How does seatbelt cause mesenteric avulsion due to sudden deaccleration
Reading File
Finding Sources
Finding Sources
Searching PubMed
seatbelt mesenteric injury deceleration mechanism
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching the Web
seatbelt mesenteric avulsion mechanism sudden deceleration anatomy
Reading Article
PMID: 25408251
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC3200117
Loading Image
I now have everything needed for a comprehensive, well-sourced answer.
Seatbelt-Induced Mesenteric Avulsion in Sudden Deceleration
The Core Biomechanical Problem
When a vehicle decelerates suddenly, the seatbelt arrests the torso while the abdominal viscera - which have inertia - continue moving forward. This creates two simultaneous mechanical forces that together cause mesenteric avulsion:
- Direct compression - the lap belt crushes the bowel between itself and the posterior abdominal wall / lumbar vertebrae
- Shear/traction at mesenteric attachment points - the forward momentum of the bowel tears it away from its fixed mesenteric root
Step-by-Step Mechanism
Phase 1 - Impact
At the moment of collision, the lap belt (particularly when incorrectly positioned over the abdomen rather than across the pelvis/pelvic girdle) acts as a fulcrum. The upper body jackknifes forward over the belt, concentrating enormous compressive force across the mid-abdomen.
Phase 2 - Visceral inertia and forward displacement
The small bowel is not rigidly fixed - it has several metres of length loosely suspended in the peritoneal cavity. As the torso is suddenly halted, the small bowel loops continue their forward trajectory. The bowel is constrained only at two anatomical points of relative fixation:
- The ligament of Treitz (duodenojejunal flexure) - the proximal anchor
- The ileocaecal junction - the distal anchor
The jejunum just beyond the ligament of Treitz is therefore the most vulnerable segment, as it is the first mobile segment yanked away from a fixed point.
Phase 3 - Mesenteric shear
The mesentery is a folded, fan-shaped peritoneal sheet connecting the small bowel to the posterior abdominal wall. Its root runs obliquely from the duodenojejunal flexure (upper left) to the right iliac fossa (lower right) - approximately 15 cm long - but it suspends ~6 metres of bowel. Within this root lie the superior mesenteric artery (SMA) and superior mesenteric vein (SMV), along with their branches.
As the bowel is thrown forward and the mesentery is stretched beyond its tensile limit, three types of failure can occur:
- Avulsion from the mesenteric root - the bowel tears away from the posterior attachment, disrupting the vascular pedicle (SMA/SMV branches)
- Mesenteric laceration - a radial split within the mesentery, transecting blood vessels
- Bowel wall haematoma or perforation - from direct crush of the bowel wall between belt and spine
The ileum and jejunum are particularly at risk via their mesenteric attachment to the posterior abdominal wall, which contains the superior mesenteric vessels. When the seatbelt stops the torso, the small bowel continues to move forward until its mesenteric attachment brings it to a halt - causing shearing of the mesentery and damage to the SMA, resulting in small bowel devascularisation. (PMC3200117)
Biomechanical note: Studies on porcine mesentery-small bowel specimens show that under dynamic loading (100 mm/s - approximating crash deceleration), the ultimate failure force is ~35 N and stiffness increases compared to slow loading, suggesting a strain-based failure threshold regardless of loading rate. At crash velocities, the mesentery fails rapidly and unpredictably. (Bège et al., Med Biol Eng Comput 2015, PMID 25408251)
Why the Lap Belt is the Key Risk Factor
A correctly worn three-point belt distributes force across the chest and pelvis, limiting abdominal compression. The problem arises with:
- Lap belt alone (2-point restraint, older vehicles)
- Incorrectly worn lap portion - positioned over the soft abdomen rather than the anterior superior iliac spines
When positioned too high (over the abdomen), the belt acts as a direct compressive force on the bowel AND creates a pivot point over which the torso flexes violently.
The Seatbelt Injury Complex (Classic Triad)
Three injuries that commonly occur together:
| Injury | Mechanism |
|---|---|
| Abdominal wall ecchymosis ("seatbelt sign") | Direct contusion from belt |
| Hollow viscus / mesenteric injury | Compression + shear as described above |
| Chance fracture (lumbar spine, L1-L3) | Hyperflexion over the belt fulcrum causing distraction fracture of the vertebral body |
The presence of a seatbelt sign increases the risk of intra-abdominal injury requiring intervention more than fivefold. A Chance fracture carries a 50% incidence of associated intra-abdominal injury. (Tintinalli's Emergency Medicine)
Clinical Consequence of Mesenteric Avulsion
- Disruption of SMA/SMV branches leads to bowel ischaemia and devascularisation
- If not recognised promptly, bowel perforation and peritonitis follow
- Mesenteric avulsion is rare (60% of cases in systematic review were seatbelt RTA) but carries 15% mortality (systematic review of 20 cases, PMID 26038032)
- CT may miss the injury initially - serial abdominal examination is essential when seatbelt sign is present
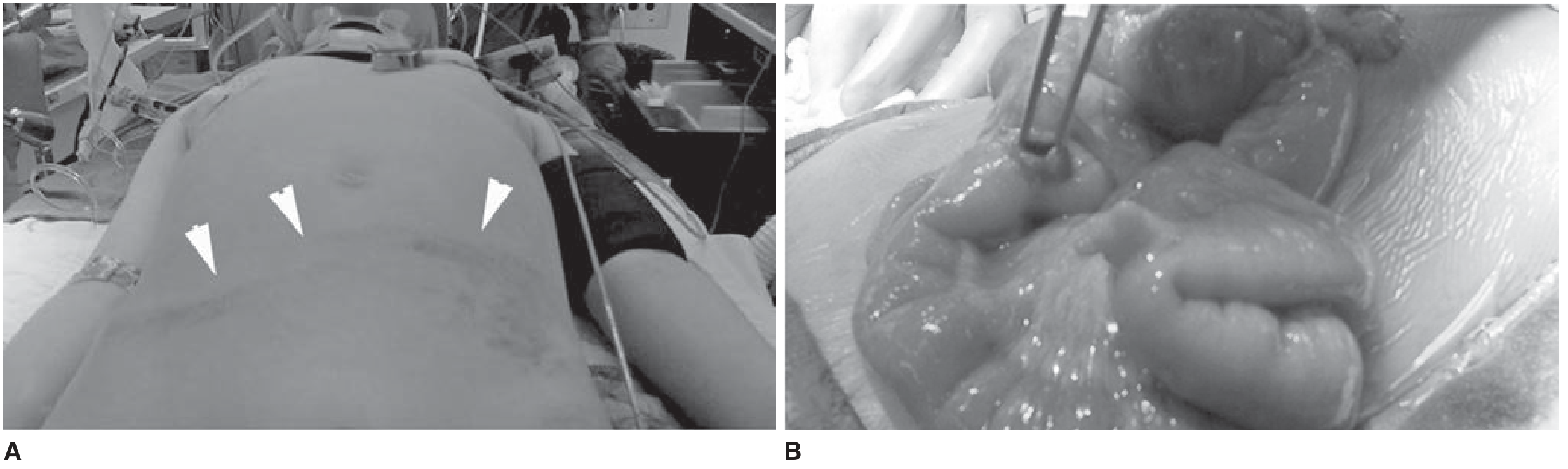
Figure: Left - seatbelt ecchymosis across the anterior abdomen (arrowheads = seatbelt sign). Right - intraoperative view of small bowel perforation/injury found at laparotomy. (Schwartz's Principles of Surgery, 11th ed.)
Summary
The mechanism of mesenteric avulsion is a combination of:
- Compression - bowel crushed between belt and spine
- Inertial shear - bowel thrown forward relative to the fixed mesenteric root, tearing the mesentery and its vascular pedicle (primarily SMA/SMV branches)
- Maximal injury at anatomical fixation points - ligament of Treitz and ileocaecal junction, making the proximal jejunum the most commonly injured segment
Sources:
- Tintinalli's Emergency Medicine: A Comprehensive Study Guide (Hollow Viscus Injury section)
- Schwartz's Principles of Surgery, 11th Ed. (Abdominal Injuries section)
- Bège T et al. "Biomechanical analysis of traumatic mesenteric avulsion." Med Biol Eng Comput 2015. PMID 25408251
- PMC3200117 - Seatbelt Injury Causing Small Bowel Devascularisation (case series + review)
- Systematic review: Blunt abdominal trauma and mesenteric avulsion PMID 26038032
This is a shared conversation. Sign in to Orris to start your own chat.