Arboviral Infections
Reading File
Finding Sources
Finding Sources
Searching PubMed
arboviral infections epidemiology treatment
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive data. Let me compile the full, detailed response on arboviral infections.
Arboviral Infections
Arboviruses (arthropod-borne viruses) are a large, ecologically defined group of RNA viruses transmitted to vertebrate hosts - including humans - through the bite of infected arthropods (mosquitoes, ticks, sandflies, midges). There are several hundred known arboviruses, of which about 100 are recognized human pathogens. Most human infections are zoonotic "dead-end" events, with important exceptions: urban dengue, chikungunya, Zika, and urban yellow fever maintain human-to-mosquito-to-human transmission cycles.
Classification
Arboviruses are not a formal taxonomic group but a functional one. They span multiple virus families:
| Family | Genus | Key Members |
|---|---|---|
| Flaviviridae | Flavivirus | Dengue (4 serotypes), Yellow fever, Zika, West Nile, Japanese B encephalitis, St. Louis encephalitis, Tick-borne encephalitis, Powassan |
| Togaviridae | Alphavirus | Chikungunya, Eastern equine encephalitis (EEE), Western equine encephalitis (WEE), Venezuelan equine encephalitis (VEE) |
| Bunyaviridae | Orthobunyavirus, Phlebovirus | La Crosse, California encephalitis, Rift Valley fever, Crimean-Congo hemorrhagic fever, Hantavirus |
| Reoviridae | Coltivirus | Colorado tick fever |
| Rhabdoviridae | Vesiculovirus | Vesicular stomatitis |
| Arenaviridae | Arenavirus | Lassa (rodent-borne), Junin, Machupo |
- Jawetz, Melnick & Adelberg's Medical Microbiology, 28th ed., Table 38-1
Transmission Cycles
The diagram below illustrates the generalized mosquito-borne flavivirus transmission cycle:
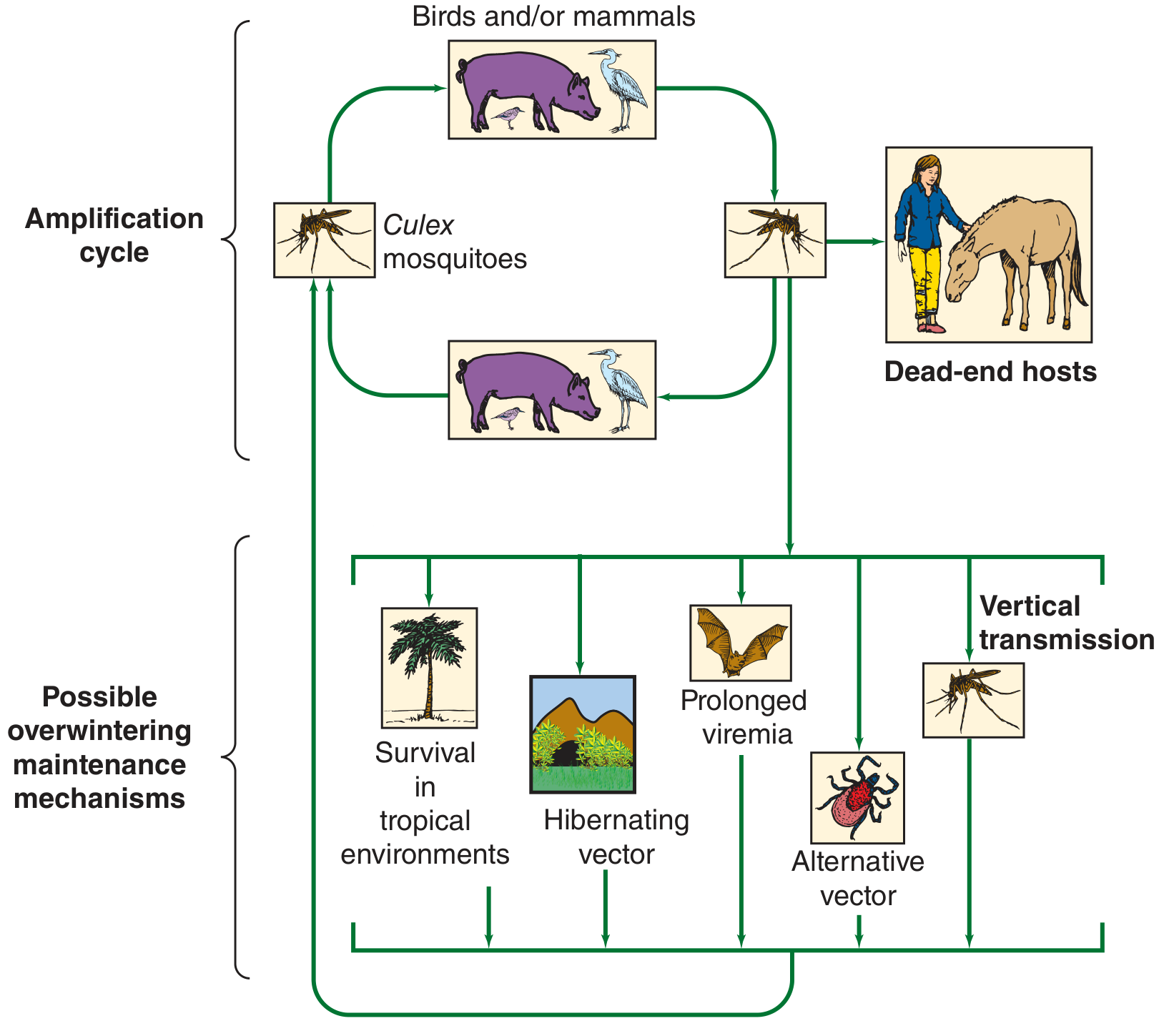
Key principles:
-
Most arboviruses cycle between arthropod vectors and vertebrate reservoir hosts (birds, rodents, primates)
-
Humans and horses are usually dead-end hosts (viremia too low to infect feeding arthropods), with exceptions noted above
-
The female arthropod takes a blood meal from a viremic host, virus multiplies in the midgut, spreads to salivary glands, then is transmitted to the next host at the next blood meal (extrinsic incubation period)
-
Ticks can acquire infection at any life stage and transmit transovarially to offspring
-
Tick-borne encephalitis can also be acquired by drinking unpasteurized milk from infected goats
-
Jawetz, Melnick & Adelberg's Medical Microbiology, 28th ed.
Clinical Syndromes
Arboviral diseases fall into three overlapping clinical categories based on the predominant site of viral replication:
1. Undifferentiated Febrile Illness ± Rash
- Typically benign and self-limited
- Fever, malaise, headache, myalgia, arthralgia
- Maculopapular rash may appear
- Examples: dengue fever (uncomplicated), Zika, chikungunya, Colorado tick fever
2. Encephalitis / Neuroinvasive Disease
- Often high case-fatality rate; significant neurologic sequelae in survivors
- Fever, headache, neck stiffness, confusion, seizures, coma
- Examples: EEE (33% mortality), WEE (5% mortality), St. Louis encephalitis, West Nile encephalitis, Japanese B encephalitis, La Crosse encephalitis
3. Hemorrhagic Fever
-
Severe, frequently fatal
-
Hemorrhage, shock, multi-organ failure
-
Examples: Dengue hemorrhagic fever / Dengue shock syndrome, Yellow fever, Crimean-Congo hemorrhagic fever, Rift Valley fever
-
Jawetz, Melnick & Adelberg's Medical Microbiology, 28th ed.
Major Arboviruses - Disease-Specific Details
Dengue
Virus: Flavivirus with 4 serotypes (DEN-1, DEN-2, DEN-3, DEN-4)
Vector: Aedes aegypti (day-biting); also Aedes albopictus
Epidemiology: ~400 million infections/year globally; 100 million symptomatic; 22,000 deaths; >100 endemic countries. Most common febrile illness in travelers returning from the tropics (excluding sub-Saharan Africa)
Pathogenesis - Antibody-Dependent Enhancement (ADE):
Dengue hemorrhagic fever (DHF) and Dengue shock syndrome (DSS) occur predominantly with the second dengue infection (with a different serotype). Cross-reactive non-neutralizing antibodies from the first infection facilitate viral entry into monocytes/macrophages via Fc receptors, amplifying viral replication. This ADE mechanism explains why severe dengue is uncommon at primary infection but dangerous at reinfection.
Clinical stages:
- Febrile phase (days 1-3): High fever ("breakbone fever"), severe headache, retro-orbital pain, myalgia, arthralgia
- Critical phase (days 4-6): Fever defervescence; plasma leakage, pleural effusions, ascites; risk of DHF/DSS
- Recovery phase (days 7-10): Fluid reabsorption; risk of fluid overload; bradycardia may appear
DHF criteria (WHO): Fever, hemorrhagic manifestations, thrombocytopenia (<100,000/mm³), evidence of plasma leakage
DSS: DHF + shock (narrow pulse pressure <20 mmHg or hypotension)
Diagnosis: NS1 antigen (acute phase, days 1-5); IgM/IgG serology; RT-PCR
Treatment: Supportive; IV fluid resuscitation titrated carefully; avoid aspirin and NSAIDs (increase bleeding risk). No specific antiviral.
Vaccines: Dengvaxia (CYD-TDV) approved in some countries; contraindicated in seronegative individuals (paradoxically increases severe disease risk in primary infection); TAK-003 (Qdenga) approved in EU/UK for ages 4+
- Sherris & Ryan's Medical Microbiology, 8th ed.; Harrison's Principles of Internal Medicine, 22nd ed.; Goldman-Cecil Medicine
Yellow Fever
Virus: Flavivirus
Vectors: Aedes aegypti (urban cycle); Haemagogus spp. (jungle cycle)
Epidemiology: Endemic in 34 African countries and 13 Central/South American countries; 84,000-170,000 severe cases and 29,000-60,000 deaths annually (Africa modeling data, 2013)
Clinical features:
- Incubation: 3-6 days
- Most infections asymptomatic or mild
- Classic severe disease (15% of cases):
- Phase 1 (Infection): Abrupt fever, chills, headache, back pain, nausea, vomiting
- Remission: Hours to 1 day of improvement
- Phase 2 (Intoxication): High fever, jaundice (hepatic involvement), Faget's sign (relative bradycardia with fever), hemorrhage (black vomit = "vomito negro"), shock, multi-organ failure
- Fatality of severe disease: 30-60%
- No long-term sequelae in survivors
Diagnosis: IgM serology; early blood PCR for viral RNA
Treatment: Supportive; avoid aspirin/NSAIDs
Prevention: Live attenuated 17-D vaccine - highly effective (single dose provides lifelong immunity); required for travel to endemic areas by many countries
- Sherris & Ryan's Medical Microbiology, 8th ed.
West Nile Virus (WNV)
Virus: Flavivirus
Vector: Culex spp. mosquitoes
Reservoir: Wild birds (crows, ravens as sentinels); horses are dead-end hosts
Distribution: North America, South America, Europe, Africa, Middle East, Asia, Australia
Clinical spectrum:
- ~80% asymptomatic
- ~20%: West Nile fever - fever, myalgia, rash, nausea, vomiting, diarrhea
- ~1%: West Nile neuroinvasive disease - meningitis, encephalitis, or acute flaccid paralysis (anterior horn cell involvement mimicking polio)
- Risk of neuroinvasive disease increases dramatically with age and immunosuppression
Neuroinvasive disease: Encephalitis (most common), meningitis, or acute flaccid myelitis. Long-term functional and neuropsychological deficits are common in survivors (Roberts et al., Ann Neurol 2025, PMID 40008684 - systematic review).
Diagnosis: CSF pleocytosis (lymphocytic); WNV IgM in CSF (diagnostic); serum IgM/IgG; PCR may be negative by symptom onset
Treatment: No specific antiviral; supportive care; IV immunoglobulin and interferon studied but not established
Table: Key North American Arbovirus Neuroinvasive Diseases
| Virus | Vector | Key Host | Clinical Features | Mortality |
|---|---|---|---|---|
| West Nile (Flavivirus) | Culex spp. | Birds | Fever, rash, encephalitis, flaccid paralysis | Varies; ~10% in neuroinvasive |
| EEE (Alphavirus) | Culiseta melanura | Birds | Severe encephalitis, all ages | ~33% |
| WEE (Alphavirus) | Culex tarsalis | Birds | Encephalitis, severe in infants | ~5%; 60% neurologic sequelae in infants |
| St. Louis Encephalitis (Flavivirus) | Culex tarsalis | Birds | Encephalitis, adults >40 most affected | ~5-30% |
| California/La Crosse (Bunyavirus) | Aedes spp. | Small mammals | Fever, seizures, encephalitis in children | <1% |
| Powassan (Flavivirus) | Ixodes ticks | Small mammals/deer | Encephalitis, meningitis | ~10%; 50% with sequelae |
- Goldman-Cecil Medicine; Sherris & Ryan's Medical Microbiology, 8th ed.
Chikungunya
Virus: Alphavirus (Togaviridae)
Vector: Aedes aegypti and Aedes albopictus
Epidemiology: Originally African, now widespread in Asia, Indian Ocean, Americas, Pacific Islands
Clinical features:
- Incubation: 1-12 days (typically 2-4 days)
- Abrupt high fever and severe, debilitating polyarthralgia/arthritis (the name "chikungunya" means "that which bends up" in Makonde)
- Maculopapular rash
- Usually self-limiting fever (3-7 days)
- Hallmark: Symmetric, bilateral joint pain/swelling - wrists, ankles, phalanges - can persist for months to years (chronic chikungunya arthritis)
- Can cause Guillain-Barré syndrome (post-infectious)
Diagnosis: RT-PCR (early); IgM/IgG serology
Treatment: Supportive; NSAIDs/chloroquine for chronic arthritis; no specific antiviral or licensed vaccine (as of 2025; IXCHIQ approved in the US in 2023)
Zika Virus
Virus: Flavivirus
Vector: Aedes aegypti, Aedes albopictus; also sexual transmission; transplacental transmission (unique among arboviruses in causing birth defects)
Clinical features:
- Most infections (80%) asymptomatic
- Mild fever, rash, conjunctivitis, arthralgia - very similar to dengue/chikungunya
- Key complications:
- Congenital Zika syndrome: Microcephaly, cortical thinning, calcifications, ophthalmologic abnormalities - caused by direct fetal neurotropism
- Guillain-Barré syndrome: Post-infectious; occurs 1-3 weeks after acute illness
Diagnosis: RT-PCR (acute, <7 days); IgM serology (cross-reacts with dengue/yellow fever - plaque reduction neutralization test [PRNT] needed for confirmation)
Treatment: Supportive only; no vaccine approved; pregnant women in endemic areas require close surveillance
- Goldman-Cecil Medicine; Jawetz, Melnick & Adelberg's Medical Microbiology, 28th ed.
A 2026 systematic review on DENV/CHIKV/ZIKV co-infections (PMID 41619199) highlights that co-infection is increasingly recognized and may worsen outcomes - clinicians in endemic areas should maintain co-infection in the differential.
Japanese B Encephalitis (JEV)
Virus: Flavivirus
Vector: Culex tritaeniorhynchus
Reservoir: Pigs (amplifying host), wild birds
Distribution: South and Southeast Asia, Western Pacific; most important cause of viral encephalitis in Asia
Clinical features:
- Most infections subclinical
- Encephalitis: fever, headache, altered consciousness, seizures, extrapyramidal signs (Parkinson-like features due to basal ganglia involvement)
- Mortality: 20-30%; 50% of survivors have neurologic sequelae
Vaccine: Live attenuated SA 14-14-2 strain; inactivated vaccines also available; recommended for travelers to endemic areas
Colorado Tick Fever
Virus: Coltivirus (Reoviridae) - double-stranded RNA
Vector: Dermacentor andersoni tick
Distribution: Mountain west of North America (Rocky Mountains)
Clinical features:
- Biphasic (saddle-back) fever - fever for 2-3 days, remission 1-2 days, then recurrence
- Chills, headache, myalgia, retro-orbital pain, abdominal pain
- Rash in ~5-10%
- Meningitis in small percentage
- Virus infects erythrocyte precursors; can be detected in red blood cells for weeks (important for blood transfusion safety)
Diagnosis - General Approach
| Timing | Test |
|---|---|
| Days 1-5 (viremic) | RT-PCR, NS1 antigen (dengue), viral culture |
| Days 5+ | IgM/IgG serology (ELISA, PRNT) |
| Neuroinvasive disease | CSF: IgM (WNV), PCR, pleocytosis |
Cross-reactivity between flaviviruses (dengue, Zika, yellow fever, WNV, JEV) is a significant diagnostic challenge in serology; PRNT is the gold standard for differentiation.
Treatment - General Principles
- No specific antiviral therapy is approved for most arboviruses
- Supportive care is the mainstay: fluid management, antipyretics (avoid aspirin/NSAIDs in dengue and yellow fever), ICU support for severe disease
- Dengue: careful titrated IV fluid resuscitation; oral rehydration in mild-moderate DSS
- Neuroinvasive disease: supportive; role of IVIG, steroids, and interferons remains investigational for most
Prevention and Vector Control
- Personal protection: Insect repellents (DEET, picaridin), long-sleeved clothing, bed nets, day and night protection (Aedes bites by day)
- Vector control: Elimination of breeding sites (standing water), insecticides, biological controls, sterile insect technique (Wolbachia-infected Aedes)
- Vaccines available:
- Yellow fever: Live attenuated 17-D vaccine (single dose = lifelong protection; required for travel)
- Japanese B encephalitis: IXIARO (inactivated), SA 14-14-2 (live attenuated)
- Dengue: Dengvaxia (seropositive individuals only), TAK-003/Qdenga
- Chikungunya: IXCHIQ (live attenuated, FDA-approved 2023)
- Tick-borne encephalitis: FSME-Immun/Encepur (Europe/Canada)
- Blood transfusion safety: Screening donors for WNV and Zika in endemic/epidemic settings; Colorado tick fever virus persists in RBCs
Geographic Distribution Summary
| Region | Dominant Arboviruses |
|---|---|
| Americas (tropical) | Dengue, Yellow fever, Zika, Chikungunya, EEE, WEE, VEE |
| North America | West Nile, EEE, WEE, St. Louis encephalitis, La Crosse, Colorado tick fever, Powassan |
| South/Southeast Asia | Dengue, Japanese B encephalitis, Chikungunya, Zika |
| Africa | Yellow fever, Dengue, Chikungunya, Rift Valley fever, Crimean-Congo HF |
| Europe/Central Asia | Tick-borne encephalitis, West Nile, Crimean-Congo HF |
| Australia/Pacific | Murray Valley encephalitis, Dengue, Ross River fever |
Key Clinical Pearls:
- Severe dengue (DHF/DSS) typically occurs at re-infection with a different serotype via antibody-dependent enhancement - not at primary infection
- Zika is the only arbovirus with established sexual transmission and teratogenicity - critical for pregnant women and their partners
- Yellow fever has a characteristic Faget's sign (relative bradycardia despite fever) and biphasic illness with "intoxication" phase
- Chikungunya causes chronic arthritis lasting months/years - distinguishes it from other febrile arboviral illnesses
- West Nile can cause acute flaccid myelitis (anterior horn cell disease), mimicking polio - rare but important
- "Breakbone fever" (dengue) is named for the extreme bone/joint pain; actual bone lesions do not occur
This is a shared conversation. Sign in to Orris to start your own chat.