Interventional therapy for treatment of copd/emphysema for md exams 10 marks answer from fishman and murray only
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
I now have all the material needed for a comprehensive 10-mark exam answer. Let me compose the full answer.
Interventional Therapy for COPD/Emphysema
(From Fishman's Pulmonary Diseases and Disorders, 5e and Murray & Nadel's Textbook of Respiratory Medicine, 7e)
Introduction
For patients with far-advanced COPD/emphysema who fail maximal medical therapy, interventional options fall into three broad categories: (1) bronchoscopic lung volume reduction, (2) surgical lung volume reduction, and (3) lung transplantation. These aim to reduce dynamic hyperinflation, improve elastic recoil, optimize respiratory muscle mechanics, and improve quality of life.
1. Bronchoscopic Lung Volume Reduction (BLVR)
The morbidity and mortality (~5% procedural death rate) of surgical lung volume reduction surgery (LVRS) demonstrated in the National Emphysema Treatment Trial (NETT) drove development of minimally invasive bronchoscopic approaches with comparable physiologic efficacy but less perioperative risk. (Fishman's, p. 659)
A. Endobronchial Valves (EBVs)
EBVs are the most extensively studied and FDA-approved modality.
Mechanism: One-way valves that allow air and secretions to exit the targeted emphysematous lung segment, while preventing air reentry - causing progressive lobar deflation, reducing total lung volume, residual volume (RV), and dynamic hyperinflation. (Murray & Nadel, p. 665)
Two FDA-approved devices:
- Zephyr valve (PulmonX) - umbrella-type duckbill valve
- Intrabronchial Valve / Spiration valve (IBV; Olympus) - approved December 2018
Key prerequisite - Collateral Ventilation Assessment:
The benefit of EBVs depends critically on the absence of collateral ventilation to the target lobe. Intact interlobar fissures are required. The Chartis system (PulmonX) is a bronchoscopic tool with ~75% accuracy in predicting clinical improvement after lobar occlusion. (Murray & Nadel, p. 665)
Evidence:
-
LIBERATE trial (Zephyr valve): Randomized multicenter study in severe heterogeneous emphysema. Inclusion required: minimal/no collateral ventilation, RV >175%, significant hyperinflation, upper lobe-predominant heterogeneous emphysema. Results: 47.7% of EBV patients vs. 16.8% controls achieved ≥15% improvement in post-bronchodilator FEV1 (P <0.001). Significant improvement in 6-minute walk distance (6MWD) and St. George's Respiratory Questionnaire (SGRQ). Pneumothorax occurred in 26.5% (all within first 45 days). (Murray & Nadel, p. 666)
-
EMPROVE trial (IBV/Spiration valve): Randomized multicenter study using CT fissure integrity to assess collateral ventilation. Achieved primary endpoints - valve approved by FDA December 2018. (Murray & Nadel, p. 666)
Patient selection for EBVs: (Fishman's, p. 659-660)
- Significant air trapping: RV >175%
- Hyperinflation present
- Heterogeneous, upper lobe-predominant emphysema (though some benefit in homogeneous disease)
- Intact lobar fissures / no collateral interlobar ventilation
Outcome after successful EBV placement: Patients achieving complete atelectasis of the target lobe have the best symptomatic and survival outcomes. Pneumothorax (a known complication) usually occurs in the first 45 days. (Fishman's, p. 660)
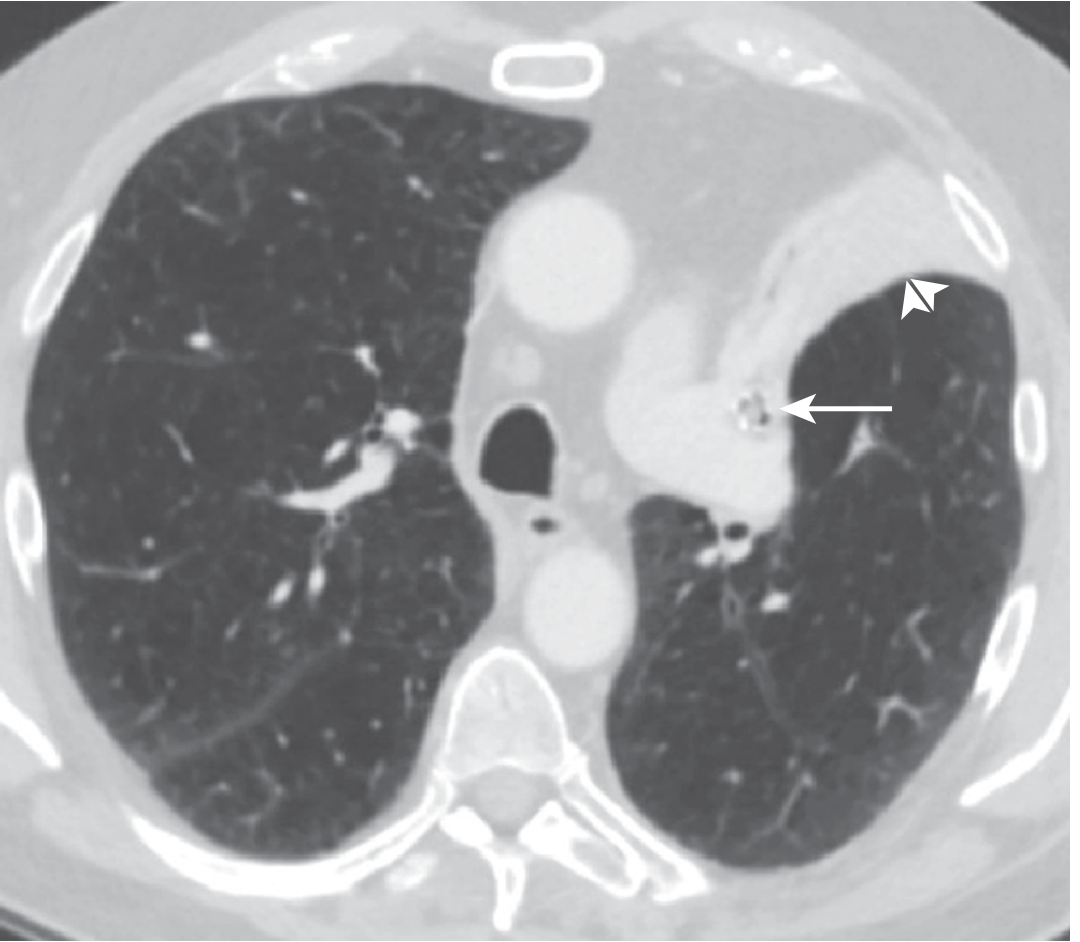
Figure: Complete left upper lobe collapse after endobronchial valve placement in a COPD patient. (Murray & Nadel's, Fig. 28.5)
B. Bronchial Lung Volume-Reduction Coils (LVR Coils)
Device: PneumRx coil - made of nitinol wires. Deployed bronchoscopically into the target bronchus; upon deployment the coil retracts and physically folds the emphysematous parenchyma, reducing lung volume. (Murray & Nadel, p. 666)
Advantage over EBVs: Success is independent of collateral ventilation - coils work even with fissure incompleteness.
Evidence - RENEW trial (multicenter, randomized Phase III): Patients with severe emphysema and severe air trapping. Primary endpoint: absolute change in 6MWD at 12 months. Results: modest, statistically significant improvement in exercise tolerance. However, higher likelihood of major complications (pneumonia, hospitalizations, potentially fatal events). Not approved by FDA (available in Europe). (Murray & Nadel, p. 666-667)
C. Biologic Sealant (AeriSeal)
A synthetic polymeric foam sealant applied bronchoscopically directly into emphysematous segments. Causes direct alveolar collapse.
- Fissure integrity less critical since sealant blocks collateral ventilation sites directly.
- Initial studies showed improvements in pulmonary function, exercise capacity, and quality of life.
- The pivotal ASPIRE trial was terminated for financial reasons. (Murray & Nadel, p. 667)
D. Bronchoscopic Thermal Vapor Ablation
Steam water vapor delivered at precise temperature via a specialized catheter directly into target lung segments. Induces a localized inflammatory response causing fibrosis and permanent atelectasis - complete and permanent lung volume reduction.
- Independent of collateral ventilation (like coils and sealant)
- Preliminary studies showed improvements in pulmonary function and quality of life. (Murray & Nadel, p. 667)
E. Complications of Bronchoscopic LVR
The most important complications, as summarized in Murray & Nadel:
- Pneumothorax (most serious and common with EBVs; 26.5% in LIBERATE)
- Transient reductions in lung function
- Flares of bronchitis or pneumonia
Reversibility: EBV placement is reversible. Coil placement, biologic sealant, and thermal vapor ablation are irreversible. (Murray & Nadel, p. 667)
2. Bronchoscopic Airway Therapies (Airway-Dominant COPD)
These target airway inflammation and peripheral airway resistance (rather than volume reduction). (Fishman's, p. 660)
A. Targeted Lung Denervation (TLD)
A bronchoscopic adaptation of surgical vagotomy (used in 1930s-1950s for airway disease). A dual-cooled radiofrequency (RF) catheter ablates parasympathetic nerves along the outer surface of the bilateral mainstem bronchi, reducing cholinergic bronchoconstriction.
- AIRFLOW trial (first RCT): TLD-treated patients had significantly fewer respiratory adverse events between 3-6.5 months post-randomization vs. sham bronchoscopy. A larger multicenter trial is underway. (Fishman's, p. 660)
B. Cryospray (for Chronic Bronchitis Phenotype)
Metered liquid nitrogen delivered bronchoscopically at -196°C into lobar and segmental airways. Rapid epithelial freezing preserves the extracellular matrix, allowing repopulation with fewer goblet cells - reducing mucus hypersecretion without scarring. Two small proof-of-concept studies confirmed safety; pivotal US trial underway. (Fishman's, p. 660)
3. Lung Volume Reduction Surgery (LVRS)
The NETT (National Emphysema Treatment Trial) - a landmark landmark collaborative study of 1218 patients with severe emphysema comparing LVRS vs. maximal medical treatment - defines current patient selection. (Murray & Nadel, p. 2019-2020)
Procedure: Bilateral stapled resection of 20-30% of lung, usually from the apices, via median sternotomy or VATS (equally safe and effective). (Fishman's, p. 659; block8)
Physiologic rationale:
- Remaining lung expands to fill the thorax, increasing elastic recoil pressure, improving expiratory airflow
- Reduces hyperinflation - diaphragm returns to normal domed configuration, improving mechanical efficiency
- Preferential removal of unventilated bullae reduces RV, increasing vital capacity
NETT outcomes and current selection criteria:
| Patient Group | LVRS Outcome |
|---|---|
| Upper lobe predominant emphysema + low exercise capacity | Improved survival, quality of life - best candidates |
| Upper lobe predominant + adequate exercise capacity | Improved quality of life but no survival benefit |
| FEV1 ≤20% predicted + DLco ≤20% predicted OR homogeneous emphysema | High surgical mortality - LVRS contraindicated |
| Lower lobe predominant + adequate exercise capacity | Worse outcomes after LVRS |
(Murray & Nadel, p. 2020; Fishman's, p. 659)
Contraindications to LVRS (Fishman's):
- FEV1 <20% predicted with DLco <20% predicted
- Diffuse homogeneous emphysema on HRCT
Bullectomy: Surgical resection of a single large bulla is rarely indicated for COPD treatment. Isolated giant bullae are usually congenital. Accepted indication: bulla occupying >1/3 of hemithorax with compression of normal lung. A preserved DLco suggests greater likelihood of improvement. (Fishman's, block8)
Rehabilitation: Pulmonary rehabilitation is required both before LVRS (to optimize functional status and baseline function) and after surgery (to facilitate adaptation to new functional level). (Fishman's, block9)
4. Lung Transplantation
For younger patients with advanced disease where LVRS is not suitable.
Referral criteria for lung transplantation in COPD (Fishman's, block8):
- FEV1 <25% predicted
- BODE index >5
- Hypercapnia
- Resting hypoxemia
- Secondary pulmonary hypertension
- Accelerating decline in FEV1
- Age <65 years
Summary Table
| Intervention | Mechanism | Key Evidence | Notes |
|---|---|---|---|
| EBV (Zephyr/Spiration) | One-way valve → lobar deflation | LIBERATE, EMPROVE | Requires intact fissures, no collateral ventilation; reversible |
| LVR Coils (PneumRx) | Mechanical compression of emphysematous parenchyma | RENEW | Works with collateral ventilation; FDA not approved (Europe only) |
| Biologic Sealant (AeriSeal) | Direct alveolar collapse | ASPIRE (terminated) | Blocks collateral ventilation sites |
| Thermal Vapor Ablation | Steam → fibrosis → permanent atelectasis | Preliminary studies | Irreversible; no collateral ventilation needed |
| Targeted Lung Denervation | RF ablation of parasympathetic nerves | AIRFLOW trial | For airway-dominant COPD phenotype |
| Cryospray | Freeze → fewer goblet cells | Proof-of-concept | For chronic bronchitis phenotype |
| LVRS | Stapled resection, 20-30% bilateral | NETT (1218 pts) | Best: upper lobe + low exercise capacity |
| Lung Transplantation | Replace diseased lung | - | For advanced disease, FEV1 <25%, BODE >5 |
Sources:
- Fishman's Pulmonary Diseases and Disorders, 5e - Ch. 34 (Bronchoscopic Treatments, pp. 659-660) and Ch. on Advanced COPD Management
- Murray & Nadel's Textbook of Respiratory Medicine, 7e - Ch. 28 (Bronchoscopic LVR, pp. 665-667) and Ch. 47 (Surgical Treatment of Emphysema, pp. 2018-2026)
This is a shared conversation. Sign in to Orris to start your own chat.