Breast milk jaundice
Reading File
Finding Sources
Finding Sources
Searching PubMed
"breast milk jaundice" neonatal hyperbilirubinemia
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
What is breast milk jaundice ?
I have all the information needed from the previous research. Here is a comprehensive answer.
Breast Milk Jaundice
Definition
Breast milk jaundice (BMJ) is a prolonged unconjugated (indirect) hyperbilirubinemia occurring in healthy, well-fed breastfed neonates, typically appearing after the first week of life and persisting for several weeks to months. It is the second most common cause of neonatal jaundice overall.
Pathophysiology
The exact mechanism is not fully established, but several factors are proposed:
-
Glucuronyl transferase inhibition - Certain fatty acids and other substances present in breast milk inhibit UGT1A1 (hepatic UDP-glucuronosyltransferase), the enzyme responsible for bilirubin conjugation. This impairs the conversion of unconjugated bilirubin to its water-soluble form.
-
Increased enterohepatic circulation - Breast milk contains beta-glucuronidases, which deconjugate bilirubin in the gut, allowing its reabsorption back into the circulation, raising unconjugated bilirubin levels.
-
Hormonal mediation - Some evidence suggests a hormonally mediated mechanism, though this is less well defined.
It differs from Lucey-Driscoll syndrome (transient familial neonatal hyperbilirubinemia), where a UGT1A1 inhibitor is found in maternal serum, not breast milk.
Clinical Features
| Feature | Details |
|---|---|
| Onset | Typically after day 4-7 of life (later than physiologic jaundice) |
| Peak bilirubin | 10-27 mg/dL, peaking around days 10-21 of life |
| Duration | May persist for 3-10 weeks, occasionally longer |
| Bilirubin type | Unconjugated (indirect) only |
| Infant appearance | Well-appearing, healthy, gaining weight adequately |
| Pattern | Gradual rise, similar to physiologic jaundice but levels continue to climb beyond day 5 |
Distinction from Breastfeeding (Starvation) Jaundice
This is a critical distinction:
| Breast Milk Jaundice | Breastfeeding Jaundice | |
|---|---|---|
| Also called | BMJ | Starvation jaundice |
| Timing | After 1st week | Days 2-4 |
| Cause | Substances in milk | Inadequate intake, dehydration |
| Infant weight | Normal | Weight loss / poor gain |
| Mechanism | Inhibition of conjugation / enterohepatic recirculation | Decreased gut motility, less meconium passage, increased reabsorption |
| Treatment | Monitor, phototherapy if needed | Improve feeding frequency and technique |
Diagnosis
- BMJ is a diagnosis of exclusion - pathologic causes must be ruled out first.
- Check total and direct (fractionated) bilirubin - direct fraction should be normal (conjugated hyperbilirubinemia is always pathologic).
- Conjugated bilirubin is normal in BMJ.
- Transcutaneous bilirubin meters can screen but do not differentiate conjugated from unconjugated.
- Additional workup if needed: CBC with smear, Coombs test, blood group, thyroid function, G6PD levels.
Red flags requiring further evaluation (Box 166.1 - Rosen's):
- Jaundice within first 24 hours of life
- Elevated direct/conjugated bilirubin
- Rapidly rising TSB unexplained by history
- TSB approaching exchange transfusion levels or not responding to phototherapy
- Jaundice persisting beyond 3 weeks of age
- Sick-appearing infant
Management
-
Continue breastfeeding - Feeding stimulates gut motility, reduces enterohepatic circulation, and lowers bilirubin. Breastfeeding should NOT be stopped routinely.
-
Monitor bilirubin levels closely to ensure levels are not rising toward the phototherapy threshold.
-
Phototherapy - Initiated based on the AAP phototherapy nomogram (see chart below), which stratifies by age (hours) and risk category:
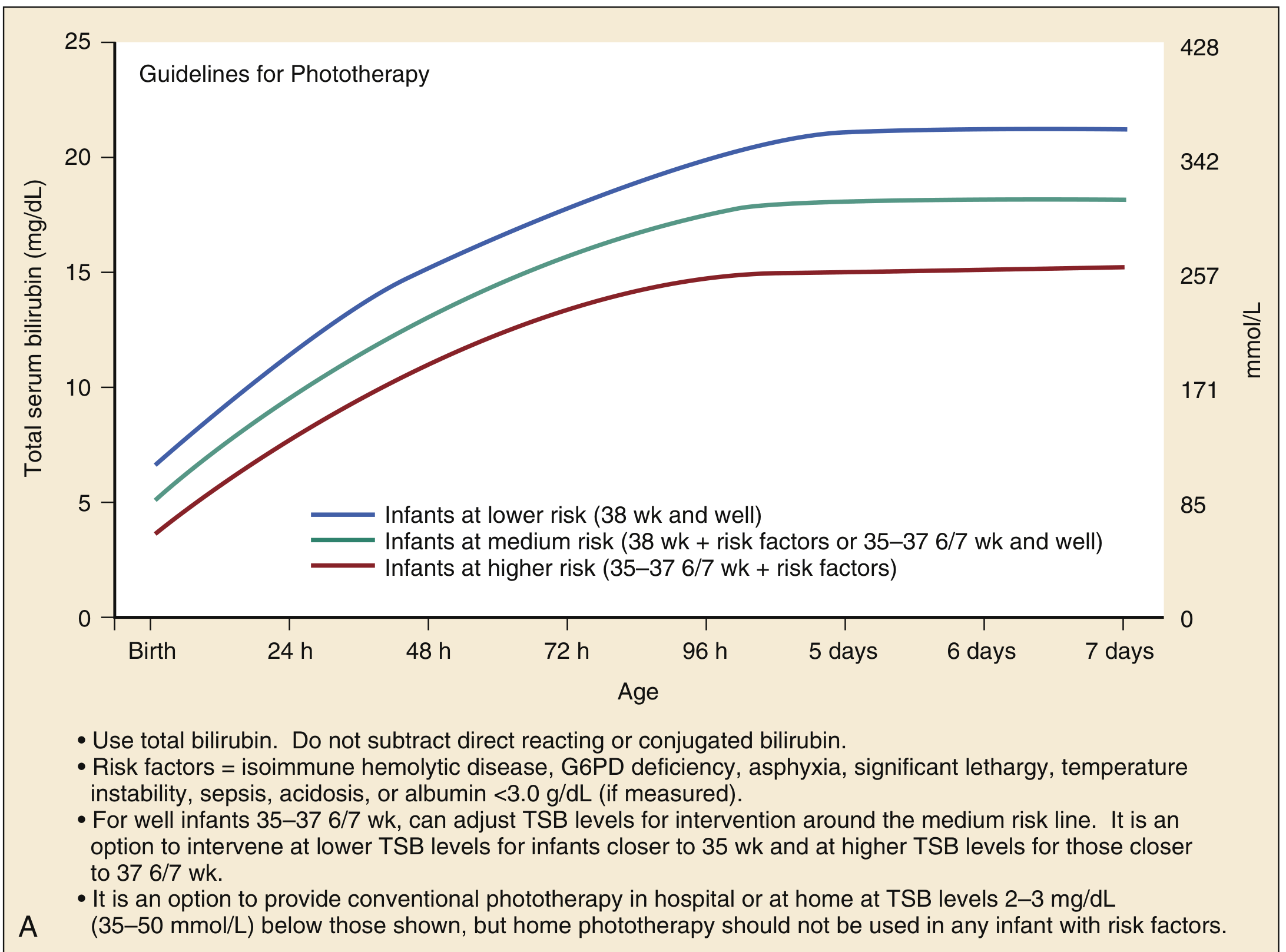
- Lower risk infants (≥38 wks, well): higher bilirubin threshold before phototherapy
- Medium risk (≥38 wks + risk factors, or 35-37 6/7 wks, well)
- Higher risk (35-37 6/7 wks + risk factors): phototherapy at lower bilirubin levels
- Risk factors include: isoimmune hemolytic disease, G6PD deficiency, asphyxia, lethargy, temperature instability, sepsis, acidosis, albumin <3.0 g/dL
-
Temporary interruption of breastfeeding - Occasionally used as a diagnostic test; bilirubin drops significantly within 24-48 hours if BMJ is the cause. However, this is generally not recommended as a routine intervention given the benefits of breastfeeding.
-
Exchange transfusion - Reserved for severely elevated bilirubin levels not responding to phototherapy, to prevent kernicterus.
Complications if Untreated (Hyperbilirubinemia in General)
At bilirubin levels generally >20-25 mg/dL, unconjugated bilirubin crosses the blood-brain barrier, causing:
- Bilirubin-Induced Neurologic Dysfunction (BIND) - acute phase: poor feeding, somnolence, hypertonia/hypotonia, high-pitched cry
- Acute Bilirubin Encephalopathy (ABE) - progresses to lethargy, opisthotonos, retrocollis, seizures, apnea, death
- Kernicterus - chronic, irreversible sequelae: cerebral palsy, sensorineural hearing loss, upward gaze palsy, intellectual disability
Key Points Summary
- BMJ = unconjugated hyperbilirubinemia in healthy breastfed neonates, appearing after the first week
- Caused by glucuronyl transferase inhibition and/or increased enterohepatic circulation from substances in breast milk
- Peaks at 10-27 mg/dL around week 2-3, may persist up to 3 months
- Always check fractionated bilirubin - direct fraction must be normal
- Continue breastfeeding; use phototherapy per AAP nomogram when thresholds are reached
- Kernicterus is preventable with timely treatment
Sources: Rosen's Emergency Medicine 9e, Harrison's Principles of Internal Medicine 22e (2025), Tintinalli's Emergency Medicine, Textbook of Family Medicine 9e, Harriet Lane Handbook 23e, Robbins Pathologic Basis of Disease
Foot burns causes
Reading File
Finding Sources
Finding Sources
Searching the Web
foot burns causes types thermal chemical electrical clinical
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
I now have rich material from multiple authoritative sources. Let me compile a thorough, well-organized answer.
Causes of Foot Burns
Foot burns arise from a wide variety of mechanisms. Understanding the cause is clinically important because it determines depth, extent, treatment strategy, and prognosis. Burns can be classified by the causative agent into the following categories:
1. Thermal Burns (Most Common)
Thermal burns result from exposure to external heat sources that raise skin and tissue temperature, causing cell death or charring. The foot is particularly vulnerable because it is often unprotected.
a) Scald Burns (Hot Liquids / Steam)
- The most common burn injury in young children
- Caused by: boiling water, hot tea/coffee, hot cooking oil, steam
- Can affect the feet when liquids are spilled or the foot is immersed (e.g., stepping into hot bathwater)
- Tend to produce partial-thickness (2nd degree) wounds with a relatively uniform depth
b) Flame / Flash Burns
- Direct contact with open flames (house fires, campfires, gas explosions)
- Flash burns from sudden ignition of flammable vapors (e.g., petrol, gas leaks)
- More common in teenagers and adults
- Often involve the dorsum of the foot and lower limbs
- Can be deep partial- or full-thickness
c) Contact Burns
- Direct contact of the foot with a hot surface - hot pavement/asphalt in summer, hot metal objects, heaters, stoves, radiators, exhaust pipes
- A common occupational and domestic injury
- Walking barefoot on hot surfaces (e.g., hot sand, hot asphalt) is a classic mechanism
- Tend to be well-demarcated, often full-thickness at the contact point
d) Tar / Asphalt Burns
- Stepping into or contact with hot tar or molten asphalt (occupational hazard in road construction)
- Tar adheres to the skin and retains heat, deepening the injury
- Removal of tar should be done carefully (mineral oil / petroleum-based solvents), not by forceful pulling
2. Scald Burn - Special Mention: Immersion Burns (Child Abuse)
- Forced immersion of a child's feet/legs into hot water as a form of non-accidental injury
- Produces a characteristic "stocking distribution" burn with a clear waterline demarcation
- Should raise high suspicion for child abuse
- Uniform depth, sharp margins, no splash marks (distinguishes from accidental scalds)
3. Chemical Burns
Caused by strong acids, alkalis, or other corrosive substances coming into contact with the skin of the foot.
| Agent | Examples | Notes |
|---|---|---|
| Acids | Sulfuric acid, hydrochloric acid, nitric acid, battery acid | Cause coagulative necrosis; self-limiting as eschar forms |
| Alkalis | Sodium hydroxide (drain cleaners), cement, lime | Cause liquefactive necrosis; penetrate deeper; more destructive |
| Solvents | Industrial chemicals, petroleum products | Can dissolve lipid-rich tissue |
| Oxidizing agents | Bleach, hydrogen peroxide | Cause oxidative cellular damage |
| Cement burns | Portland cement (alkali) | A classic occupational foot burn - wet cement inside boots |
- Chemical burns are progressive until the agent is fully diluted/neutralized
- First aid: immediate and prolonged irrigation with water
- Alkali burns are generally more severe than acid burns
4. Electrical Burns
- Electrical current enters through a contact point and exits through another (entry and exit wounds)
- The foot is a common exit point for electrical injuries (current travels through the body to ground)
- Types:
- Low voltage (<1000 V): household current (AC), often produces localized contact burns
- High voltage (>1000 V): industrial/power lines; can cause extensive deep tissue necrosis, rhabdomyolysis, renal failure
- Lightning strikes: massive flash of current; entry and exit burns on feet/hands are common
- The full extent of damage may not be apparent at first presentation - deep tissue destruction can be far greater than the surface wound suggests
- May require fasciotomy or even amputation
5. Radiation Burns
- Sunburn: prolonged ultraviolet (UV) exposure to bare feet - causes erythema, blistering (superficial to partial thickness)
- Therapeutic radiation: radiation therapy to lower limb tumors can cause radiation dermatitis on the foot
- Radiation accidents: industrial or nuclear exposure (rare)
6. Friction Burns
- Caused by skin rubbing against a rough surface at speed
- Common in: road traffic accidents (motorcyclists, pedestrians - "road rash"), sports injuries
- Also seen with ill-fitting shoes/prosthetics causing shear forces
- Typically superficial but can be deep over bony prominences
7. Cold Burns (Frostbite) - Thermal Injury by Extreme Cold
Though technically a "cold injury," frostbite causes tissue destruction by similar mechanisms to heat burns:
- Direct injury from ice crystal formation in extracellular fluid
- Ischemic injury from vascular endothelial damage, clot formation, and increased sympathetic tone
- The foot is one of the most commonly affected sites (toes, heel)
- Risk groups: high-altitude climbers, skiers, hunters, homeless individuals, alcoholics
8. Inhalation Burns - Indirect Foot Involvement
In large burns with inhalation injury (e.g., house fires), the feet may be involved as part of multi-site burns. The systemic effects (fluid shifts, edema, compartment syndrome) can affect the extremities even if the foot was not the primary contact site.
Summary Table of Foot Burn Causes
| Category | Specific Cause | Key Feature |
|---|---|---|
| Thermal - Scald | Hot water, steam, cooking oil | Most common in children; uniform depth |
| Thermal - Flame | Fire, gas explosion | Full-thickness; flash burns possible |
| Thermal - Contact | Hot pavement, metal, exhaust | Well-demarcated; occupational/barefoot |
| Thermal - Tar | Hot asphalt/tar | Adheres to skin; deep injury |
| Thermal - Immersion | Forced hot water | Stocking pattern; suspect child abuse |
| Chemical - Acid | Battery acid, industrial acids | Coagulative necrosis; self-limiting |
| Chemical - Alkali | Cement, NaOH, lime | Liquefactive necrosis; progressive |
| Electrical | Entry/exit wound | Deep tissue injury; may not be obvious |
| Radiation | UV, therapeutic radiation | Sunburn; radiation dermatitis |
| Friction | Road rash, shear | Superficial; sports/traffic accidents |
| Cold (Frostbite) | Freezing temperatures | Ice crystal + ischemic injury; toes |
Clinical Note on Depth Classification
Regardless of cause, burns are classified by depth:
- Superficial (1st degree): epidermis only - erythema, no blisters (e.g., mild sunburn)
- Partial-thickness (2nd degree): epidermis + part of dermis - blistering, painful
- Full-thickness (3rd degree): full skin destruction - leathery, painless, requires grafting
- 4th degree: extends to subcutaneous tissue, muscle, or bone (typically electrical or prolonged contact burns)
The foot and hand are functionally critical areas - burns here are considered special area burns requiring specialized burn center care due to the risk of contracture, impaired mobility, and long-term functional loss.
Sources: Current Surgical Therapy 14e, Sabiston Textbook of Surgery, Campbell's Operative Orthopaedics 15e (2026), Bailey and Love's Surgery 28e, Stanford Health Care, UCLA Health
Patient is 55 years old with complain of burning sensation on dorsum of foot .he has history of gerd and know case of prosthetic hypertrophy.
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Searching the Web
55 year old burning sensation dorsum foot GERD prostatic hypertrophy differential diagnosis neuropathy
Reading File
Finding Sources
Reading File
Searching the Web
BPH medications alpha blockers 5-alpha reductase inhibitors peripheral neuropathy burning feet side effects
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.