chest CT → Air crescent sign?
↓ Yes
Aspergillus precipitins (IgG) → likely >95% positive
↓
Assess fitness for surgery + hemoptysis severity
↓
Massive hemoptysis → BAE first → then lobectomy
Mild/moderate + operable → surgical resection
Inoperable → itraconazole ± intracavitary AmB
Asymptomatic → watchful waiting
Lab reports reveal HIV positivity and CD4 count of 43 . Chest CT shows a central nodule surrounded by ground glass changes. Microscopy shows fungi with narrow septated hyphae
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
I now have comprehensive data to build the full analysis. Here is the complete updated clinical picture:
Updated Diagnosis: Invasive Pulmonary Aspergillosis (IPA) in AIDS
How the New Data Changes Everything
| Feature | Before | Now |
|---|---|---|
| HIV status | Unknown | Positive - AIDS (CD4 = 43) |
| Diagnosis | Aspergilloma (saprophytic) | Invasive Pulmonary Aspergillosis |
| Mechanism | Cavity colonization | Angioinvasive tissue destruction |
| Urgency | Elective | Medical emergency - high mortality |
| CT finding | Air crescent (Monod) sign | Halo sign (nodule + ground-glass) |
| Microscopy | Fungal ball in cavity | Narrow septate hyphae invading tissue |
CD4 of 43 cells/mm³ represents profound immunosuppression (AIDS-defining). At this level, the patient cannot mount any meaningful antifungal host defense, enabling Aspergillus hyphae to invade pulmonary vasculature, cause thrombosis, infarction, and necrosis - the hallmark of IPA.
Pathogenesis of IPA in HIV/AIDS
IPA is characterized by tissue invasion, frequently involving blood vessels. Hyphae within the alveoli penetrate the respiratory mucosa and alveolar capillaries into endothelial cells and pulmonary arterioles. This causes:
- Intravascular thrombosis
- Local hypoxia
- Coagulative necrosis (angioinvasive form)
In the HIV patient, the residual TB cavity served as a portal of entry, but the organism has now gone beyond saprophytic colonization into true invasion. - Murray & Nadel's Respiratory Medicine, p. 1310
Microscopy: Narrow Septate Hyphae
This is the morphologic signature of Aspergillus species (and differentiates it from other molds):
| Feature | Aspergillus | Mucor/Rhizopus |
|---|---|---|
| Hyphae | Narrow (3-6 µm), septate | Broad (10-15 µm), pauci-septate/aseptate |
| Branching | Acute angle (45°) | Right angle (90°) |
| Invasion | Angioinvasive | Also angioinvasive |
The finding of narrow, septate hyphae branching at 45° on tissue microscopy or BAL specimen is a key morphologic clue distinguishing Aspergillus from mucormycosis.
CT: The Halo Sign
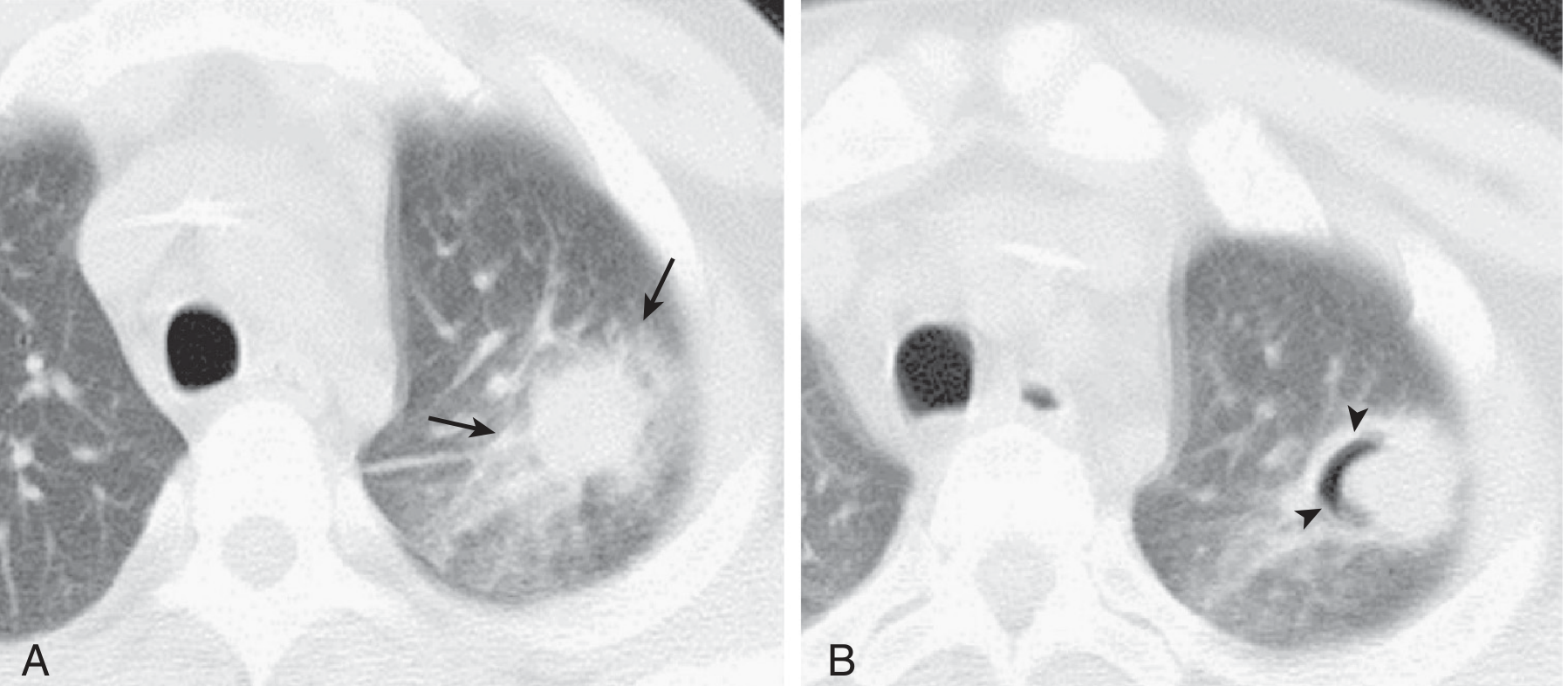
Figure: IPA in CT - (A) poorly defined nodule with surrounding ground-glass opacity = Halo sign, representing central infarction surrounded by hemorrhagic infiltrate. (B) Cavitation developing later = air crescent sign. - Murray & Nadel's Respiratory Medicine, p. 1311
Halo sign mechanism: The central nodule = zone of coagulative infarction/necrosis. The surrounding ground-glass = hemorrhagic infiltration from angioinvasion. This sequence is pathognomonic of angioinvasive fungal infection.
CT evolution in IPA:
- Early: Halo sign (nodule + ground-glass)
- Late: Cavitation → Air crescent sign (as immune reconstitution begins or fungus retracts)
Complete Diagnostic Workup
| Test | Finding/Significance |
|---|---|
| Chest CT | Halo sign (central nodule + GGO) - already present |
| Serum Galactomannan (GM) | Cell wall polysaccharide of Aspergillus; sensitivity/specificity best in neutropenic patients; BAL GM more sensitive than serum in HIV |
| Serum β-D-Glucan | Pan-fungal marker; FDA-approved Fungitell assay (cutoff ≥80 pg/mL); detectable earlier than GM |
| BAL + culture | Sputum cultures positive in >50% of IPA; BAL GM especially useful |
| Aspergillus PCR (BAL/blood) | High sensitivity; combined GM + PCR improves diagnostic yield |
| Tissue biopsy (VATS/CT-guided) | Gold standard for "proven" IPA; shows hyphae invading tissue |
| Aspergillus precipitins (IgG) | Useful in aspergilloma; less reliable in severely immunosuppressed patients (may be falsely negative) |
| CD4 count | 43 - profound immunosuppression, AIDS |
| HIV viral load | Assess ART urgency |
| Blood cultures | Usually negative in IPA; positive in disseminated disease |
| Antifungal susceptibility (MIC) | Perform due to rising azole resistance (cyp51A mutations: TR34/L98H) |
Treatment
First-Line: Voriconazole (IDSA Guideline)
Voriconazole is the FDA-approved first-line therapy for IPA. Treatment must be prompt and aggressive. - Jawetz Medical Microbiology
| Drug | Dose | Notes |
|---|---|---|
| Voriconazole (1st line) | 6 mg/kg IV q12h x 2 doses (loading), then 4 mg/kg IV q12h → step-down to 200-300 mg PO q12h | TDM (therapeutic drug monitoring) recommended; target trough 1-5.5 µg/mL |
| Isavuconazole (alternative 1st line) | 200 mg IV/PO q8h x 6 doses, then 200 mg/day | Non-inferior to voriconazole; fewer adverse effects; preferred if drug interactions problematic |
| Liposomal AmB (L-AmB) (alternative) | 3-5 mg/kg/day IV | For patients intolerant/refractory to azoles; less nephrotoxic than AmB-d |
| Caspofungin (salvage) | 70 mg IV day 1, then 50 mg/day | FDA approved for salvage; echinocandins are fungistatic against Aspergillus |
| Posaconazole (salvage) | 300 mg PO/IV daily | For azole-refractory/intolerant cases; response ~42% |
| Voriconazole + Anidulafungin (combo) | As above | Consider in severe disease/hematologic malignancy; reduces mortality in probable IPA |
Important: In this patient with prior azole exposure (possibly TB treatment), check for azole resistance via susceptibility testing. TR34/L98H mutation in A. fumigatus confers pan-azole resistance. - Murray & Nadel, p. 1313
Additional Management in This HIV Patient
1. Start/Optimize Antiretroviral Therapy (ART)
- CD4 of 43 means ART is urgently needed
- ART initiation timing: generally after 2 weeks of antifungal therapy to avoid IRIS (Immune Reconstitution Inflammatory Syndrome)
- Drug interactions: voriconazole is a CYP2C19/3A4 substrate - significant interactions with ritonavir-boosted regimens; efavirenz induces CYP and reduces voriconazole levels markedly
2. PCP Prophylaxis
- CD4 <200: start trimethoprim-sulfamethoxazole (TMP-SMX)
- CD4 <50: also add azithromycin for MAC prophylaxis
- CD4 <100: consider fluconazole for cryptococcal prophylaxis (especially in high-prevalence settings)
3. Monitor for IRIS
- When ART is started, immune reconstitution may cause paradoxical worsening of IPA
- Characterized by fever, respiratory deterioration, expanding CT lesions despite antifungal therapy
4. Duration of Antifungal Therapy
- Minimum 6-12 weeks; continue until:
- Lesions resolve/stabilize on CT
- CD4 count recovers on ART
- Clinical improvement
Prognosis
IPA in HIV/AIDS with CD4 <50 carries very high mortality if treatment is delayed:
- Untreated: near 100% mortality
- With prompt voriconazole + ART: mortality remains ~30-50%
- Poor prognostic factors: profound immunosuppression (CD4 <50), delayed diagnosis, dissemination to CNS or other sites, azole-resistant Aspergillus, inability to start ART
Summary: Diagnostic Framework
HIV+ (CD4 = 43) + Post-TB cavity
↓
Hemoptysis + narrow septate hyphae + CT halo sign
↓
INVASIVE PULMONARY ASPERGILLOSIS
↓
Confirm: serum/BAL galactomannan + beta-glucan + BAL culture + Aspergillus PCR
↓
Start VORICONAZOLE immediately (don't wait for culture confirmation)
↓
Check susceptibility (azole resistance)
Start ART (after 2 weeks, avoid IRIS)
Prophylax: TMP-SMX + Azithromycin
↓
Monitor: TDM voriconazole, CT at 4-6 weeks, CD4 recovery
A 40 year old man presents with white patches on the side of his tongue
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
Loading Image
Reading File
Reading File
I have all the information needed for a comprehensive answer. Here it is:
White Patches on the Lateral Tongue - 40-Year-Old Man
Most Likely Diagnosis: Oral Hairy Leukoplakia (OHL)
The lateral tongue location is the single most distinguishing clue. OHL almost exclusively arises along the lateral tongue margins (bilateral), and is caused by Epstein-Barr Virus (EBV) replication in the setting of immunosuppression - most commonly HIV/AIDS.
Given the clinical context of prior TB and the previous case's HIV positivity, this is a classic AIDS-defining oral manifestation.
The Appearance

Fig: Oral hairy leukoplakia along the lateral tongue margin showing vertically corrugated keratotic white ridges. - Cummings Otolaryngology, p. 1582
The appearance ranges from:
- Early: Subtle smooth/macular white streaks
- Intermediate: Vertical white keratotic ridges (the "corrugated" pattern)
- Advanced: Thick, shaggy, irregular white surface alterations
The "hairy" name comes from the surface projections giving a hair-like corrugated appearance.
Histopathology

Fig: Low-power histology of OHL - thick parakeratotic surface layer + characteristic pale subsurface layer above spinous layer. - Cummings Otolaryngology, p. 1582
Microscopic features:
- Hyperkeratosis with irregular surface projections
- Ballooning degeneration of subsurface keratinocytes
- Nuclear "beading" - chromatin displacement to inner nuclear membrane by viral replication
- Confirmed by in situ hybridization or PCR demonstrating EBV
Differential Diagnosis of White Tongue Patches
| Diagnosis | Location | Key Features | Scrape Test |
|---|---|---|---|
| Oral Hairy Leukoplakia (top dx) | Lateral tongue bilaterally | Corrugated/vertical ridges; EBV; HIV marker | Cannot be scraped off |
| Pseudomembranous Candidiasis (Thrush) | Anywhere; dorsum, buccal | Curd-like white plaques; erythematous base | Scrapes off leaving raw surface |
| Hyperplastic Candidiasis | Buccal mucosa | Thick white plaque; rarest form | Cannot be scraped off |
| Simple Leukoplakia | Buccal mucosa, floor of mouth | Homogeneous white patch; premalignant; no EBV | Cannot be scraped off |
| Oral Lichen Planus | Posterior buccal mucosa | Reticular/lacy white striae (Wickham's striae); may be erosive | Cannot be scraped off |
| Squamous cell carcinoma | Lateral tongue, floor of mouth | Indurated, ulcerated, fixed; mixed red-white | Fixed, indurated |
The Single Most Important Bedside Test:
Can the white patch be scraped off?
- Yes (leaves raw/bleeding base) = Candidiasis (thrush)
- No = OHL, leukoplakia, lichen planus, or carcinoma
How to Confirm OHL
| Test | Purpose |
|---|---|
| Clinical appearance alone | Often sufficient - lateral tongue + corrugated white patches + HIV+ |
| Biopsy + in situ hybridization for EBV | Gold standard - demonstrates EBV DNA in epithelial cells |
| EBV PCR or Southern blot | Confirmatory |
| KOH preparation / PAS stain | Rules out Candida (negative in OHL) |
| HIV test + CD4 count | OHL is a marker of immunosuppression - must be investigated |
OHL is an AIDS-defining illness in the correct context. Its presence in any patient without a known cause of immunosuppression is an indication to test for HIV immediately.
Clinical Significance of OHL
- Caused by EBV (not Candida, not a premalignant lesion - no malignant potential)
- It is asymptomatic - patients usually notice the white patches incidentally
- It is not painful (contrast with candidiasis which may burn, or erosive lichen planus which ulcerates)
- It is strongly associated with CD4 <200 - the lower the CD4, the more extensive the lesion
- In HIV patients, it is a clinical marker that immunosuppression is significant and ART is needed
- Less commonly seen in: organ transplant recipients, hematologic malignancy, other causes of immunosuppression (can occur even in HIV-negative immunosuppressed individuals)
Management
| Scenario | Management |
|---|---|
| HIV+, on ART | OHL typically disappears with effective ART and CD4 recovery - no specific treatment needed |
| Symptomatic/cosmetically distressing | Topical podophyllum resin, topical retinoids, or acyclovir/valacyclovir (EBV antiviral) |
| OHL + not yet on ART | Initiate ART - lesion will resolve as CD4 recovers |
| Candidiasis (if co-existing) | Topical nystatin (CD4 >200) or systemic fluconazole (CD4 <200) |
The key management principle: establishing the diagnosis is the most important step. If OHL is confirmed and HIV is the cause, the treatment is ART - not antifungal therapy. - Cummings Otolaryngology, p. 1582
Summary in Context
Given this patient's profile (40-year-old man, HIV+, CD4 = 43, prior TB):
- The white lateral tongue patches are almost certainly Oral Hairy Leukoplakia (EBV-driven)
- Co-existing oral candidiasis is also highly likely at CD4 = 43 (the two often co-exist)
- Both resolve with ART initiation and CD4 recovery
- The lesion carries no malignant risk but is a powerful marker of immune failure
This is a shared conversation. Sign in to Orris to start your own chat.