Tumor like lesions of bone
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
I now have comprehensive material to write a detailed response. Let me compose the full answer:
Tumor-Like Lesions of Bone
These are non-neoplastic lesions that clinically, radiologically, and sometimes histologically mimic true bone tumors. They are broadly divided into cystic lesions, fibrous lesions, and reactive/histiocytic lesions. The major entities are:
1. Simple (Unicameral / Solitary) Bone Cyst
Epidemiology & Presentation
- Most common in children and adolescents (usually <20 years); male predominance
- Majority (>65%) occur in the proximal humerus, followed by proximal femur and distal tibia
- Often asymptomatic - discovered incidentally or after a pathologic fracture from minor trauma (e.g., throwing a baseball)
Pathogenesis
- Believed to result from a developmental defect in the physis leading to local obstruction of interstitial fluid drainage and accumulation of fluid under increased pressure
Active vs. Latent
- Active cyst: abuts the physeal plate - more likely to grow and fracture
- Latent cyst: normal bone intervenes between cyst and physis - more stable
Radiology
- Symmetric, midline, centrally located cystic expansion with cortical thinning
- The bone is expanded but generally no wider than the physis
- Often appears trabeculated
- "Fallen leaf sign" - fractured cortical fragment falls to the dependent portion of the cyst, pathognomonic
Histology
- Thin fibrous lining containing fibrous tissue, giant cells, hemosiderin, and a few chronic inflammatory cells
- No true epithelial lining
Treatment
- Asymptomatic: observation with annual X-rays for 2 years
- Symptomatic: aspiration and injection with methylprednisolone acetate, bone marrow aspirate, or bone graft substitute
- High-risk locations (proximal femur): curettage, grafting, and internal fixation to prevent fracture/osteonecrosis
2. Aneurysmal Bone Cyst (ABC)
Epidemiology & Presentation
- All age groups, but most common in adolescence (10-20 years)
- Common sites: femur, tibia, and vertebral body posterior elements
- Presents with pain and swelling; locally aggressive despite being non-neoplastic
Pathogenesis
- Spindle-shaped cells frequently show rearrangements of chromosome 17p13 - fusion of the USP6 gene (deubiquitinating enzyme) to regulatory elements of COL1A1, leading to USP6 overexpression
- USP6 upregulates NF-κB activity → increases matrix metalloproteases → cystic bone resorption
- About 30% are secondary ABCs arising within pre-existing lesions (GCT, chondroblastoma, fibrous dysplasia, osteosarcoma)
Radiology
- Eccentric, expansile, lytic metaphyseal lesion with well-defined margins
- MRI/CT: internal septa and characteristic fluid-fluid levels (blood of different ages layering)
- Wider than the closest physis (distinguishes it from UBC)
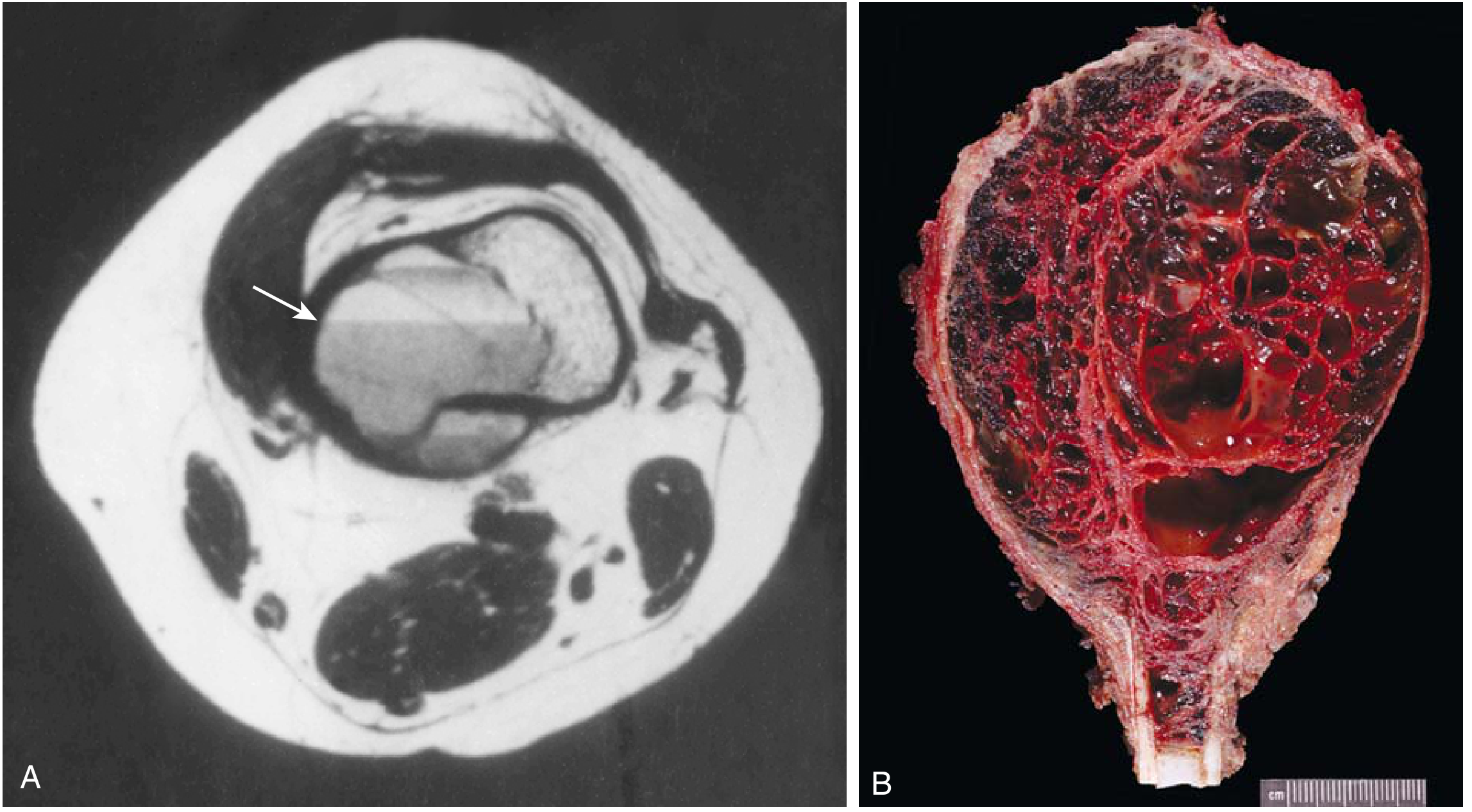
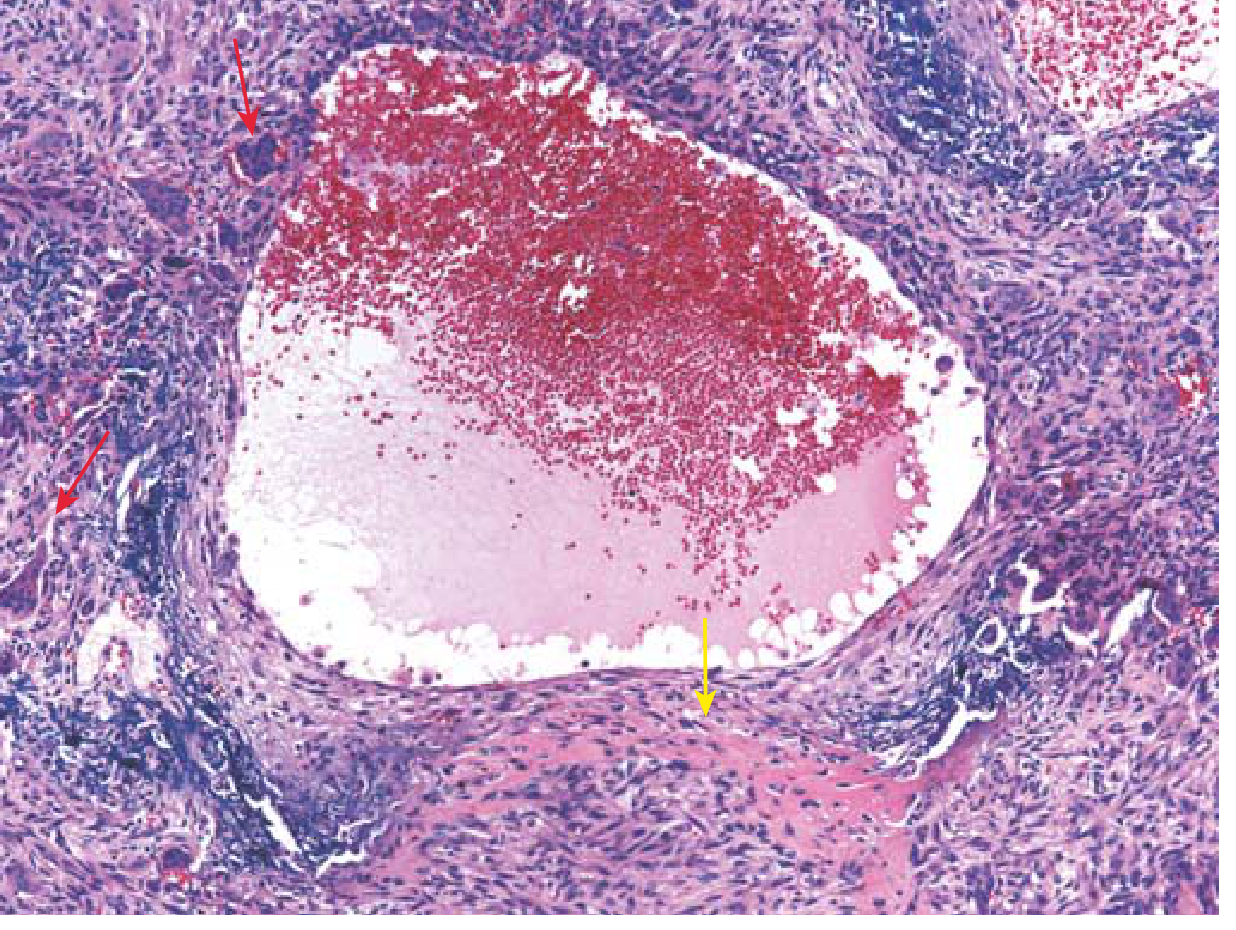
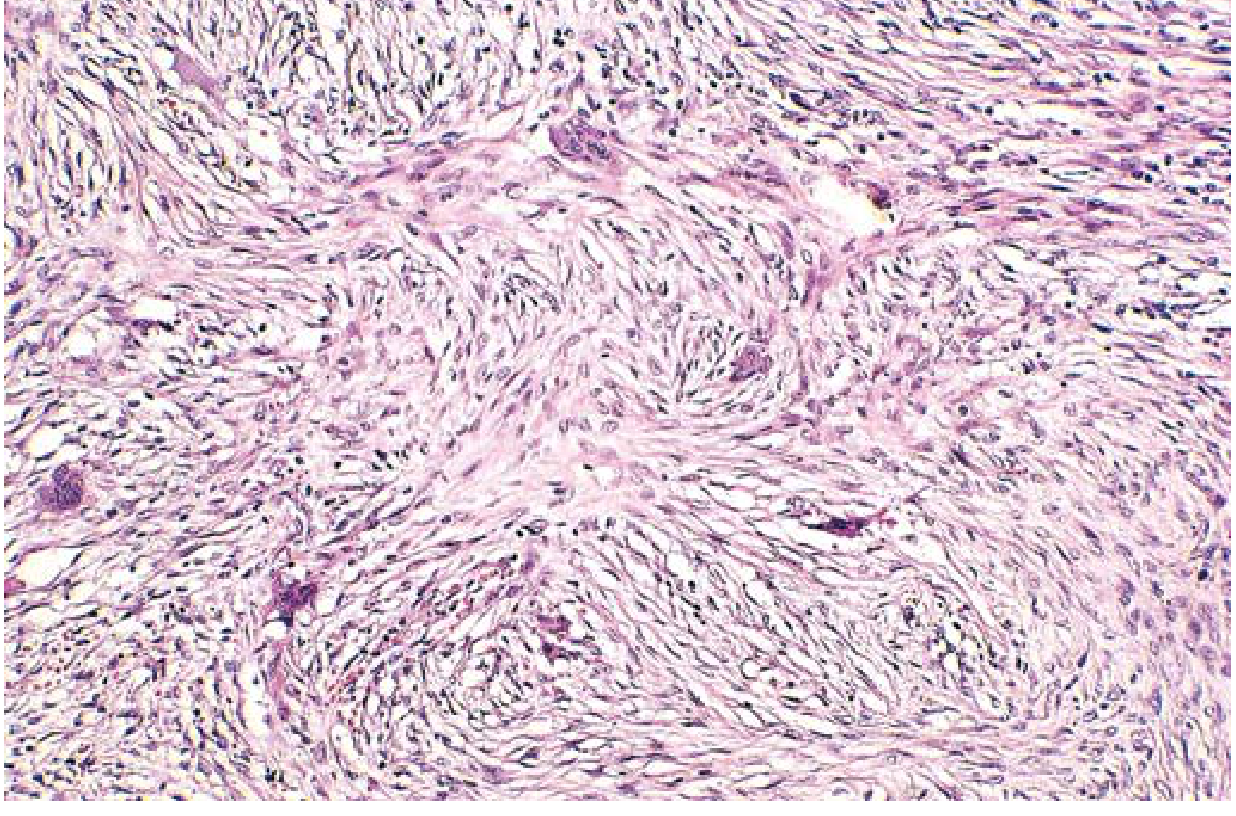
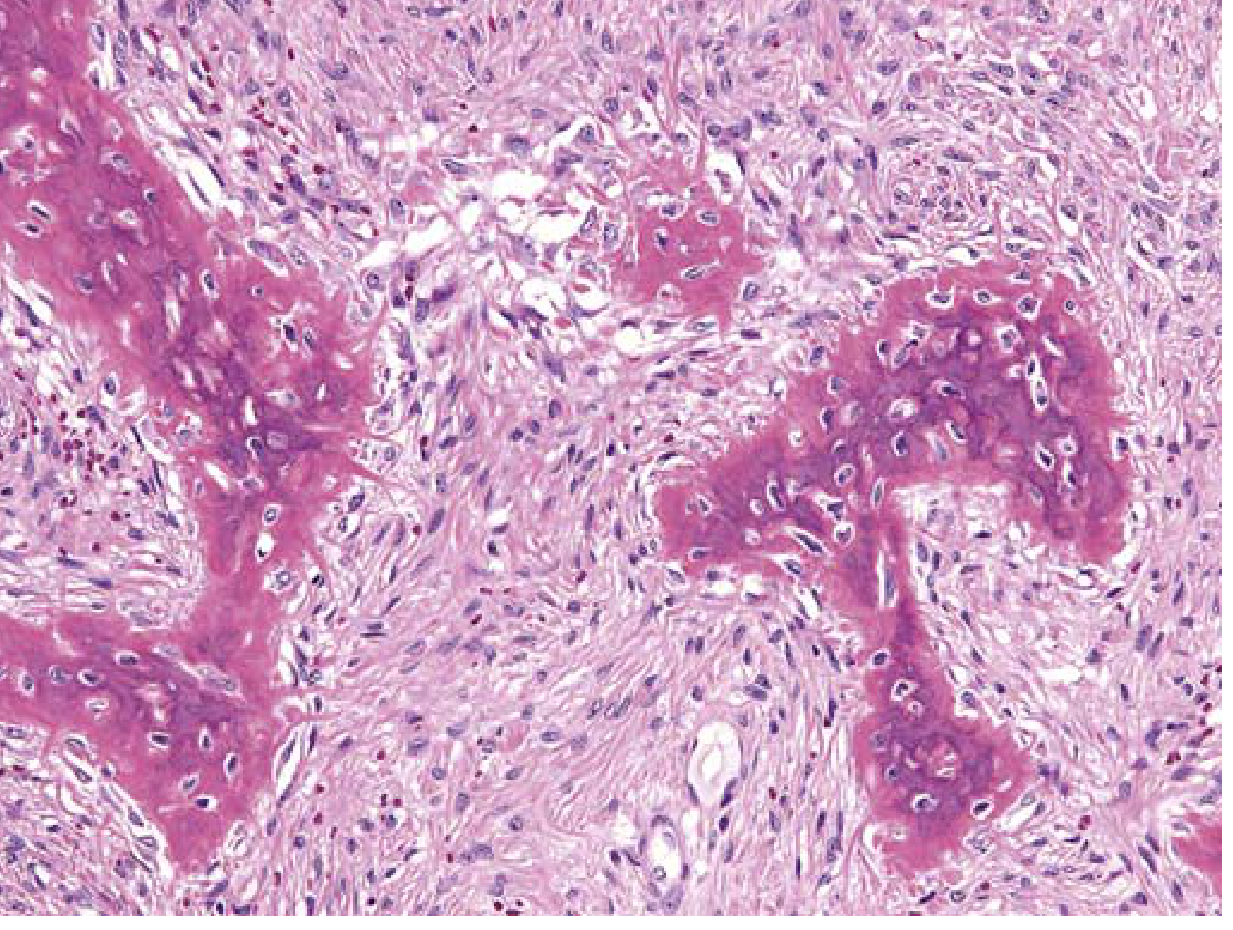
Histology
- Multiple blood-filled cystic spaces separated by thin, tan-white septa
- Septa lack endothelial lining; composed of plump fibroblasts, osteoclast-like multinucleate giant cells, and reactive woven bone
Treatment
- Curettage or excision; recurrence 10-50%
- Adjuvant modalities: cryotherapy, cauterization, selective arterial embolization
- Denosumab (anti-RANKL) used in unresectable cases
Comparison: ABC vs. UBC
| Feature | ABC | UBC |
|---|---|---|
| Age | Any; adolescence | <20 years |
| Location | Eccentric metaphysis | Central metaphysis |
| Width | Wider than physis | Same as physis |
| MRI | Fluid-fluid levels | Uniform fluid |
| Septa | Present (thin trabeculae) | Absent or few |
| Histology | Giant cells, no endothelium | Fibrous lining, giant cells |
3. Fibrous Cortical Defect and Nonossifying Fibroma
Epidemiology
- Fibrous cortical defects (FCD) are found in up to 50% of children >2 years old - one of the most common developmental anomalies
- Majority arise eccentrically in the metaphysis of distal femur and proximal tibia; nearly half are bilateral or multiple
- Lesions >5-6 cm are classified as nonossifying fibromas (NOF)
Radiology
- Sharply demarcated, eccentric lobulated radiolucency surrounded by a thin rim of sclerosis
- This appearance is sufficiently specific that biopsy is rarely needed

Histology
- Gray to yellow-brown lesions with cytologically bland fibroblasts arranged in a storiform (pinwheel) pattern
- Macrophages with foamy cytoplasm and multinucleate giant cells
- Hemosiderin commonly present
Clinical Course & Treatment
- Most small lesions resolve spontaneously within several years
- Progressively enlarging lesions may cause pathologic fracture - require biopsy to exclude other tumors
- Treatment: curettage ± bone grafting
4. Fibrous Dysplasia
Definition & Classification
- A benign condition resulting from a localized developmental arrest - all bone components are present but fail to differentiate into mature structures
- Sporadic or syndromic; arises during skeletal development
Forms:
| Form | Features |
|---|---|
| Monostotic | Single bone; most common (~70-80%) |
| Polyostotic | Multiple bones |
| McCune-Albright syndrome | Polyostotic FD + café-au-lait skin pigmentation + endocrine abnormalities (precocious puberty) |
| Mazabraud syndrome | Fibrous dysplasia + soft tissue myxoma |
Pathogenesis
- All forms result from somatic gain-of-function mutations in GNAS1 (also mutated in pituitary adenomas)
- Mutations produce a constitutively active Gs-protein → elevated cAMP → cellular proliferation + disrupts osteoblast differentiation
- Phenotype depends on the embryonic stage when mutation is acquired
Radiology
- Intramedullary lytic lesions that may expand, causing bowing and cortical thinning
- Classic appearance: "ground-glass" opacity on X-ray (hazy, like frosted glass)
- Shepherd's crook deformity of the proximal femur in polyostotic disease
- Periosteal reaction is usually absent
Histology
- Curvilinear ("Chinese letters" or "alphabet soup") trabeculae of woven bone without a rim of osteoblasts (absence of osteoblastic rimming is a key distinguishing feature)
- Surrounded by moderately cellular fibroblastic proliferation
- Cystic degeneration, hemorrhage, and foamy macrophages common
Clinical Features & Treatment
- Monostotic: often stops enlarging at growth plate closure; may cause pain and fracture
- Polyostotic: progressive deformities and fractures into adulthood; bisphosphonates reduce pain severity
- Rare complication of polyostotic FD: malignant transformation to sarcoma (~1%; osteosarcoma most common)
5. Langerhans Cell Histiocytosis (LCH) / Eosinophilic Granuloma
LCH of bone presents as three clinical entities:
| Entity | Features |
|---|---|
| Eosinophilic granuloma (monostotic LCH) | Single bone or multiple bones; most common form |
| Hand-Schüller-Christian disease | Polyostotic + visceral disease (classic triad: skull lesions, diabetes insipidus, exophthalmos) |
| Letterer-Siwe disease | Polyostotic + visceral disease in infants; most aggressive |
Presentation
- Pain and swelling; any bone may be involved
- Vertebral involvement → vertebra plana (marked vertebral body flattening)
Radiology
- Lytic lesion with well-defined "punched out" margins
- Cortex may be destroyed with periosteal reaction - can simulate a malignant tumor
- Different degrees of cortical destruction may give a "bone within a bone" appearance
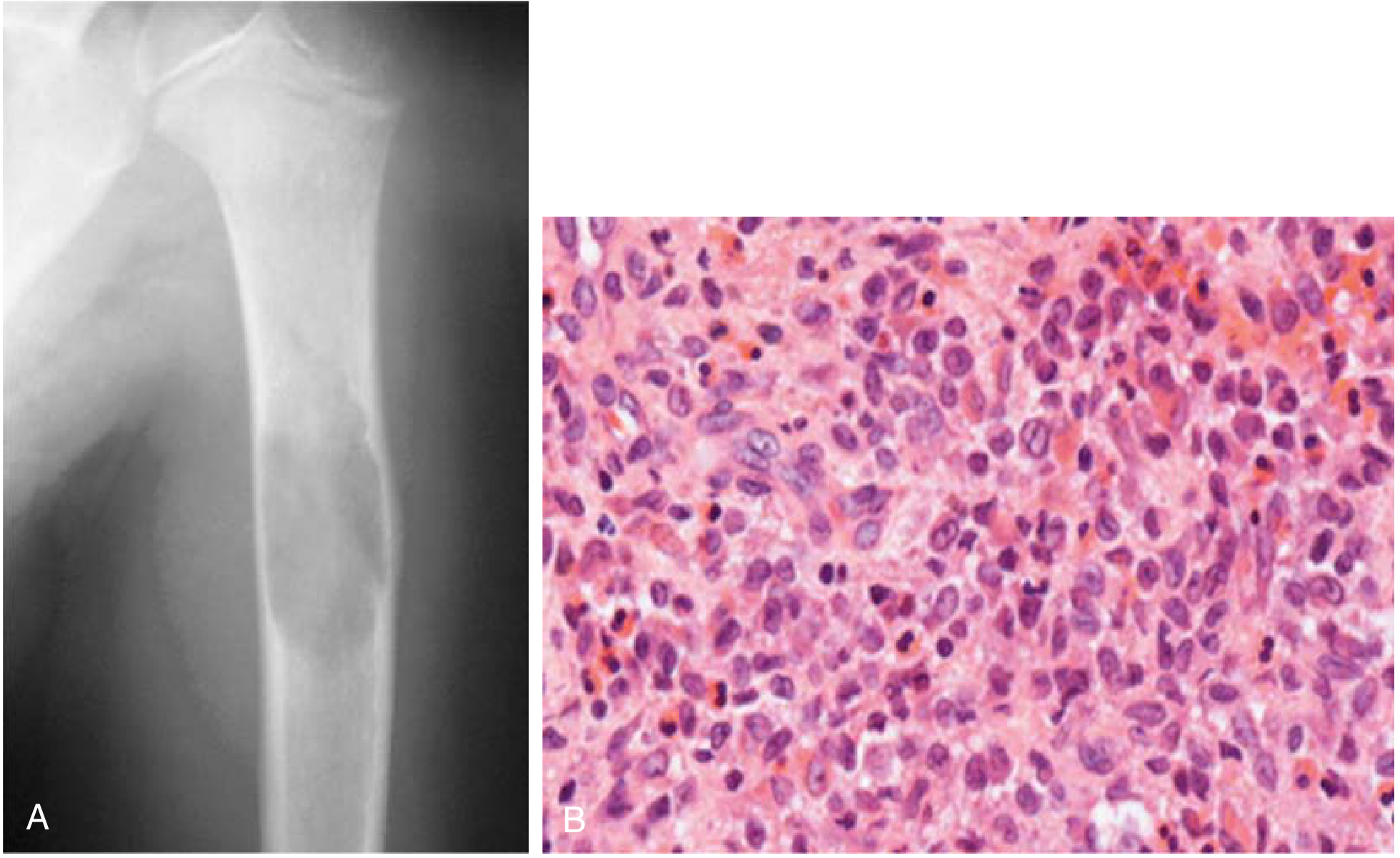
Histology
- Characteristic cell: Langerhans cell - large histiocyte with indented/grooved ("coffee-bean") nucleus, eosinophilic cytoplasm
- Large numbers of bilobed eosinophils with bright granular cytoplasm
- EM: Birbeck granules (tennis-racket shaped) in Langerhans cells
- IHC: CD1a positive, S-100 positive
Treatment
- Monostotic EG: intralesional steroid injection, curettage, low-dose radiation, or observation
- Polyostotic/systemic: chemotherapy (vinblastine + prednisolone is standard)
6. Intraosseous Ganglion
- A mucin-filled cystic lesion within bone (carpus most common, especially lunate)
- Histology: mucoid degeneration of fibrous tissue, no epithelial lining
- Treatment: curettage and bone grafting
Quick Reference Summary Table
| Lesion | Age | Location | X-ray | Key Histology |
|---|---|---|---|---|
| Simple Bone Cyst | <20 yrs | Proximal humerus, proximal femur | Central, metaphyseal lytic; no wider than physis; fallen leaf sign | Thin fibrous lining, giant cells, hemosiderin |
| ABC | Adolescence | Femur, tibia, vertebral posterior elements | Eccentric, expansile, wider than physis; fluid-fluid levels on MRI | Blood-filled spaces, no endothelium, giant cells, reactive woven bone |
| Fibrous Cortical Defect / NOF | Children/adolescents | Distal femur metaphysis (eccentric) | Eccentric lobulated radiolucency + sclerotic rim | Storiform fibroblasts, foamy macrophages, giant cells, hemosiderin |
| Fibrous Dysplasia | Childhood/young adults | Any bone; ribs, femur, skull common | Ground-glass opacity; shepherd's crook deformity | Woven bone "Chinese letters" WITHOUT osteoblastic rimming; fibrous stroma |
| EG/LCH | Children (5-10 yrs) | Any bone; skull, long bones, vertebra | Punched-out lytic lesion; vertebra plana | Langerhans cells (grooved nucleus), eosinophils; CD1a+, Birbeck granules |
Sources: Robbins & Kumar Basic Pathology, pp. 787-789; Miller's Review of Orthopaedics 9th Ed., pp. 849-851; Schwartz's Principles of Surgery 11th Ed., p. 1984
This is a shared conversation. Sign in to Orris to start your own chat.