Subclavian artery and it's applied Anatomy
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
I now have comprehensive information from multiple authoritative sources. Let me compile the full answer.
Subclavian Artery - Anatomy and Applied
Origin
- Right subclavian artery: Arises from the brachiocephalic trunk (which bifurcates behind the right sternoclavicular joint)
- Left subclavian artery: Arises directly from the arch of the aorta (the last branch of the arch), slightly more to the left
Both arteries exit the thorax through the superior thoracic aperture and arch over the apex of the lung and dome of the pleura to the base of the neck.
Parts - Relation to Anterior Scalene Muscle
The subclavian artery is divided into three parts in relation to the anterior scalene muscle:
| Part | Extent |
|---|---|
| 1st part | From origin to medial border of anterior scalene |
| 2nd part | Posterior to anterior scalene muscle |
| 3rd part | From lateral border of anterior scalene to lateral border of rib I |
At the lateral border of rib I, it becomes the axillary artery.
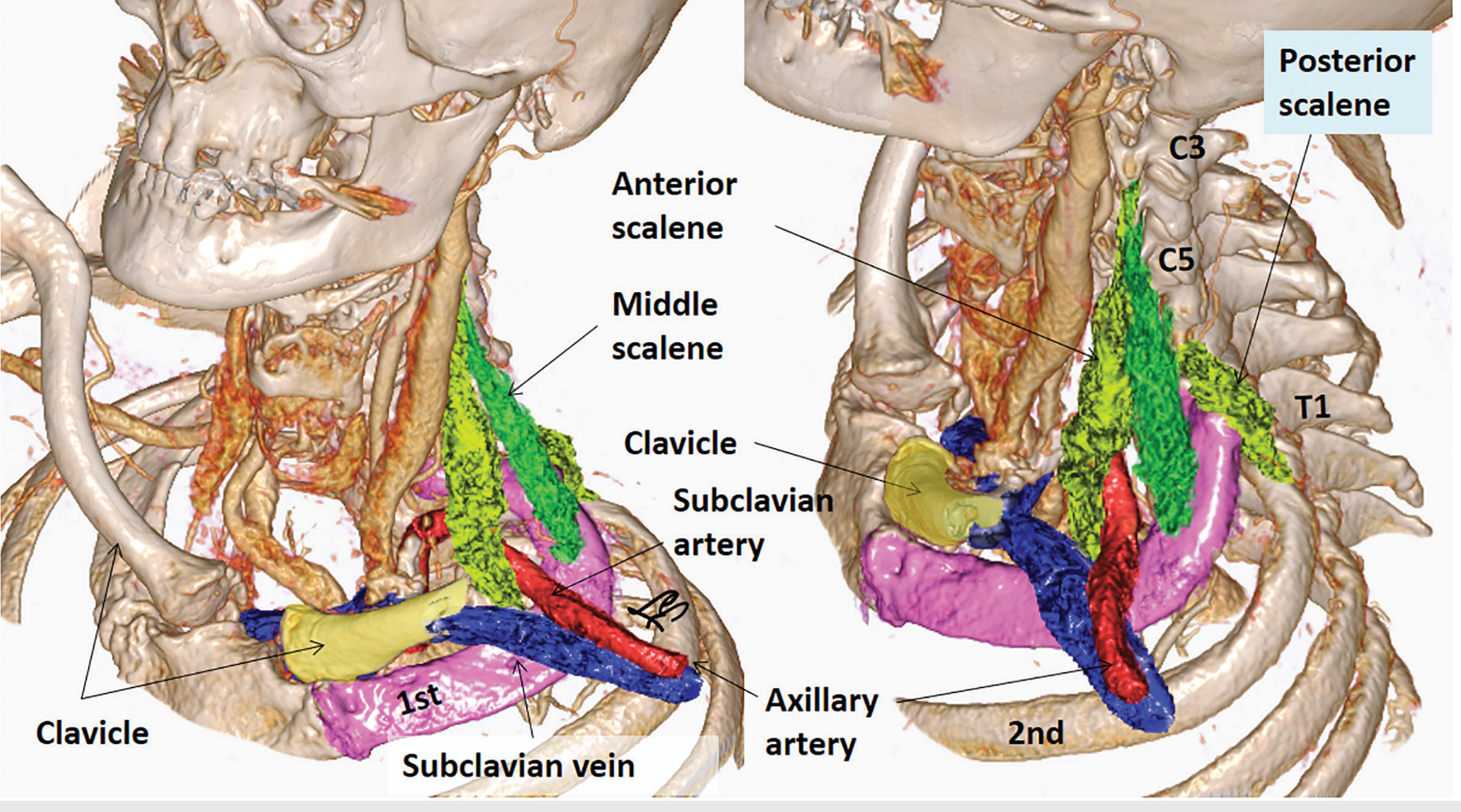
3D CT rendering of scalene muscle relationships with subclavian vessels - Imaging Anatomy Vol. 3
Branches
All branches arise from the 1st part, except the costocervical trunk on the right side, which arises from the 2nd part.
1. Vertebral Artery (1st branch of 1st part)
- Ascends and enters the foramen transversarium at C6, passing superiorly through C6-C1
- Turns medially at C1, crosses the posterior arch of the atlas
- Enters the cranial cavity via the foramen magnum to supply the posterior brain
- Right + left vertebral arteries unite to form the basilar artery
- Vulnerable to damage in fractures involving transverse processes of upper 6 cervical vertebrae
2. Thyrocervical Trunk (2nd branch of 1st part)
A short, wide trunk giving off three main branches:
- Inferior thyroid artery: Ascends anterior to the scalene, turns medially behind the carotid sheath, supplies the thyroid (posterior surface), pharynx, esophagus, trachea, and larynx; gives off the ascending cervical artery (supplies spinal cord and prevertebral muscles)
- Transverse cervical artery: Passes laterally across the posterior triangle, divides into superficial branch (deep to trapezius) and deep branch (deep to rhomboids along medial scapular border)
- Suprascapular artery: Passes laterally, crosses over the superior transverse scapular ligament into the supraspinous fossa; anastomoses with the circumflex scapular artery
3. Internal Thoracic Artery (3rd branch, from inferior surface of 1st part)
- Descends posterior to the clavicle and large veins
- Runs anterior to the pleural cavity, posterior to ribs and anterior to transversus thoracis
- Gives off anterior intercostal branches; also gives the pericardiacophrenic artery (to pericardium and diaphragm) and musculophrenic artery
- Terminates as the superior epigastric artery, which enters the rectus sheath and anastomoses with the inferior epigastric artery (from external iliac) - clinically important anastomotic channel in aortic coarctation
4. Costocervical Trunk (1st part on left; 2nd part on right)
- Ascends and arches posteriorly over the dome of the pleura
- Divides into:
- Deep cervical artery: Ascends in the back of the neck; anastomoses with the descending branch of the occipital artery
- Supreme (highest) intercostal artery: Descends anterior to rib I; gives rise to posterior intercostal arteries for the 1st and 2nd intercostal spaces
5. Dorsal Scapular Artery
- Arises from the 2nd or 3rd part (more commonly the 3rd), or occasionally from the transverse cervical artery
- Passes posterolaterally to the superior angle of the scapula, descends along the medial border of the scapula posterior to the rhomboid muscles
Diagram of Relations
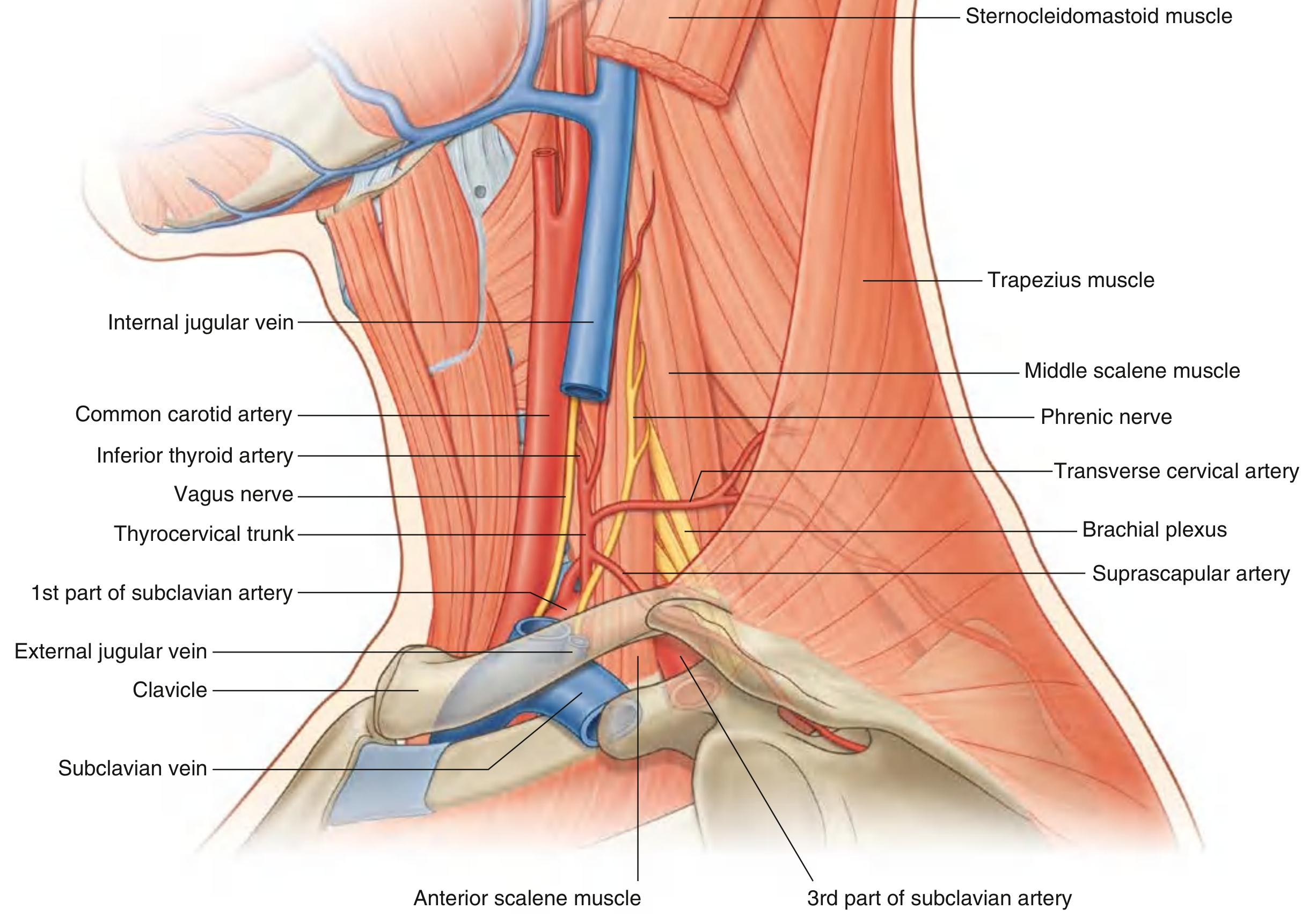
Fig. 8.189 - Arteries in the Posterior Triangle of the Neck (Gray's Anatomy for Students)
Applied Anatomy
1. Subclavian Steal Syndrome
A clinically important applied anatomy scenario:
- Caused by significant stenosis/occlusion of the subclavian artery proximal to the vertebral artery (most commonly the left side)
- At rest, collateral channels (through anastomoses of ascending cervical, deep cervical, thyroid arteries) maintain perfusion to the upper limb
- During vigorous arm exercise, demand increases - collaterals dilate, causing retrograde flow in the ipsilateral vertebral artery, siphoning blood from the basilar system
- This produces brainstem/cerebellar ischemia: dizziness, vertigo, visual disturbances (binocular loss), and arm claudication
- Classic finding: significant pressure difference between both arms (e.g., 45 mmHg difference as in the case described)
- Collateral routes include:
- Via muscular branches of vertebral artery → ascending cervical → inferior thyroid → thyrocervical trunk
- Via deep cervical artery → costocervical trunk (enters subclavian distal to stenosis)
- Via thyroid gland anastomoses (bilateral superior and inferior thyroid arteries)
- Via occipital artery → deep cervical artery
- Treatment: extrathoracic carotid-subclavian bypass, or endovascular stenting
2. Cervical Rib and Thoracic Outlet Syndrome (TOS)
- The thoracic outlet contains: first rib, subclavian artery and vein, brachial plexus, clavicle, and lung apex
- A cervical rib or anomalous scalene insertion can narrow the scalene triangle, compressing the subclavian artery - this is Scalenus syndrome
- Arterial TOS (least common, ~1%): Subclavian artery compression causes poststenotic dilatation → secondary thrombus → distal embolisation to hand. Presents with reduced BP in affected limb, pallor, coolness, claudication, paresthesias. No neurological signs. Diagnosed by Doppler ultrasound. Treated with thrombolysis/embolectomy + surgical excision of cervical rib
- Neurogenic TOS (most common): Compression of lower brachial plexus (C8/T1), often by anomalous fibrocartilaginous band from elongated C7 transverse process to rib I. Wasting of intrinsic hand muscles, sensory loss on 5th finger
- Venous TOS: Subclavian vein thrombosis → arm swelling
- Compression can occur in: scalene triangle, costoclavicular space (clavicle + rib I), or subpectoral space (pectoralis minor + coracoid)
3. Fracture of Rib I
- The subclavian artery is fixed to the superior surface of rib I by surrounding muscles as it passes from neck to axilla
- Rapid deceleration (upper thoracic trauma) can cause a rib I fracture, compromising the distal subclavian or proximal axillary artery
- Fortunately, rich anastomotic networks around the scapula (between subclavian and axillary branches) mean complete ischemia is rare even with vessel transection
4. Subclavian/Axillary Venous Access
- Clinical practice calls the infraclavicular venous route the "subclavian route," but most clinicians actually enter the first part of the axillary vein
- The vein should be punctured at the midclavicular line or lateral to it - medial puncture risks catheter kinking under the subclavius muscle, causing catheter fatigue and fracture (important for pacemaker wires and Hickman lines)
- The vein passes anterior to the artery, superior to rib I, and inferior to the clavicle
5. Anomalous Right Subclavian Artery (Arteria Lusoria)
- Occurs when the right 4th pharyngeal arch artery and right dorsal aorta disappear cranial to the 7th intersegmental artery
- Results in the right subclavian artery arising from the distal aortic arch, passing posterior to the esophagus (retroesophageal course) to supply the right upper limb
- Forms a vascular ring around the trachea and esophagus
- Usually clinically silent (ring is not tight enough to constrict), but may rarely cause dysphagia (dysphagia lusoria)
6. Ligation of the Subclavian Artery
- If ligation is needed (e.g., trauma, vascular surgery), survival of the limb depends on the periarticular anastomosis around the scapula:
- Suprascapular artery (from thyrocervical trunk) anastomoses with the circumflex scapular artery (from subscapular, a branch of axillary artery)
- Transverse cervical artery (deep branch) anastomoses with the subscapular/lateral thoracic arteries
- Ligation proximal to the thyrocervical trunk is safer for limb viability than distal ligation
Sources: Gray's Anatomy for Students, p. 1166-1172 | Color Atlas of Human Anatomy Vol. 2, p. 103-104 | Imaging Anatomy Vol. 3 | Harrison's Principles of Internal Medicine 22E, p. TOS section | The Developing Human (Moore), p. 868
What is torticollis
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed for a comprehensive answer. Here it is:
Torticollis (Wryneck)
Definition
Torticollis (Latin: tortus = twisted, collum = neck), also called wryneck, is a deformity in which the head is bent/tilted towards one side while the chin points to the opposite side - due to unilateral shortening or spasm of the sternocleidomastoid (SCM) muscle.
In torticollis, the head is tilted towards and rotated away from the tight sternocleidomastoid muscle.
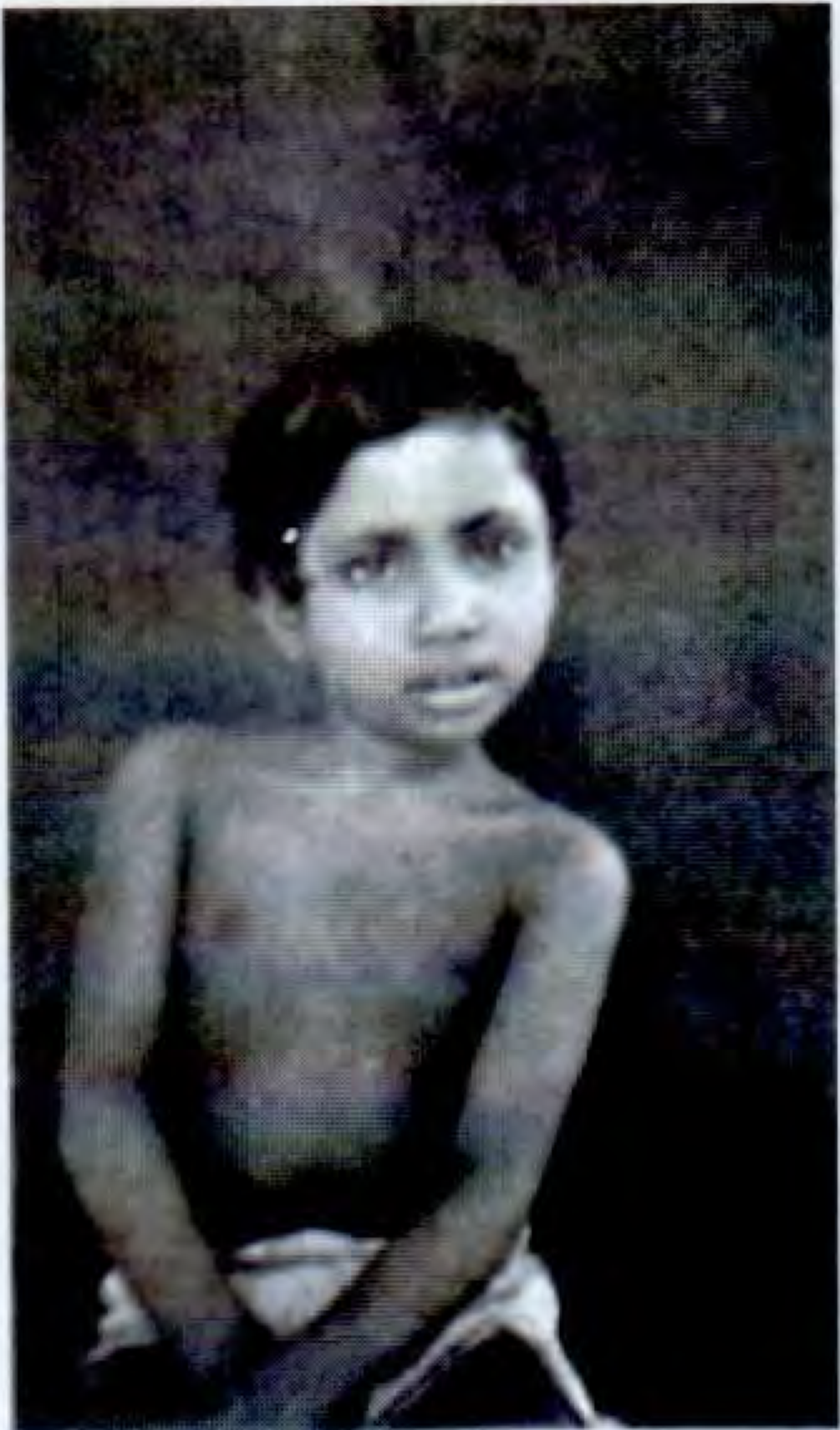
Clinical appearance of torticollis - S Das Manual on Clinical Surgery
Muscles Involved
The sternocleidomastoid (SCM) is the primary muscle. Remember its actions:
- Ipsilateral side: tilts the head toward the same shoulder
- Contralateral side: rotates the chin to the opposite side
So a tight/contracted right SCM → head tilts to the right, chin points to the left.
In spasmodic torticollis, the levator scapulae and trapezius are also prominently involved; the levator spasm also slightly lifts the ipsilateral shoulder.
Classification / Types
1. Congenital Muscular Torticollis (CMT)
The most common form in infants and children.
Pathogenesis / Proposed causes:
- Malposition of fetus in utero / intrauterine constraint
- Birth trauma - tearing of SCM fibers during difficult delivery → bleeding → hematoma → necrosis of muscle fibers → fibrosis and shortening of the SCM
- Intrauterine or perinatal compartment syndrome
- Vascular injury to the SCM
- Primary SCM myopathy (explains cases after C-section deliveries)
Clinical features:
- Presents in early infancy - head tilted to the affected side, chin rotated away
- A palpable firm sternomastoid "tumour" (fibrotic nodule) may be felt within the muscle - this typically confirms the diagnosis without further imaging
- In long-standing untreated cases: facial asymmetry (plagiocephaly) develops - the distance from the outer canthus of the eye to the angle of the mouth is smaller on the affected side, the eyebrow is less arched, the nose is somewhat flattened, and the cheek is less full - likely due to impaired vascular supply from restricted mobility
Associations:
- Developmental dysplasia of the hip (DDH) - an association exists, so hip examination is mandatory in all CMT cases
- Other causes to consider: ocular torticollis, vertebral anomalies, Sandifer syndrome, Grisel syndrome, posterior fossa tumours, benign paroxysmal torticollis
Diagnosis:
- Clinical: characteristic fibrotic nodule is usually sufficient
- Ultrasonography: useful to evaluate the SCM and predict need for surgery (SCM thickness >5 cm correlates with poor response to stretching)
- Cervical spine radiographs / MRI: if diagnosis uncertain, neurological signs present, or to rule out congenital vertebral anomalies
Treatment:
- Non-operative (first line in infancy): Stretching exercises - rotate the chin to the affected side (stretching the shortened muscle). Initiated before 3-4 months of age → 92-100% achieve full passive neck rotation, with only ~1% requiring surgery. For every month treatment is delayed, the chance of surgery increases.
- Operative: If CMT persists beyond 1 year of life, or if non-operative treatment fails. Involves release of the origin and/or insertion of the SCM (tenotomy). Best results occur before 3 years; surgery for neglected cases in older children/adults gives significant improvement in quality of life but less complete correction.
- Botulinum toxin + physiotherapy: used for resistant cases
2. Spasmodic Torticollis (Idiopathic Cervical Dystonia)
The most frequent form of focal dystonia, affecting adults.
Features:
- Onset in early to middle adult life; more common in women (peak in 5th decade)
- Begins as subtle tilting/turning of head - worsens gradually
- Can be intermittent (smooth/jerky) or sustained deviation/tilt to one side
- Often accompanied by irregular tremor beating in the direction of the dystonic movement
- Muscles: SCM, levator scapulae, trapezius, and posterior cervical muscles (bilateral on EMG)
- The deviated shoulder is slightly elevated due to levator spasm
- "Sensory tricks" (gestes): Characteristic - placing a hand on the chin or neck, light counterpressure on the side of deviation, or resting the occiput on a high-backed chair reduces spasms. These tricks become less effective as disease progresses.
- Spasms worsen on standing/walking, reduce when lying down
- In chronic cases: affected muscles undergo hypertrophy and become painful
- ~15% also have oral/mandibular/hand dystonia; ~10% have blepharospasm
Aetiology: Idiopathic in most. DYT1 gene abnormality found in a few patients.
Treatment:
- Botulinum toxin injections (every 3-6 months into affected muscles): Treatment of choice - ~90% get some relief. Guided by palpation + EMG. Adverse effects: excessive weakness, local pain, dysphagia. 5-10% develop neutralising antibodies and become resistant.
- Anticholinergics (trihexyphenidyl/benztropine): may give partial relief but poorly tolerated
- L-dopa and antiparkinsonian agents: generally ineffective
- Deep brain stimulation (DBS): for cases refractory to medications and botulinum toxin - targets globus pallidus (GPi) or subthalamic nucleus
- Surgical: Combined sectioning of the spinal accessory nerve + first three cervical motor roots bilaterally - used in severe cases; gives relief in 1/3-1/2 of cases for up to 6 years
3. Acquired (Secondary) Torticollis
| Type | Cause |
|---|---|
| Traumatic | Fracture-dislocation of cervical spine |
| Rheumatic | Sudden onset after exposure to cold/draught |
| Inflammatory | Inflamed cervical lymph nodes; soft tissue infection of the neck |
| Atlantoaxial rotatory subluxation | Spontaneous or post-pharyngeal infection (Grisel syndrome) |
| Spinal pathology | Pott's disease of cervical spine |
| Ocular (compensatory) | Visual defect or squint causing head tilt to compensate |
| Posterior fossa tumour | Head tilt due to raised ICP or cerebellar herniation - a red flag |
| Contracture | Burns, scarring, ulceration of neck skin |
| Scoliosis | Compensatory posture |
Key Anatomical Point (SCM Actions - Why the Deformity Occurs)
The SCM has two heads (sternal and clavicular), inserting into the mastoid process and superior nuchal line. Its unilateral action:
- Tilts the head toward the same side
- Rotates the chin to the opposite side
So a contracted/spastic right SCM produces: right lateral tilt + left chin rotation = right torticollis.
Sources: S Das Manual on Clinical Surgery, p. 377-378 | Bailey & Love's Short Practice of Surgery 28th ed. | Campbell's Operative Orthopaedics 15th ed. 2026 | Adams & Victor's Principles of Neurology 12th ed., p. 110-111 | The Developing Human (Moore), p. 965
This is a shared conversation. Sign in to Orris to start your own chat.