Leprosy
Reading File
Finding Sources
Searching PubMed
leprosy Hansen disease
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I have comprehensive data from multiple authoritative textbooks. Now I'll compose the full answer.
Leprosy (Hansen's Disease)
Definition and Causative Agent
Leprosy is a chronic, slowly progressive infectious disease caused primarily by Mycobacterium leprae and, less frequently, by the more recently described M. lepromatosis (proposed 2008). It mainly affects the skin, peripheral nerves, and mucosa of the upper respiratory tract. Despite its low communicability, leprosy remains endemic, with approximately 200,000 new infections reported annually, concentrated in South/Southeast Asia, East Africa, and Brazil, which together account for >65% of the global burden. - Robbins, Cotran & Kumar Pathologic Basis of Disease
Microbiology
-
Obligate intracellular pathogen - cannot be cultured in vitro
-
Acid-fast bacillus (weakly acid-fast on standard Ziehl-Neelsen; best visualized with Fite stain)
-
Replicates optimally at 32-34°C (human skin temperature) - this explains why it avoids warm core organs
-
Doubling time: approximately 12-14 days (extremely slow)
-
Virulence factor: phenolic glycolipid-1 (PGL-1) - mediates invasion of host cells and binding to peripheral nerve basal lamina
-
Inhibits mitochondrial energy metabolism to evade host immune response
-
Primary target: Schwann cells of the peripheral nervous system
-
Clusters characteristically in "globi" (clumps/bundles) inside macrophages (lepra cells)
-
Sherris & Ryan's Medical Microbiology, 8th Ed.; Park's Textbook of Preventive & Social Medicine
Epidemiology
| Factor | Details |
|---|---|
| Transmission | Nasal/respiratory droplets from active (multibacillary) cases; minor traumatic skin inoculation; zoonotic from 9-banded armadillos (southern USA, South America); red squirrels in British Isles |
| Incubation period | Usually 3-5 years; range 1-20 years (occasionally up to 4 decades) |
| Infectivity | Highly infectious but very low pathogenicity - most exposed individuals never develop disease |
| Portal of exit | Nasal mucosa (millions of bacilli shed per sneeze), ulcerated skin |
| Attack rate | 4.4-12% among household contacts of lepromatous cases within 5 years |
| Endemic countries | India (#1), Brazil, Indonesia, Angola, Madagascar, DRC |
| Global trend | Prevalence fell from 5.2 million (1985) to ~177,175 (2018) - a >90% reduction |
- Park's Textbook of Preventive & Social Medicine; Red Book 2021
Pathogenesis and Immunology
The spectrum of disease is entirely determined by the host's cell-mediated immune (CMI) response:
| Tuberculoid (TT) | Lepromatous (LL) | |
|---|---|---|
| CMI | Strong Th1 (IL-2, IFN-γ) | Weak Th1; relative Th2/T-reg dominance |
| CD4+ T cells | Abundant | Scarce |
| Macrophage activation | Classical M1 | Foamy, bacteria-laden |
| Bacterial load | Low (paucibacillary) | High (multibacillary) |
| Antibodies to M. leprae | Low | High (but NOT protective) |
| Immune complexes | Rare | Common - cause erythema nodosum, vasculitis, glomerulonephritis |
After entering Schwann cells, M. leprae causes demyelination of peripheral sensory nerves, leading to localized anesthesia. If untreated, progressive nerve damage causes irreversible disability.
BCG vaccination cross-protects (28-60%) due to shared antigens with M. tuberculosis.
- Robbins, Cotran & Kumar; Sherris & Ryan's Medical Microbiology
Classification
Ridley-Jopling Scale (used in the US - histopathologic):
- Tuberculoid (TT)
- Borderline Tuberculoid (BT)
- Mid-Borderline (BB)
- Borderline Lepromatous (BL)
- Lepromatous (LL)
WHO Simplified Classification (field use - clinical skin count):
-
Paucibacillary (PB): 1-5 skin lesions (usually TT/BT)
-
Multibacillary (MB): >5 skin lesions (usually BB/BL/LL)
-
Red Book 2021
Cardinal Clinical Features
A diagnosis of leprosy requires one or more of:
- Hypopigmented or erythematous skin patch(es) with loss of sensation (light touch affected first)
- Thickened peripheral nerves
- Acid-fast bacilli in slit-skin smears or biopsy
- Park's Textbook of Preventive & Social Medicine
Clinical Forms
Tuberculoid Leprosy
- Dry, scaly, flat-to-raised lesions - irregular shapes, hyperpigmented elevated margins, depressed pale centers (central healing)
- Asymmetric large peripheral nerve involvement
- Nerves enclosed in granulomatous reactions; small peripheral twigs destroyed
- Complications: skin anesthesia, muscle atrophy, contractures, paralysis, autoamputation, corneal ulceration (facial nerve palsy)
- Histology: well-formed granulomas resembling tuberculosis, with almost no bacilli (paucibacillary)
Lepromatous Leprosy
- Symmetric skin thickening, nodules, plaques on face/ears/wrists/elbows/knees
- Progressive nodule coalescence → leonine facies
- Madarosis (loss of eyebrows/eyelashes)
- Widespread invasion of Schwann cells and perineural macrophages
- Nasal mucosa involvement: rhinitis, septal perforation, nasal depression ("saddle nose")
- Testes destruction → sterility
- Histology: lipid-laden foamy macrophages (lepra cells) packed with "globi" of acid-fast bacilli; CD8+ T cells dominant; sparse CD4+
- In advanced disease: bacilli present in sputum and blood
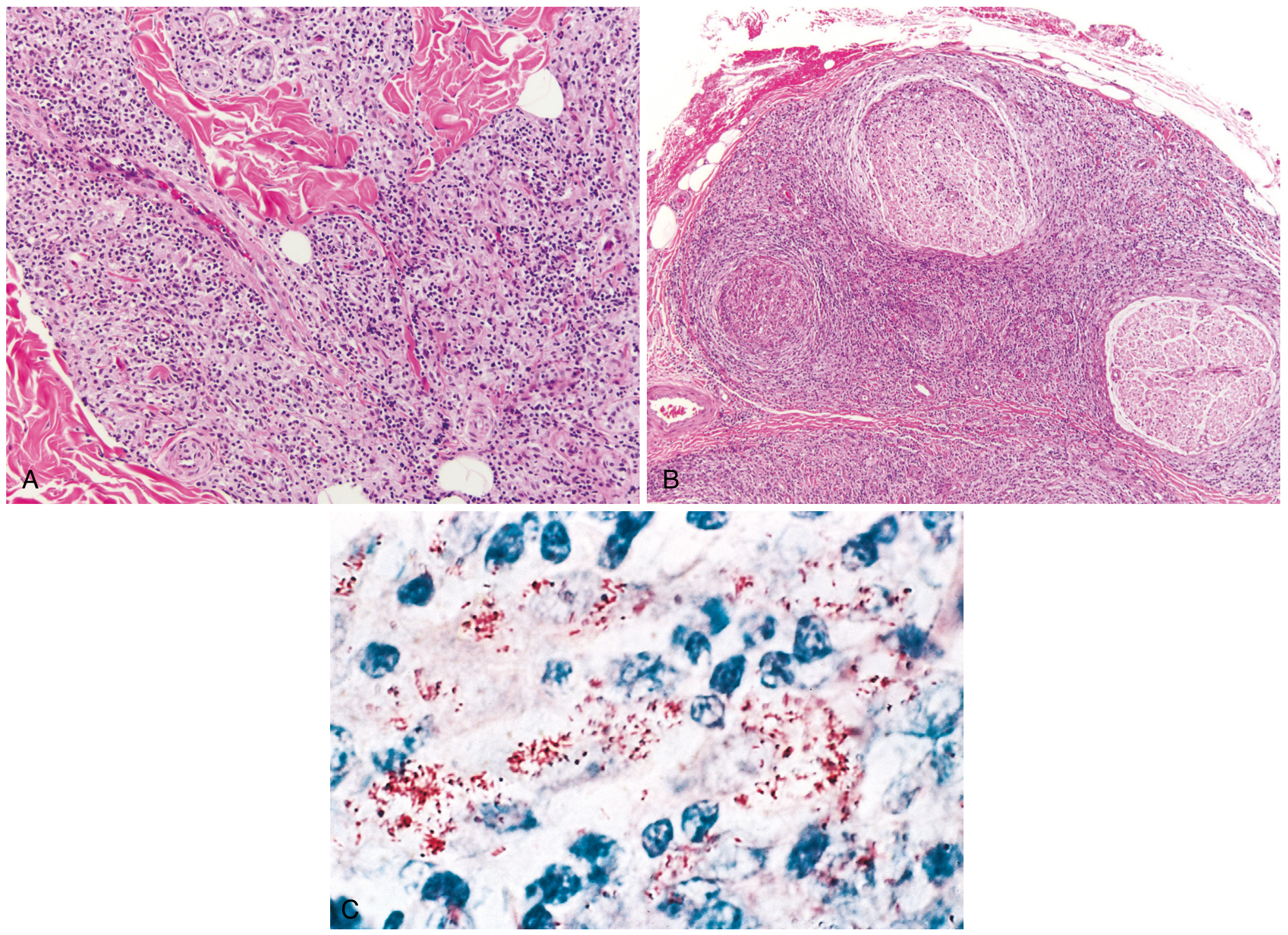
Fig. 8.33 - Robbins: (A) Tuberculoid leprosy - macrophage infiltration surrounding adnexa, vessels, and nerves. (B) Lepromatous leprosy - dense lymphocytic/macrophage infiltration of large nerve bundles. (C) Acid-fast bacilli within macrophages (lepromatous form).
Lepra Reactions (Immunologic Exacerbations)
These can occur during treatment or spontaneously and are the leading cause of nerve damage and disability:
Type 1 - Reversal Reaction (LR-1)
- Occurs in borderline forms (BT, BB, BL)
- Mechanism: sudden increase in effective CMI
- Features: acute tenderness/swelling of skin lesions and nerves, new lesion development, ulceration possible
- No fever or systemic toxicity typically
- Treatment: Prednisone (1 mg/kg/day; with methotrexate as a sparing agent for long-term use)
Type 2 - Erythema Nodosum Leprosum (ENL / LR-2)
-
Occurs in borderline lepromatous and lepromatous forms
-
Mechanism: systemic immune complex deposition
-
Features: tender red subcutaneous papules/nodules, high fever, migratory polyarthralgia, painful lymphadenopathy, iridocyclitis, rarely nephritis
-
Treatment: Thalidomide (100-400 mg/day for 4 days) under strict supervision; also prednisone
-
Red Book 2021
Diagnosis
-
Gold standard: Skin biopsy with histopathologic examination by experienced pathologist (Fite stain for AFB)
-
Slit-skin smears: AFB visible in MB/lepromatous forms, rarely in PB/tuberculoid
-
PCR (for M. leprae and M. lepromatosis) - available at specialized centers
-
Molecular tests for drug resistance and strain typing
-
Lepromin skin test (DTH response) - no longer routinely available
-
Tuberculin/IGRA: NOT used for leprosy diagnosis
-
Pre-treatment workup: G6PD deficiency screen, CBC, LFTs, rule out active TB (especially if HIV+)
-
Red Book 2021
Treatment - Multidrug Therapy (MDT)
Adults: Dapsone + Rifampin + Clofazimine
| Regimen | Drugs | Duration |
|---|---|---|
| Paucibacillary (PB) | Rifampin + Dapsone | 6 months |
| Multibacillary (MB) | Rifampin + Dapsone + Clofazimine | 12 months |
Key points:
-
Infectivity ceases within a few days of starting MDT
-
Relapse is rare: 0.01-0.14%
-
Multi-drug therapy prevents resistance (resistance to all 3 agents is documented but extremely rare)
-
Rifampin renders the patient non-infectious within ~3 weeks
-
MDT is provided free of charge by WHO globally
-
Isolation is NOT required - standard precautions only
-
Red Book 2021
Disability and Complications
- Leading cause of permanent physical disability among communicable diseases worldwide
- Unrecognized trauma due to anesthesia → ulcers, fractures, bone resorption, autoamputation
- Eye involvement: corneal scarring - all patients should have ophthalmologic evaluation
- Deformities: claw hand, foot-drop, claw toes, plantar ulcers, saddle nose, lagophthalmos
Control Measures
- Reportable disease (US: report to state health authorities, CDC, and NHDP)
- Household contacts: initial examination (no prolonged follow-up if asymptomatic)
- Chemoprophylaxis: not recommended
- BCG vaccine: 28-60% protective; used as adjunct in Brazil; may precipitate leprosy in subclinically infected individuals
- No vaccines approved in the US specifically for leprosy
Sources:
- Robbins, Cotran & Kumar - Pathologic Basis of Disease
- Red Book 2021 - Report of the Committee on Infectious Diseases
- Park's Textbook of Preventive and Social Medicine
- Sherris & Ryan's Medical Microbiology, 8th Ed.
Recent evidence note: A 2024 systematic review (PMID 39308868) updates leprosy immunopathogenesis, reinforcing the Th1/Th2 dichotomy and highlighting the role of regulatory T cells in lepromatous disease - consistent with the textbook framework above.
This is a shared conversation. Sign in to Orris to start your own chat.