Provide notes for my general pathology exam on my topic EYE. Take Reference from Robins and cotran latest edition.i want to get 90 percentage mark.provide easy shortcuts and nmonics diagram flow chart for better understanding.Provide notes for my general pathology exam on my topic EYE. Take Reference from Robins and cotran latest edition.i want to get 90 percentage mark.provide easy shortcuts and nmonics diagram flow chart for better understanding.
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Here are your complete, exam-ready notes on EYE PATHOLOGY from Robbins & Kumar Basic Pathology (latest edition). Organized anatomically, packed with mnemonics, flowcharts, and high-yield shortcuts.
👁️ EYE PATHOLOGY — GENERAL PATHOLOGY EXAM NOTES
Reference: Robbins & Kumar Basic Pathology (10th Ed., ISBN 9780323790185)
🗺️ ANATOMY OVERVIEW (Fig. 21.36)
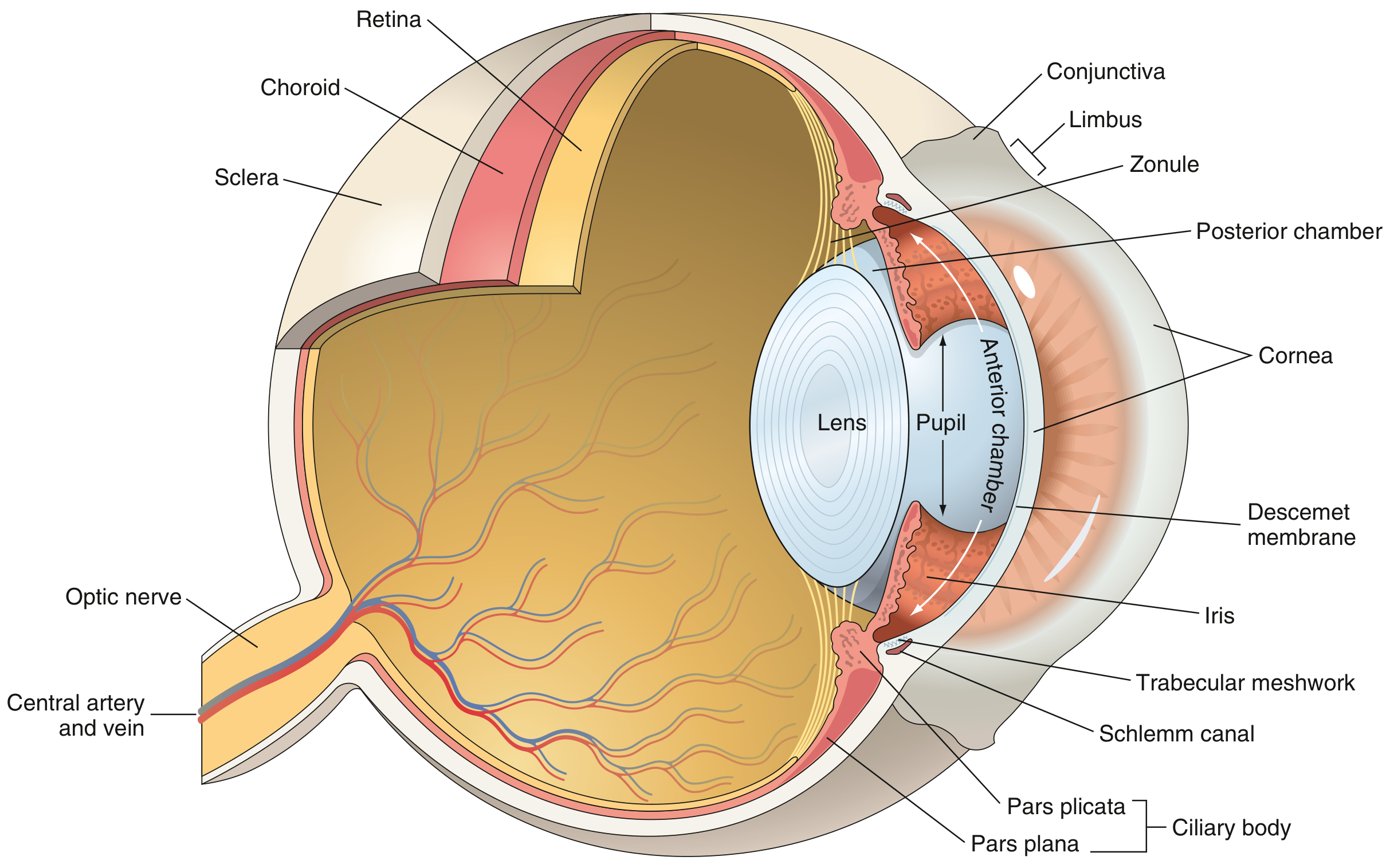
Mnemonic: "Can Classy Surgeons Look Rarely For Unusual Retinal Things?" Cornea → Conjunctiva → Sclera → Lens → Retina → Fovea/Macula → Uvea → RPE → Trabecular meshwork
Key anatomical points:
- Aqueous humor flows: Posterior chamber → through pupil → Anterior chamber → Trabecular meshwork → Canal of Schlemm
- Corneal stroma: avascular + no lymphatics = transparent + transplant-friendly
- RPE (Retinal Pigment Epithelium): supports photoreceptors; sits on Bruch membrane above choriocapillaris
- Adnexa: eyelids, orbit, conjunctiva, lacrimal glands, optic nerve
📋 CHAPTER OVERVIEW MAP
EYE PATHOLOGY
│
├── CONJUNCTIVA
│ ├── Conjunctivitis (Chlamydia = trachoma → #1 infectious blindness)
│ └── Lesions: Pterygium, Pinguecula, SCC, Melanoma
│
├── CORNEA
│ ├── Keratitis & Ulceration
│ ├── Keratoconus
│ └── Fuchs Endothelial Dystrophy
│
├── ANTERIOR SEGMENT
│ ├── Cataract
│ └── Glaucoma (Open-angle vs Closed-angle)
│
├── UVEA
│ ├── Uveitis
│ └── Uveal Melanoma
│
├── RETINA
│ ├── Retinal Detachment
│ ├── Retinal Vascular Disease
│ │ ├── Diabetic Retinopathy
│ │ └── Hypertensive Retinopathy
│ ├── AMD (Dry & Wet)
│ └── Retinitis Pigmentosa
│
└── TUMORS
├── Retinoblastoma
└── Uveal Melanoma
1️⃣ CONJUNCTIVA
Conjunctivitis
| Type | Cause | Key Feature |
|---|---|---|
| Bacterial/Viral | Staph, adenovirus | Heals without sequelae |
| Trachoma | Chlamydia trachomatis (gram-negative intracellular) | #1 infectious cause of blindness worldwide |
Trachoma Progression:
Initial follicular conjunctivitis
↓
Repeated episodes → SCARRING
↓
Eyelid inversion → TRICHIASIS (lashes turn inward)
↓
Repeated corneal rubbing → ULCERATION → SCARRING → OPACIFICATION → BLINDNESS
Mnemonic: "Trachoma Makes Terrible Corneas Slowly" → Trachomatis → Mucous → Trichiasis → Corneal ulcer → Scarring/blindness
Other Conjunctival Lesions
| Lesion | Cause | Nature |
|---|---|---|
| Pterygium | UV/actinic damage | Benign submucosal growth |
| Pinguecula | UV/actinic damage | Benign submucosal (no threat to vision) |
| SCC | UV radiation; preceded by intraepithelial dysplasia | Malignant |
| Conjunctival Nevus | Melanocytic | Benign, rarely invades cornea |
| Conjunctival Melanoma | Acquired BRAF mutations | Unilateral; spreads to parotid/submandibular nodes |
Shortcut: Pterygium vs Pinguecula - Both = benign, both = sun damage; Pterygium = "grows toward pupil (P→P)"; Pinguecula = doesn't invade cornea
2️⃣ CORNEA
Structure (Anterior → Posterior)
Epithelium → Basement Membrane → Bowman Layer (acellular) → Stroma (avascular!) → Descemet Membrane → Endothelium (from neural crest)
A. Keratitis and Ulceration
Causes:
- Bacterial, Fungal, Viral (HSV, HZV - most important), Protozoal (Acanthamoeba - contact lens users)
Mechanism of Stromal Damage:
- Pathogens + epithelial cells → activate collagenases in corneal epithelium & keratocytes → stromal dissolution
Key Signs:
- Hypopyon = exudate + cells accumulating in anterior chamber (visible by slit lamp, or penlight if severe)
Mnemonic "HABit to CHECK Corneas" = HSV/HZV → Acanthamoeba → Bacteria → Collagenase activation → Hypopyon → Exacerbated by Contact lenses (Acanthamoeba) → Keratocyte damage
B. Keratoconus
- Progressive non-inflammatory thinning of cornea → conical shape
- Result: Irregular astigmatism and myopia
- Treatment: Corneal transplant in severe cases
C. Fuchs Endothelial Dystrophy
- Loss of corneal endothelial cells (normally responsible for pumping water OUT of stroma)
- Result: Corneal edema → blurred vision (worse in morning)
- Treatment: Corneal transplant
Shortcut: Fuchs = Failure to pump fluid out = Fluid-logged cornea
3️⃣ ANTERIOR SEGMENT
A. CATARACT 🔑 HIGH YIELD
Definition: Opacification of the lens
Causes (Mnemonic: "CATARACTS"):
C - Congenital (TORCH infections, galactosemia) A - Aging (#1 cause) T - Trauma A - Advanced diabetes (sorbitol accumulation by aldose reductase) R - Radiation (UV, X-ray) A - A lack of nutrition (hypocalcemia, hypoparathyroidism) C - Corticosteroids (posterior subcapsular type) T - Toxins (chlorpromazine) S - Systemic disease (myotonic dystrophy → "Christmas tree" cataract)
Types by location:
LENS
┌────────────┐
│ Anterior │ ← Subcapsular cataract (steroids → posterior subcapsular)
│ Cortical │ ← Spokes of wheel (diabetes)
│ Nuclear │ ← Aging (yellow-brown nuclear sclerosis)
└────────────┘
Pathogenesis of Diabetic Cataract:
Hyperglycemia → Glucose enters lens →
Aldose reductase converts Glucose → Sorbitol →
Sorbitol cannot leave lens → Osmotic swelling →
Lens fiber damage → OPACIFICATION
B. GLAUCOMA 🔑 HIGH YIELD
Definition: Group of conditions with elevated intraocular pressure (IOP) → optic nerve damage → visual field loss
Normal IOP: 10-21 mmHg
Classification Flowchart:
GLAUCOMA
│
┌────────────┴────────────┐
Open-Angle Closed-Angle
(wide angle) (narrow angle)
│ │
Gradual onset ACUTE painful onset
Painless Corneal edema
Tunnel vision Halos around lights
(peripheral first) Red eye, nausea/vomiting
│ │
#1 most common Emergency! - needs
type (90%) immediate Rx
Primary Open-Angle Glaucoma (POAG)
- Pathogenesis: Increased resistance in trabecular meshwork → decreased aqueous outflow → ↑ IOP
- Risk factors: Age, Black race, Family history, Myopia
- Classic finding: Optic disc "cupping" (cup:disc ratio >0.6)
- Treatment: Eye drops (beta-blockers, prostaglandins), laser, surgery
Primary Angle-Closure Glaucoma
- Pathogenesis: Pupillary block → iris bows forward → trabecular meshwork obstructed
- Precipitants: Dark rooms, drugs causing mydriasis (antihistamines, anticholinergics)
- Exam pearl: Shallow anterior chamber
Secondary Glaucoma causes:
- Diabetic retinopathy (neovascularization on iris → neovascular glaucoma)
- Lens-induced (hypermature cataract)
- Post-uveitis (synechiae)
- Steroid use
Mnemonic: "GLAUCOMA" Genetics (family hx) | Loss of peripheral vision first | Aqueous outflow blocked | Unilateral or bilateral | Cupping of optic disc | Old age | Mesenchymal trabecular defect | Acute vs chronic
4️⃣ UVEA (Iris + Ciliary Body + Choroid)
Uveitis
Classification:
| Type | Location | Common Causes |
|---|---|---|
| Anterior (Iritis/Iridocyclitis) | Iris + ciliary body | HLA-B27 diseases (AS, ReA, Psoriasis), Sarcoidosis |
| Intermediate | Vitreous/pars plana | MS, sarcoidosis |
| Posterior (Choroiditis/Retinitis) | Choroid/retina | CMV (immunocomp), Toxoplasma, TB |
| Panuveitis | All layers | Sarcoidosis, VKH, Behçet disease |
Mnemonic for Posterior Uveitis causes: "CT Scan" = CMV + Toxoplasma + Syphilis + Candida + HIV/AIDS + NTB
Uveal Melanoma 🔑
- Most common primary intraocular tumor in adults
- Arises from melanocytes of uveal tract (choroid most common)
- Molecular: Mutations in GNAQ/GNA11 (90%), monosomy 3 = worst prognosis
- Spreads: Hematogenously → LIVER (characteristic)
- Types: Spindle cell (better prognosis) vs Epithelioid cell (worse prognosis)
- Iris melanomas = most benign; Choroidal melanomas = most common
Shortcut: Uveal melanoma = Adults + Goes to Liver + GNAQ mutation
5️⃣ RETINA 🔑 MOST HIGH-YIELD SECTION
A. Retinal Detachment
Types:
RETINAL DETACHMENT
│
┌────┴────┐
Rhegmatogenous Non-Rhegmatogenous
(has a HOLE) (no hole)
│ │
Hole/tear in ┌──────┴──────┐
sensory retina Tractional Exudative
│ (DM, sickle (HTN, tumors,
Vitreous fluid cell) inflammation)
enters gap
High-Yield Mechanism:
- Neurosensory retina separates from RPE
- Photoreceptors lose nutrient supply from choriocapillaris → degenerate rapidly
- Symptoms: Flashes (photopsia) → Floaters → "Curtain" visual field defect
B. Diabetic Retinopathy 🔑🔑 MUST KNOW
DIABETES
│
▼
Basement membrane thickening + pericyte loss
│
▼
┌─────────────────────────────────────────────────────┐
│ NONPROLIFERATIVE DIABETIC RETINOPATHY (NPDR) │
│ │
│ Microaneurysms (1st change) → Dot hemorrhages → │
│ Hard exudates (lipid leakage) → Cotton-wool spots │
│ (nerve fiber infarcts) → Venous beading │
└────────────────────┬────────────────────────────────┘
│ VEGF ↑ (hypoxia)
▼
┌─────────────────────────────────────────────────────┐
│ PROLIFERATIVE DIABETIC RETINOPATHY (PDR) │
│ │
│ Retinal neovascularization (NVD/NVE) → │
│ Vitreous hemorrhage → Traction retinal detachment │
│ → Neovascular glaucoma → BLINDNESS │
└─────────────────────────────────────────────────────┘
Key Facts:
- 60-80% develop some form of retinopathy within 15-20 years
- Microaneurysms = FIRST visible change
- Pericyte loss = early hallmark (pericytes normally suppress neovascularization)
- VEGF drives neovascularization (hypoxia → VEGF ↑)
- Treatment: Anti-VEGF injections (intravitreal) = current mainstay + laser photocoagulation
Mnemonic for NPDR findings: "Micro-Dot-Hard-Cotton-Vein" Microaneurysms → Dot hemorrhages → Hard exudates → Cotton-wool spots → Venous beading
C. Hypertensive Retinopathy
| Grade | Finding |
|---|---|
| Grade 1 | Arterial narrowing (A:V ratio <2:3) |
| Grade 2 | AV nicking/nipping (sclerotic artery compresses vein at crossing) |
| Grade 3 | Flame hemorrhages, cotton-wool spots, hard exudates |
| Grade 4 | Papilledema (severe/malignant HTN) |
Classic signs:
- "Copper wire" arterioles = moderate sclerosis
- "Silver wire" arterioles = severe sclerosis
- Salus sign = AV nipping
- Gunn sign = AV nipping with right-angle deviation of vein
Mnemonic for grades: "Never Argue, Forget Grades Properly" N-ormal → A-rterial narrowing → F-lame hemorrhage + exudates → G-rade 4 papilledema
D. Age-Related Macular Degeneration (AMD)
AMD
│
┌──────────┴──────────┐
DRY (Atrophic) WET (Neovascular)
~85% ~15%
│ │
DRUSEN in Bruch membrane Choroidal NV through
Geographic RPE atrophy Bruch membrane
No treatment ↓
Antioxidants + zinc Fluid/blood leakage
slow progression under retina
↓
Anti-VEGF injections
(CURRENT MAINSTAY Rx)
Pathogenesis: RPE + Bruch membrane + choriocapillaris = functional unit → disruption → photoreceptor loss
Risk factors: Age (>75 yrs, 8% cumulative incidence), Smoking, Genetics (CFH mutation), Caucasian
Shortcut: "Dry = Drusen + Degenerating (no vessels); Wet = With new Vessels"
E. Retinitis Pigmentosa (RP)
- Hereditary (AR, AD, X-linked) degeneration of rod photoreceptors
- Progressive night blindness → tunnel vision → central vision loss
- Classic finding: "Bone spicule" pigment deposits in peripheral retina
- No curative treatment
Mnemonic: "Rod Pathology = Night blindness first" (rods = dark/dim vision)
6️⃣ TUMORS OF THE EYE 🔑
RETINOBLASTOMA 🔑🔑 CLASSIC EXAM TOPIC
Definition: Most common primary intraocular tumor in children (typically <5 years)
Genetics Flowchart:
RB1 gene (chromosome 13q14) = TUMOR SUPPRESSOR
│
┌────────┴────────┐
SPORADIC (60%) HEREDITARY (40%)
│ │
Unilateral BILATERAL (or multifocal)
Both mutations First mutation = germline
acquired Second = somatic
(somatic)
│
Knudson's "Two-Hit Hypothesis"
Hit 1 → Hit 2 → RB protein lost
→ E2F transcription factor uncontrolled
→ Cell cycle S-phase entry → TUMOR
Key Features:
| Feature | Detail |
|---|---|
| Presentation | Leukocoria (white pupillary reflex = "cat's eye") + Strabismus |
| Histology | Small blue round cells (SBRT); Flexner-Wintersteiner rosettes (pathognomonic) |
| Calcification | Common (useful on imaging) |
| Spread | Along optic nerve → brain; Hematogenous → bone |
| Trilateral RB | Bilateral RB + pineoblastoma |
Hereditary RB associations:
- 30-fold ↑ risk of osteosarcoma and other sarcomas
- Lifetime surveillance needed
Mnemonic: "LEUKO-RB" Leukocoria (white reflex) | Early (<5 yrs) | Unilateral = sporadic | Knudson 2-hit | Osteosarcoma risk (hereditary) | Rosettes (Flexner-Wintersteiner) | Bilateral = hereditary
UVEAL MELANOMA (Adults)
(see Uvea section above)
7️⃣ QUICK COMPARISON TABLES
Causes of Blindness - Global vs USA
| Setting | #1 Cause |
|---|---|
| Worldwide - Infectious | Trachoma (C. trachomatis) |
| Worldwide - Overall | Cataract |
| Developed countries | AMD, Glaucoma, Diabetic retinopathy |
Anti-VEGF Therapy in the Eye (KEY CONCEPT)
Conditions treated with intravitreal anti-VEGF:
- Wet AMD
- Proliferative diabetic retinopathy / Diabetic macular edema
- Corneal neovascularization
- Neovascular glaucoma
"When hypoxia drives VEGF up, anti-VEGF brings vision back"
8️⃣ MASTER MNEMONIC SHEET
| Topic | Mnemonic |
|---|---|
| Cataract causes | CATARACTS (see above) |
| Trachoma progression | Trachomatis → Mucous → Trichiasis → Corneal scar |
| NPDR features | Micro-Dot-Hard-Cotton-Vein |
| Retinoblastoma | LEUKO-RB |
| Glaucoma features | GLAUCOMA (see above) |
| Posterior uveitis | CT Scan (CMV, Toxo, Syphilis, Candida, AIDS, NTB) |
| AMD dry vs wet | Dry=Drusen; Wet=With Vessels |
| Fuchs dystrophy | Fuchs=Fails to pump Fluid |
9️⃣ ONE-LINERS FOR EXAM
- Trachoma = C. trachomatis = #1 infectious blindness worldwide
- Retinoblastoma = Leukocoria + Flexner-Wintersteiner rosettes + chromosome 13q14
- Uveal melanoma = Most common intraocular tumor in adults → mets to liver
- Cataract = #1 cause of treatable blindness worldwide
- Microaneurysm = FIRST retinal change in diabetes
- Pericyte loss = hallmark of early diabetic retinopathy
- Anti-VEGF = treatment for Wet AMD + proliferative diabetic retinopathy
- Open angle glaucoma = silent, painless, peripheral vision loss first
- Angle-closure glaucoma = ACUTE emergency, painful, halos, red eye
- Fuchs dystrophy = endothelial loss → corneal edema (worse in morning)
- Keratoconus = non-inflammatory corneal thinning → cone shape → irregular astigmatism
- Retinal detachment = neurosensory retina separates from RPE; rhegmatogenous = has hole
- Dry AMD = drusen + geographic atrophy; Wet AMD = choroidal neovascularization
- GNAQ/GNA11 mutation = uveal melanoma; monosomy 3 = worst prognosis
- Herpes simplex = most important viral cause of keratitis
- Cornea = avascular + no lymphatics = transparent + best graft success
- Silver wire arterioles = severe hypertensive sclerosis
- Cotton-wool spots = nerve fiber layer infarcts (in DM, HTN)
- Knudson's two-hit = retinoblastoma model; germline (hereditary) vs somatic (sporadic)
- Bone spicule pigment = retinitis pigmentosa (rod degeneration)
🔟 EXAM STRATEGY TIPS
- Anatomy questions always show eye cross-section - memorize structures Cornea → Iris → Lens → Vitreous → Retina → Choroid → Sclera
- Pediatric intraocular tumor = think Retinoblastoma (always!)
- Adult intraocular tumor = think Uveal Melanoma (always!)
- Leukocoria = white pupil = Retinoblastoma until proven otherwise
- VEGF comes up in 4 different retinal conditions - memorize the link
- Trachoma = infectious blindness worldwide (love to ask this in MCQs)
- When you see pericyte loss = early diabetes retinopathy
- Flexner-Wintersteiner rosettes = retinoblastoma (pathognomonic)
- Optic disc cupping = glaucoma
- Drusen in Bruch membrane = AMD
Reference: Robbins & Kumar Basic Pathology, 10th Edition (Chapter 21 - The Eye, pp. 866-880)
This is a shared conversation. Sign in to Orris to start your own chat.