Wrist block with diagram in detail
Reading File
Finding Sources
Searching the Web
wrist block regional anesthesia anatomy nerves technique diagram
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
I now have everything needed for a comprehensive, well-illustrated answer. Here it is:
Wrist Block - Detailed Guide with Diagrams
Overview
A wrist block is a peripheral nerve block technique that provides anaesthesia to the hand and all digits by blocking the three major terminal nerves of the upper limb at the level of the wrist. It is preferred over a nerve block at the elbow because it carries less risk of direct nerve injury and provides a more reliable field of anaesthesia for hand surgery.
Nerves blocked:
- Ulnar nerve (+ its dorsal cutaneous branch)
- Median nerve
- Radial nerve (superficial branch - subcutaneous ring)
Sensory Innervation of the Hand
Before performing the block, understanding which nerve covers which territory is essential:
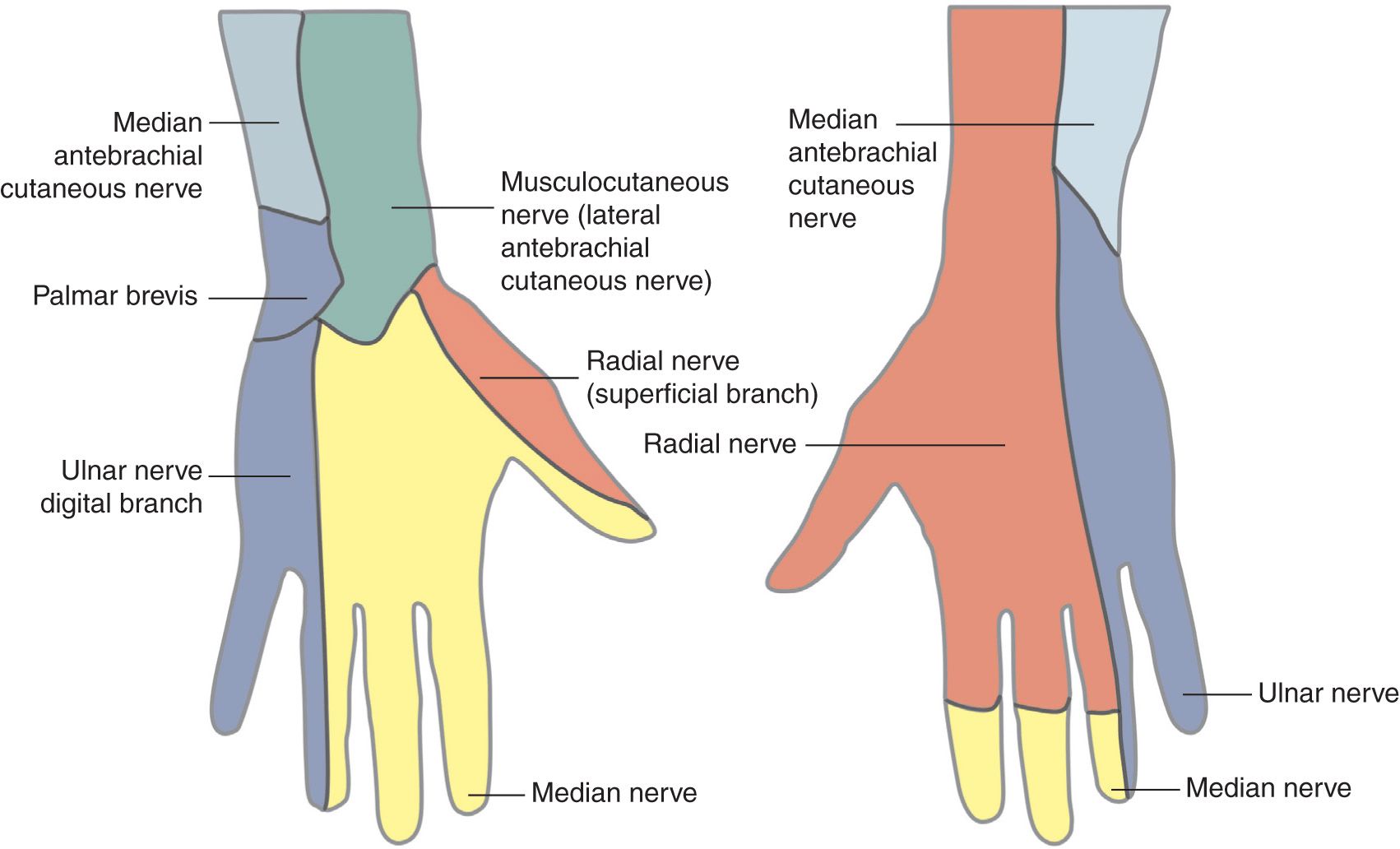
| Surface | Nerve | Territory |
|---|---|---|
| Palmar | Median | Thumb, index, middle, and radial half of ring finger |
| Palmar | Ulnar | Little finger and ulnar half of ring finger |
| Dorsal | Radial (superficial) | Dorsum of thumb, index, middle, and radial ring finger (proximal phalanges) |
| Dorsal | Ulnar (dorsal cutaneous branch) | Dorsum of little and ulnar ring finger |
Anatomy of the Nerves at the Wrist
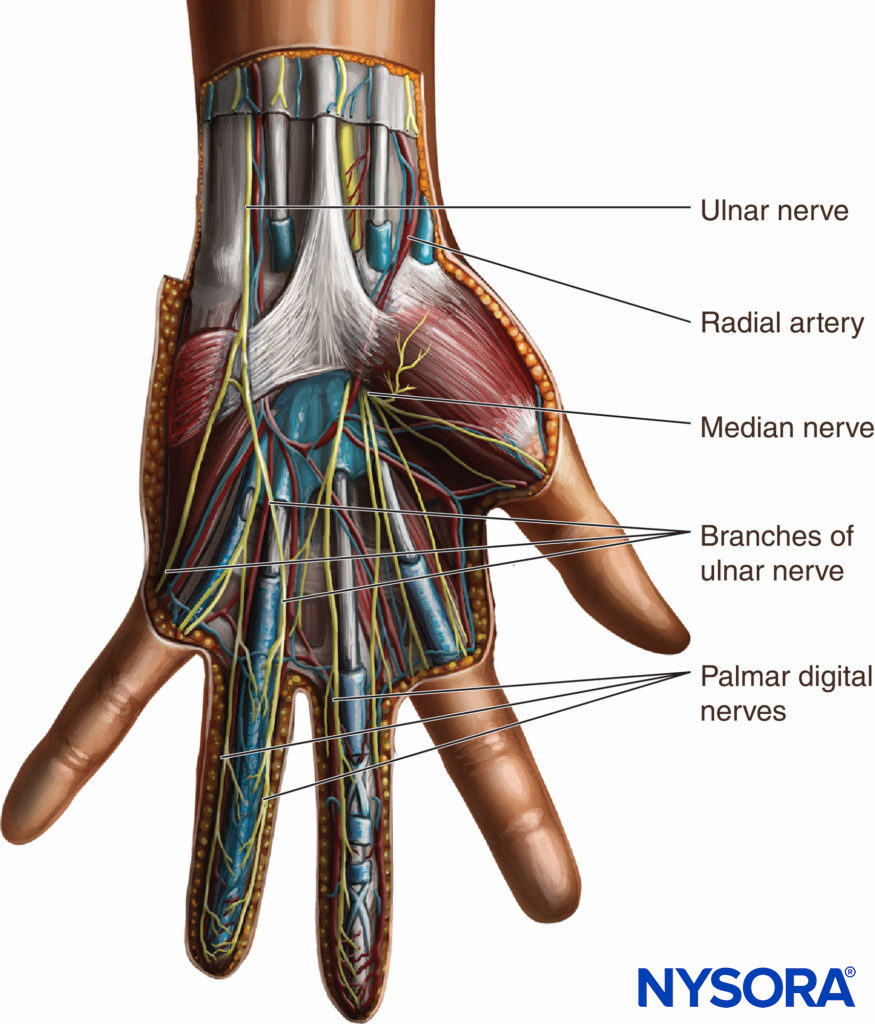
Ulnar Nerve
- Runs between the flexor carpi ulnaris (FCU) tendon (medially) and the ulnar artery (laterally)
- Lies deep to the FCU at the wrist crease
- Gives off the dorsal cutaneous branch about 5-7 cm proximal to the pisiform, which curves around the ulna to supply the dorsal-ulnar hand
Median Nerve
- Lies between the tendons of palmaris longus (PL) and flexor carpi radialis (FCR)
- If PL is absent (in ~15% of people), it lies just to the ulnar side of FCR
- Passes under the flexor retinaculum through the carpal tunnel
Radial Nerve (Superficial Branch)
- Purely sensory at the wrist
- Divides into multiple small branches as it crosses the anatomical snuff box
- No single injection point is reliable - requires a subcutaneous ring infiltration
Injection Level and Landmarks
All three injections are performed at the same level: the proximal wrist crease, approximately at the level of the distal end of the ulna.
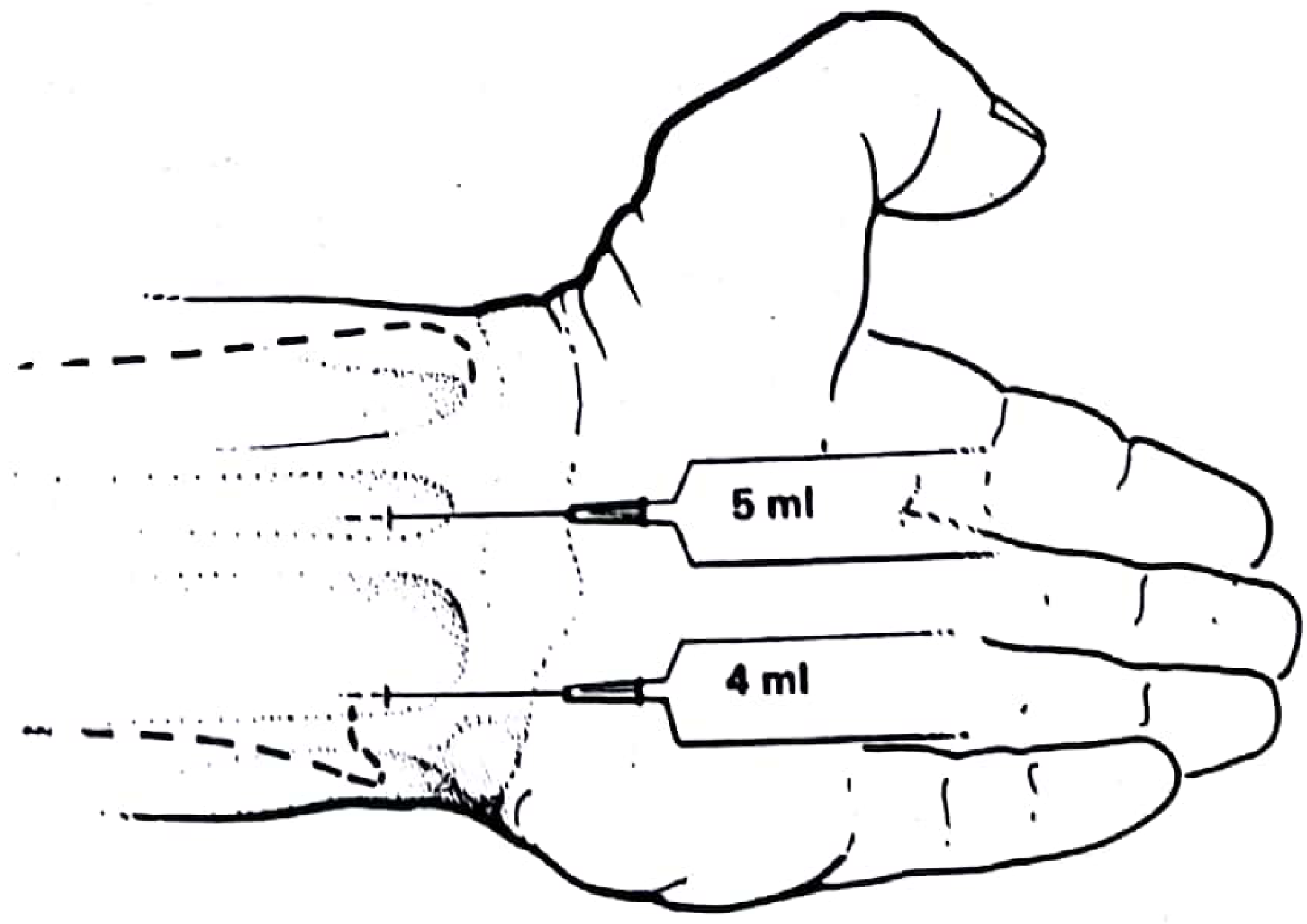
Figure 8.3 from Pye's Surgical Handicraft (22nd Ed.) - Wrist block, palmar (front) view. Upper needle (5 ml) = median nerve; lower needle (4 ml) = ulnar nerve.
Technique - Step by Step
Patient Position
- Arm supinated, wrist extended slightly (a small roll under the wrist helps)
- Identify key surface landmarks: FCU, FCR, palmaris longus, pisiform, ulnar styloid, radial styloid
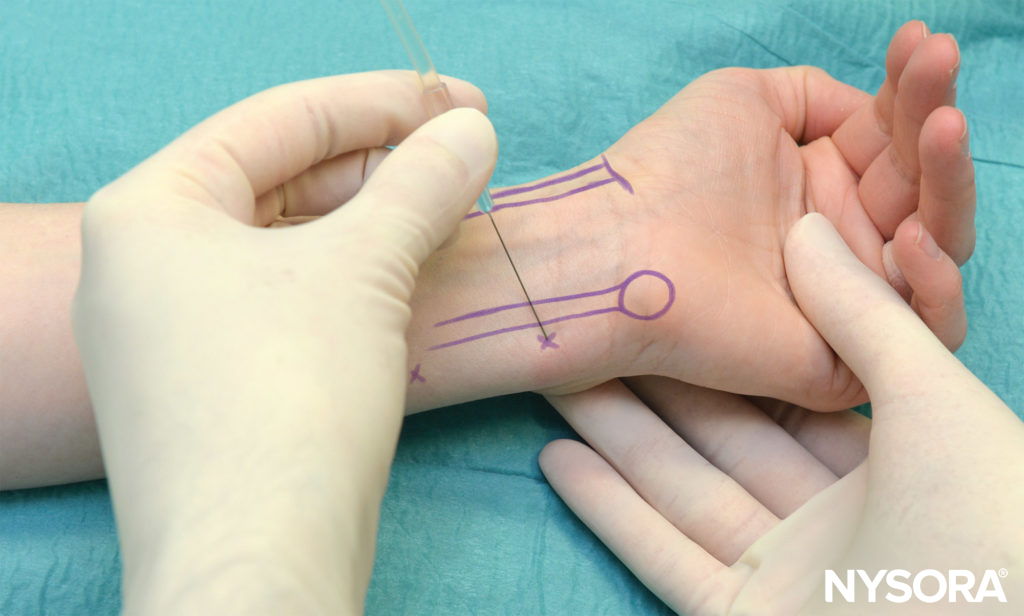
1. Ulnar Nerve Block
Landmarks: FCU tendon at the level of the distal ulna, immediately radial (lateral) to it. The ulnar artery lies just radial to the nerve.
Technique:
- Insert a 25 G needle to a depth of 1 cm, immediately to the radial side of FCU
- Aspirate to confirm no vascular placement
- Inject 4 ml of 1% lignocaine (or equivalent)
Dorsal branch of ulnar nerve: Also requires a separate subcutaneous injection - inject local anaesthetic between the proximal edge of the pisiform and the middle of the dorsum of the wrist, sweeping across the ulnar border subcutaneously.
2. Median Nerve Block
Landmarks: Same level as the ulnar block, in the midline of the wrist between PL and FCR tendons.
Technique:
- Insert a 25 G needle between the tendons of palmaris longus and flexor carpi radialis to a depth of 1 cm
- If PL is absent, inject 3 mm to the ulnar side of FCR (this point sits close to the wrist midline or just slightly to the radial side)
- Aspirate, then inject 5 ml of 1% lignocaine
Do NOT inject if strong paresthesia is felt - reposition the needle to avoid intraneural injection.
3. Radial Nerve Block (Subcutaneous Ring)
Because the superficial radial nerve divides into multiple small branches near the wrist with considerable anatomical variation, a single-injection technique is unreliable.
Technique:
- Inject up to 10 ml of 1% lignocaine subcutaneously in a fan/ring around the entire radial border of the wrist
- The injection arc extends from the middle of the dorsum, sweeping around the radial side, to the middle of the palmar surface - a semicircle that covers all branch points
Figure 8.4 from Pye's Surgical Handicraft - Wrist block (back). Dotted line represents the subcutaneous injection arc for the radial nerve.
Drugs and Doses Summary
| Nerve | Volume | Drug | Depth |
|---|---|---|---|
| Ulnar | 4 ml | 1% lignocaine | 1 cm deep to FCU |
| Median | 5 ml | 1% lignocaine | 1 cm deep, between PL & FCR |
| Radial | Up to 10 ml | 1% lignocaine | Subcutaneous ring, radial border |
| Dorsal ulnar | 2-3 ml | 1% lignocaine | Subcutaneous, pisiform to dorsal midline |
Total volume: ~20-22 ml of 1% lignocaine. Bupivacaine 0.25-0.5% can be substituted for longer duration (4-8 hours).
Area of Anaesthesia
This triple block (with dorsal ulnar coverage) provides analgesia of:
- All digits (fingers and thumb)
- The whole hand
Exception: The proximal 1-2 cm of the palmar aspect of the hand immediately distal to the wrist joint may not be covered (this area is supplied by the palmar cutaneous branches of median and ulnar nerves, which arise proximal to the wrist crease).
Indications
- Minor hand surgery (tendon repair, wound closure, foreign body removal)
- Finger fracture reduction
- Emergency hand procedures when a tourniquet will be applied at the forearm level
- Carpal tunnel release (supplementary to local infiltration)
- Burns/wound debridement of the hand
Contraindications
- Infection at injection site
- Patient refusal
- Known allergy to local anaesthetic agent
- Significant coagulopathy (relative)
Advantages over Elbow Block
- Lower risk of direct nerve injury (ulnar nerve is superficial and at risk at the elbow)
- More predictable block distribution
- No motor block of forearm flexors
- Suitable for outpatient/day-case procedures
Tips and Pitfalls
- Always block the dorsal branch of the ulnar nerve separately - forgetting it leaves the dorsal-ulnar hand unsensate
- Do NOT use vasoconstrictors (epinephrine) in the local anaesthetic for wrist blocks as there is some risk of digital ischemia through vascular reflex
- Onset takes 10-20 minutes - allow adequate time before starting surgery
- If paresthesia is elicited with needle placement, withdraw slightly before injecting to avoid intraneural injection
Source: Pye's Surgical Handicraft, 22nd Edition, Chapter 8 - Nerve block at the wrist; NYSORA Wrist Block Guidelines
This is a shared conversation. Sign in to Orris to start your own chat.