Mi ka management batao pura
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Loading Image
Reading File
Ab mere paas poora comprehensive content hai. Final answer likhta hoon:
Myocardial Infarction (MI) - Pura Management
Overview (STEMI vs NSTEMI)
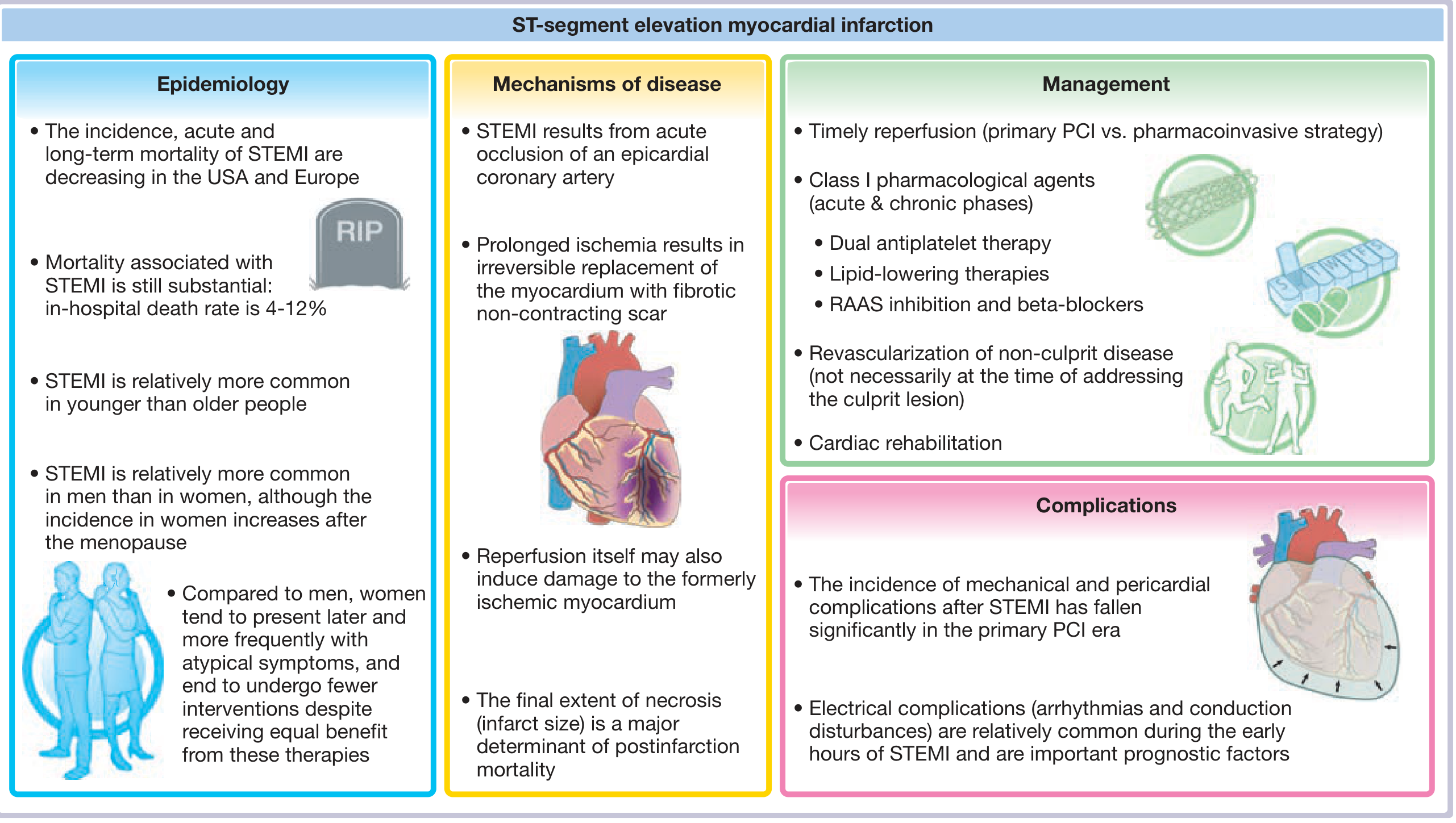
MI do types ka hota hai:
- STEMI - ST-segment elevation MI (complete coronary occlusion)
- NSTEMI - Non-ST-elevation MI (partial occlusion, enzyme raise hoti hai)
STEP 1 - Immediate / Upstream Therapy (Sabse Pehle)
Jab bhi MI suspect ho, turant ye drugs deni chahiye:
| Drug | Dose | Note |
|---|---|---|
| Aspirin (ASA) | 162-325 mg chew karke | Sabko dena hai, contraindication na ho to |
| P2Y12 inhibitor (clopidogrel/ticagrelor/prasugrel) | Loading dose | Ticagrelor: 180 mg load, fir 90 mg BD |
| Anticoagulant (UFH/LMWH) | UFH: 60 units/kg IV bolus + 12 units/kg/h | Thrombolysis ya PCI dono ke saath |
| Nitroglycerin | 0.4 mg sublingual, har 5 min mein 3 baar | Hypotension ho to mat do |
| Oxygen | Sirf agar hypoxic ho (SpO2 <90%) | Routine oxygen band kar di gayi hai |
| Beta-blocker (Metoprolol) | 25 mg PO | HF, shock, advanced AV block, bronchospasm mein AVOID |
| Morphine | Pain ke liye | Caution - ongoing ischemia symptoms mask kar sakta hai |
STEP 2 - Reperfusion Strategy (STEMI Ke Liye Sabse Zaroori)
Reperfusion = STEMI ka cornerstone treatment hai. Baaki sab secondary hai.
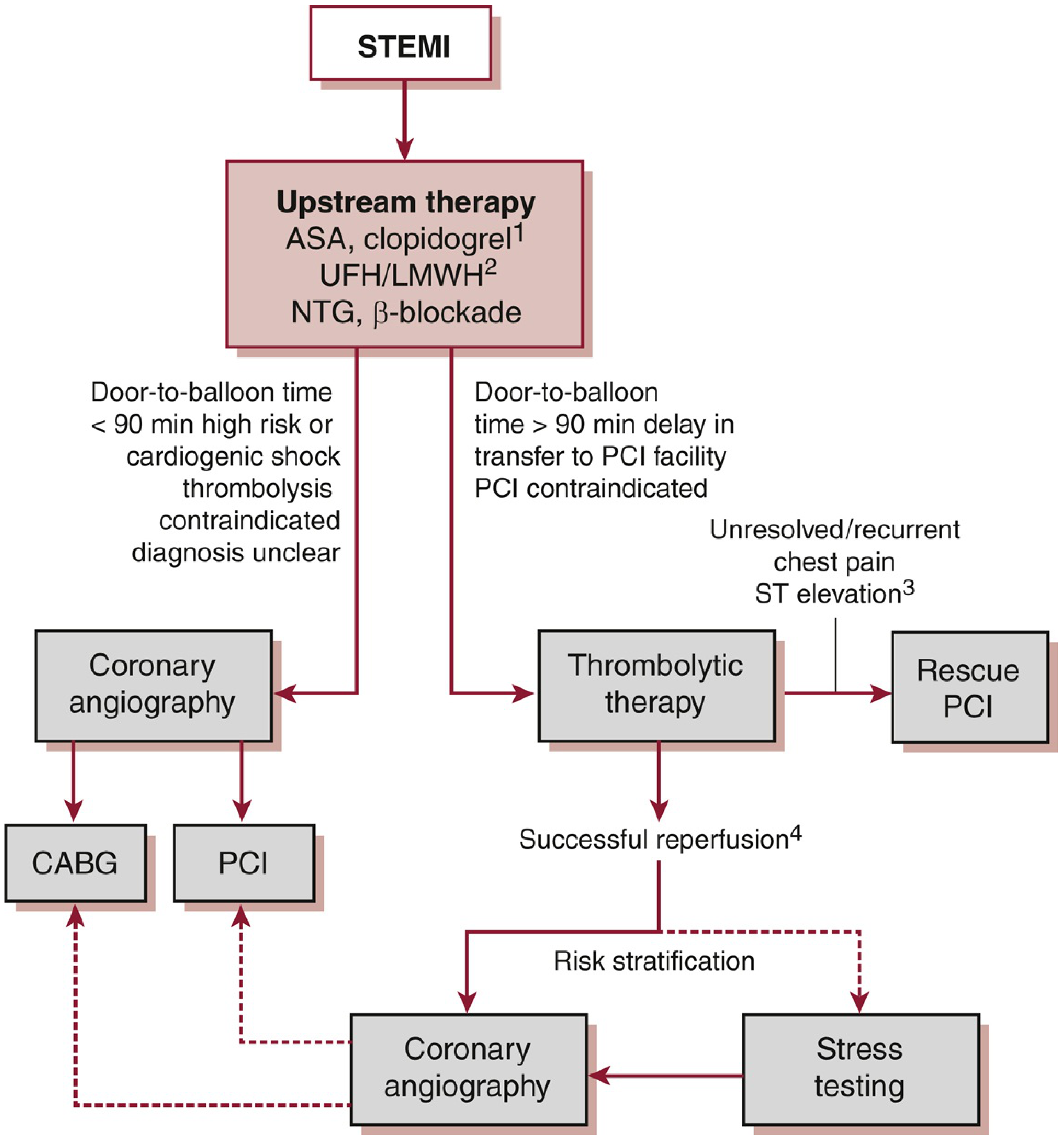
Option A - Primary PCI (Preferred)
- Door-to-balloon time < 90 minutes mein available ho to PCI hi karo
- PCI > thrombolysis kyunki:
- Better vessel patency (TIMI 3 flow)
- Kam reinfarction
- Hemorrhagic stroke ka risk bahut kam
- Improved survival
- Symptom onset se 12 hours ke andar sabse effective
Option B - Thrombolysis (Jab PCI 90-120 min mein available na ho)
Drugs:
- Alteplase (rt-PA): 15 mg IV bolus, fir 0.75 mg/kg 30 min, fir 0.5 mg/kg 60 min
- Reteplase: Do 10-unit IV boluses, 30 min apart
- Tenecteplase (TNK): 0.5 mg/kg single IV bolus
Thrombolysis ke baad:
- Chest pain relief + >50% ST reduction at 90 min = successful reperfusion
- Reperfusion arrhythmia (accelerated idioventricular rhythm) bhi sign hai
- Sab patients ko 24 hours mein coronary angiography ke liye refer karo
Thrombolysis Contraindications (Absolute):
- Intracranial hemorrhage history
- Ischemic stroke 3 months ke andar
- Aortic dissection
- Active bleeding
- Severe uncontrolled HTN (SBP >180 / DBP >110)
- Acute pericarditis
STEP 3 - Antiplatelet & Anticoagulation Detail
Antiplatelet (DAPT - Dual Antiplatelet Therapy):
- ASA lifelong 81 mg/day (PCI ke baad)
- P2Y12 inhibitor sath dena hai:
- Ticagrelor 90 mg BD (clopidogrel se better, mortality benefit)
- Prasugrel (PCI ke liye)
- Clopidogrel (sirf thrombolysis ke sath use karo)
Anticoagulants:
| Drug | Dose | Note |
|---|---|---|
| UFH | 60 units/kg bolus + 12 units/kg/h | PCI aur thrombolysis dono mein |
| Enoxaparin (LMWH) | 30 mg IV bolus, fir 1 mg/kg SC BD | >75 years: bolus nahi, 0.75 mg/kg SC |
| Bivalirudin | 0.75 mg/kg bolus + 1.75 mg/kg/h | Sirf PCI mein validated |
| Fondaparinux | 2.5 mg IV, fir 2.5 mg SC daily | Thrombolysis mein preferred, PCI mein catheter thrombosis risk |
STEP 4 - Peri-Infarct / CCU Management
- CCU mein admit karo - minimum 24 hours telemetry monitoring
- Daily assessment: chest pain, HF symptoms, ECG
- Echocardiogram (ECHO) baseline lena zaroori:
- EF check karo
- Wall motion abnormality
- Valvular lesions
- Ventricular thrombus
- Pacing: AV block aane par - inferior wall MI mein transient hota hai, anterior wall MI mein unstable ho sakta hai (temp pacemaker laga sakte hain)
STEP 5 - Secondary Prevention (Long-Term, Discharge Ke Baad)
Ye medicines survival improve karti hain:
| Drug | Purpose |
|---|---|
| Aspirin 81 mg lifelong | Antiplatelet |
| P2Y12 inhibitor (1 year tak DAPT) | Post-stenting |
| Beta-blocker (Metoprolol/Carvedilol) | Mortality benefit, LV remodeling rokta hai |
| ACE inhibitor / ARB | Post-MI, especially LV dysfunction mein |
| High-intensity Statin | LDL <70 mg/dL target |
| GPIIb/IIIa inhibitor | Sirf PCI + stenting mein |
NSTEMI / Unstable Angina (UA) Management
NSTEMI mein thrombolysis NAHI dete - ST depression mein contraindicated hai.
- DAPT + anticoagulant dena hai
- Risk stratification karo (TIMI score / HEART score)
- Early invasive strategy (coronary angiography within 24-48 hours)
Complications Jo Monitor Karni Hain
- Arrhythmias (afib, VT, VF) - sabse common early complication
- Cardiogenic shock - intra-aortic balloon pump / vasopressors
- Mechanical complications - papillary muscle rupture (severe MR), VSD, free wall rupture (emergency CABG)
- Ventricular aneurysm
- Dressler's syndrome (post-MI pericarditis)
Yaad Rakhne Ka Formula (Mnemonic) - "MONA + DAPT + Reperfusion"
| Letter | Meaning |
|---|---|
| M | Morphine (pain ke liye) |
| O | Oxygen (sirf hypoxia mein) |
| N | Nitrates |
| A | Aspirin |
| DAPT | Dual Antiplatelet Therapy |
| Reperfusion | PCI first choice, thrombolysis second |
Sources: Washington Manual of Medical Therapeutics, p.152-160 | Symptom to Diagnosis, 4th Ed., p.175 | Fuster & Hurst's The Heart, 15th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.