Stone in salivary gland
Reading File
Finding Sources
Finding Sources
Searching PubMed
sialolithiasis salivary gland calculus
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive, authoritative information. Here is a complete clinical overview.
Sialolithiasis (Salivary Gland Stone)
Definition
Sialolithiasis is the formation of calculi (sialoliths) within the ductal system of the salivary glands. It is the most common cause of salivary gland inflammation.
- Cummings Otolaryngology Head and Neck Surgery
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery
Gland Distribution
| Gland | Frequency |
|---|---|
| Submandibular (Wharton duct) | 80-90% |
| Parotid (Stensen duct) | 10-20% |
| Sublingual | ~1% |
| Minor salivary glands | Rare (upper lip most common) |
Why the submandibular gland is most affected:
- The Wharton duct is longer, wider, more tortuous, and runs against gravity around the mylohyoid
- Submandibular saliva is more viscous, more alkaline, and has higher calcium and phosphate content
- Alkaline saliva precipitates calcium phosphate, promoting stone formation
Composition of Stones
Sialoliths are composed predominantly of calcium phosphate and carbonate deposited in concentric shells (~10 µm thick), within an organic matrix of glycoproteins and mucopolysaccharides. Small amounts of magnesium, potassium, and ammonium are also present.
Pathophysiology
The exact etiology is unknown, but key drivers include:
- Salivary stasis - intermittent stasis alters mucoid elements of saliva, forming an organic gel that acts as a framework for salt deposition
- Ductal inflammation and injury - chronic sialadenitis is the inciting event in parotid stones; in the submandibular gland, the stone itself may come first, then cause stasis and retrograde bacterial sialadenitis
- Sialomicrooliths - microscopic concretions (~1% of submandibular glands at necropsy) that seed larger stone growth
Note: Serum calcium and phosphorus levels are NOT typically related to stone formation. However, hyperparathyroidism increases the risk of sialolithiasis (and co-existing nephrocalcinosis).
Associations: Diabetes mellitus, hypertension, chronic liver disease, nephrolithiasis. The antiretroviral atazanavir has also been linked.
Clinical Features
- Postprandial salivary colic - recurrent episodes of pain and swelling of the affected gland triggered by eating (meal-time syndrome)
- Swelling is diffuse, rapid in onset, non-tender, and resolves over a few hours
- History of recurrent acute suppurative sialadenitis
- On examination: bimanual palpation may reveal a palpable stone in the submandibular duct floor of mouth
- Foul-tasting fluid on gland massage (mucoid/mucopurulent)
- Parotid stones may be seen at the orifice of the Stensen duct
- Stones of minor salivary glands present as painless hard swellings
Imaging
Figure 54.6a (Bailey & Love's) - X-ray, CT, and ultrasound showing submandibular sialolithiasis:
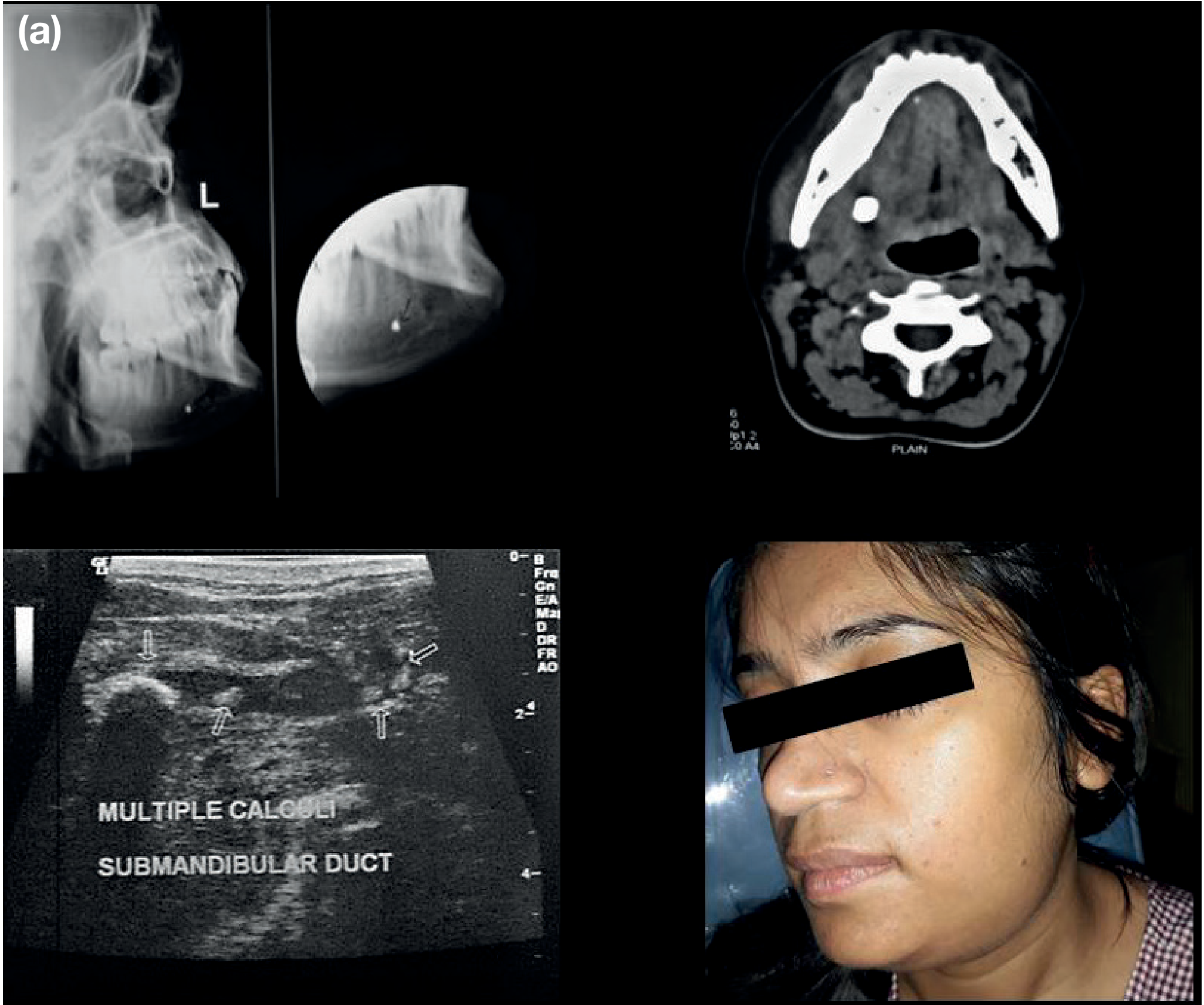
| Modality | Notes |
|---|---|
| Plain X-ray (occlusal/lateral skull view) | Traditional first step; only ~80% radiopaque; misses radiolucent stones |
| Ultrasound (US) | First-line; cost-effective, no radiation, can detect both radiopaque and radiolucent stones, dynamic assessment; useful intraoperatively |
| CT scan (fine cuts) | Excellent for stone detection; useful if neoplasm suspected; reveals dilated duct and enlarged gland |
| MRI | Calculus appears as low signal on both T1 and T2; MR sialography uses saliva as contrast and rivals digital sialography in accuracy |
| Sialography (digital subtraction) | Gold standard; sensitivity 95-100%; detects radiolucent stones; contraindicated in active infection and for stones in the oral portion of the Wharton duct |
| Sialoendoscopy | Direct visualization; first-line where available; both diagnostic and therapeutic |
Management
General principle: The earlier the stone is removed, the better - stones that stay in ducts grow larger and become more immobile.
Conservative (initial)
- Sialagogues (lemon drops, sour candies)
- Hydration
- Local heat
- Gland massage
- Antibiotics if infection is present
Minimally Invasive (preferred)
Figure 54.6b (Bailey & Love's) - Sialoendoscopy showing a stone in the duct (yellow calculus visible) and retrieved stones of varying sizes:
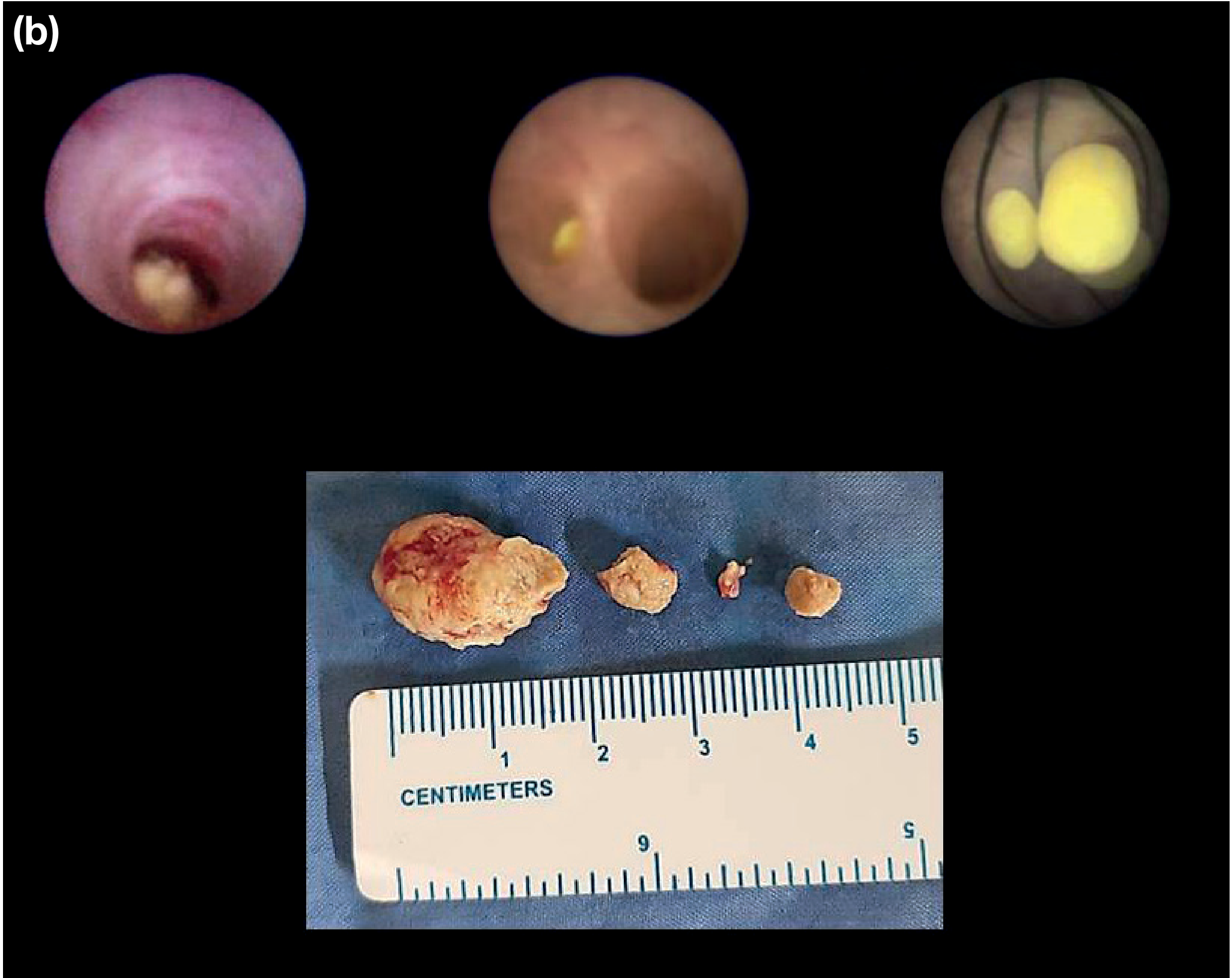
| Stone Size/Location | Approach |
|---|---|
| Small (<5 mm) distal | Sialoendoscopy alone (basket retrieval) |
| Large (>5 mm) distal | Duct slitting + endoscopy |
| Impacted / anterior submandibular duct (within 2 cm of orifice) | Transoral incision / manual milking |
| 5-7 mm intraparenchymal | Endoscopic extraction |
| >7 mm intraparenchymal | Transoral slitting or open approach |
| Not palpable, not visualizable | Extracorporeal shock wave lithotripsy (ESWL), then sialoendoscopy for fragment retrieval |
| ESWL limit | Not suitable for stones >7-10 mm |
| Intracorporeal lithotripsy | Laser (Ho:YAG, erbium:YAG, XeCl excimer) - expensive, risk of duct perforation |
Surgical (last resort)
- Submandibular gland excision - for failed minimally invasive approaches, or hilar/proximal/intraglandular stones not amenable to endoscopy
- Parotid stones <7 mm - endoscopic; difficult cases need combined transcutaneous approach; parotidectomy only as a last resort
- Traditional parotid management (pre-endoscopy era): transoral approach or parotidectomy; high stricture risk with duct manipulation
A 2024 systematic review and meta-analysis (PMID 37486613) confirmed sialendoscopy success rates, with stone removal achieved in up to 93% of patients and symptom relief in up to 95%.
Complications
- Acute suppurative sialadenitis (bacterial superinfection)
- Abscess formation
- Chronic non-specific sialadenitis
- Ductal stricture (post-manipulation)
- Gland fibrosis and permanent dysfunction
Key Points to Remember
- Submandibular > Parotid for stone frequency (85% vs 10%)
- Submandibular stones tend to be proximal (ductal); parotid stones tend to be distal (hilar/parenchymal)
- ~20-30% of parotid stones are radiolucent - plain X-ray will miss them
- Sialendoscopy has transformed management - gland preservation is now achievable in most cases
- ESWL is not available in the US (important exam point)
- Stone on MRI: low signal on T1 and T2
- Sialography is contraindicated in active infection
Sources: Cummings Otolaryngology Head and Neck Surgery; Bailey and Love's Short Practice of Surgery 28th Ed.; Scott-Brown's Otorhinolaryngology Head & Neck Surgery
This is a shared conversation. Sign in to Orris to start your own chat.